ICU Snapshots:
60 yo pt, multiple medical problems (including morbid obesity; BMI 50), admitted to the ICU w ARDS in setting of sepsis. Intubated 08/14 (with 👇CXR), improved w VC-CMVs the next day but the same night became very hypoxic, had to be placed on FiO2 100% + PEEP 12
⚠️ Ventilating obese ICU patients is NOT just “standard ARDS with higher pressures.”
It’s a completely different physiology.
🧠 What’s really happening:
Obesity doesn’t just add weight…
It reshapes respiratory mechanics:
▪️ ↑ Pleural pressure
▪️ ↓ Functional residual capacity (FRC)
▪️ ↑ Chest wall elastance
▪️ ↑ Atelectasis + V/Q mismatch
➡️ The lung is smaller, compressed, and harder to keep open
🚫 Big mistake we still see:
👉 Using actual body weight for tidal volume
❌ Leads to overdistension
❌ Increases VILI risk
✔️ Always use:
🎯 Predicted Body Weight (PBW)
→ VT: 6–8 mL/kg PBW
⚡ PEEP is NOT optional here
In obesity:
▪️ High pleural pressure → alveoli collapse easily
▪️ Standard PEEP (5-10) is often insufficient
👉 You need:
✔️ Higher, individualized PEEP
✔️ Guided by:
Transpulmonary pressure
EIT
Driving pressure (with caution)
📉 Critical nuance (many miss this):
👉 High plateau ≠ high lung stress
In obesity:
▪️ Airway pressure = lung + chest wall
▪️ Chest wall is stiff → pressures look falsely high
➡️ You might be undertreating PEEP out of fear
🫁 Airway & intubation = high risk zone
▪️ Rapid desaturation (low FRC)
▪️ Difficult airway more common
✔️ Best approach:
▪️ Ramped position
▪️ NIV or HFNC preoxygenation
▪️ Video laryngoscopy FIRST LINE
🔥 Game-changing mindset shift
Don’t think:
❌ “Obese patient = higher pressures”
Think:
✔️ “Compressed lung that needs recruitment and protection”
💡 Take-home
Obesity ventilation is about:
▪️ Protecting a smaller lung
▪️ Fighting collapse (PEEP)
▪️ Interpreting pressures correctly
▪️ Anticipating airway risk early
📚 Kitisin N et al. (2026)
Intensive Care Medicine
DOI: 10.1007/s00134-026-08397-3
Jueves de Artículo Clásico…
Fórmula para ajustar la paCO2 modificando el Ventilador Mecánico 🫁
Ventilación Minuto necesaria =
PaCO2 medida x Vent Min actual
———————————————
PaCO2 deseado
Si la Vent Min es = FR x Vt
Puedes modificar cualquiera de las 2 o ambos para lograr la paCO2 que deseas (la FR tendrá menor impacto dañino en ARDS o Neurocríticos, tal vez…)
Y funcionará siempre y cuando:
1) el px no haga ventilaciones espontáneas (sedado, por ej)
2) las condiciones metabólicas (producción de CO2) se mantengan estables
3) NO exista obstrucción en la vía aérea (ej, broncoespasmo)
https://t.co/A7rk1xWIwX
This blew my mind.
OpenAI just published the first comprehensive study of how 700 million people actually use ChatGPT.
The results destroy every assumption about AI adoption.
Here's everything you need to know in 3 minutes:
💉🩺Rapid sequence intubation in 2026: we are no longer “protecting the airway.”
We are managing physiology under extreme stress.
The latest evidence challenges one of the oldest dogmas in critical care.
RSI was designed to prevent aspiration.
But today, the real enemy is often hypoxemia and cardiovascular collapse.
1. Aspiration is no longer the central problem
For decades, RSI was built around one fear: aspiration.
But emerging data suggest:
RSI may not significantly reduce aspiration
It may increase hypoxemia and hemodynamic instability
The paradigm is shifting:
👉 From aspiration avoidance → to physiologic optimization
2. First-pass success is everything
Every additional attempt increases:
Hypoxia
Hemodynamic collapse
Mortality
Modern RSI is built around one goal:
Get it right the first time.
That means:
Videolaryngoscopy first-line
Stylet routinely
Team choreography, not improvisation
3. Preoxygenation is now a therapeutic intervention
Not just a step—a determinant of survival
NIV > face mask
HFNO as adjunct
Semi-upright positioning
And one key shift:
👉 Gentle ventilation is no longer taboo
Done correctly, it reduces hypoxemia without increasing aspiration risk.
4. Hemodynamics matter more than ever
Up to 40–50% of patients experience peri-intubation instability.
The modern approach:
Avoid propofol in unstable patients
Favor etomidate or ketamine
Consider prophylactic vasopressors
Fluid loading?
Not routinely beneficial.
5. Cricoid pressure: from dogma to doubt
No clear benefit in preventing aspiration
May worsen laryngoscopy and ventilation
Current thinking:
👉 Use selectively, or not at all
6. RSI is no longer a rigid protocol
It is now:
Patient-specific
Physiology-driven
Team-dependent
With tools like:
Gastric ultrasound
POCUS-guided decisions
Structured airway protocols
7. The real determinant of success: human factors
Preparation, communication, and coordination matter as much as drugs.
Because in critical care:
The airway is not just anatomy.
It is a moment of systemic vulnerability.
🤓Final message
RSI has evolved:
From speed → to precision
From protocol → to physiology
From individual skill → to team performance
And ultimately:
The goal is no longer just to intubate.
It is to intubate without killing the patient.
📃Reference
Boulos NM et al. Anaesth Crit Care Pain Med. 2026. https://t.co/KWUfUtAMyP
💉The 2026 Anaphylaxis Guidelines highlight something uncomfortable for all of us in acute care:
we do not fail because we lack knowledge, but because we fail to act on what we already know.
Across 12 international guidelines, there is almost perfect agreement on one point:
intramuscular epinephrine is the first and most important intervention⚠️. Yet in real practice, it remains significantly underused, often replaced or delayed by antihistamines or corticosteroids, therapies with no evidence for acute life saving benefit
This gap between evidence and behavior is the central clinical problem.
From a bedside perspective, three insights are particularly relevant:
First, diagnosis remains the main bottleneck, not treatment.
The guidelines clearly show that variability in diagnostic criteria, especially in patients without skin manifestations or in infants, leads to hesitation. Clinically, this reinforces a key principle:
-> anaphylaxis is a clinical diagnosis driven by physiology, not by complete textbook criteria. Waiting for skin signs or full multisystem involvement delays epinephrine and worsens outcomes.
Second, the document reframes management from a pharmacologic problem to a systems and education problem.
Underrecognition by clinicians, lack of training in schools and community settings, and poor patient education all contribute to undertreatment. In reality, the success of anaphylaxis management depends less on ICU level interventions and more on early recognition and immediate action in prehospital environments.
Third, there is a clear shift toward proactive risk management rather than reactive treatment.
Modern guidelines emphasize emergency action plans, patient carried epinephrine, and structured education programs. This aligns with a broader trend in critical care: outcomes improve when interventions occur before physiological collapse, not after.
An important nuance for critical care physicians is the role of adjunctive therapies.
Antihistamines and corticosteroids are consistently positioned as SECONDARY, non life saving treatments. Their continued overuse reflects a cognitive bias toward treating visible symptoms rather than addressing the underlying hemodynamic and airway threat. Clinically, this is equivalent to treating hypotension in septic shock with paracetamol.
🤓Bottom line:
Anaphylaxis is one of the clearest examples in medicine where the evidence is simple, but implementation fails.
The priority is not new drugs or devices, but closing the gap between recognition and immediate epinephrine administration.
📃Reference
Wallace DV, Immunol Allergy Clin N Am ▪ (2026) https://t.co/VoarNwD7v7
Point-of-care ultrasonography (#POCUS) is a noninvasive bedside imaging modality used to assess intravascular volume status in hospitalized or emergency department patients with possible #VolumeOverload.
POCUS evaluates the inferior vena cava, internal jugular vein, and lung parenchyma with high-frequency linear, low-frequency phased-array, and low-frequency curvilinear probes.
🧵 1/ First ever AHA/ACC/multi-society guidelines re: diagnosis & management of acute PE released today!
2 year effort with 38 authors from 10 specialties.
Link attached & summary in this thread:
https://t.co/uUUyUvz3pR
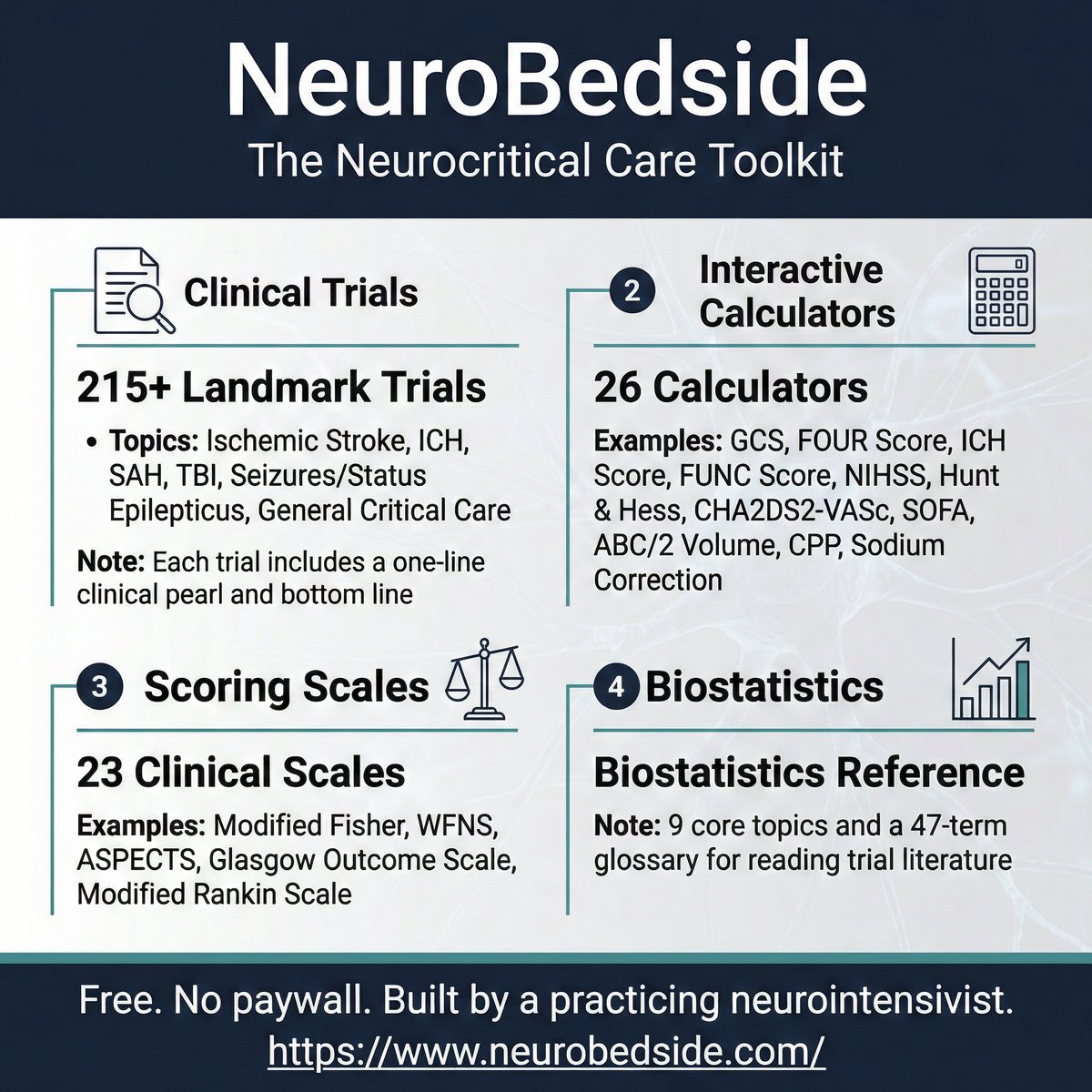
I built a free neurocritical care reference tool called NeuroBedside.
215+ landmark trials with trial details and one-line clinical pearls. 26 interactive relevant medical calculators. details of 23 scoring scales. Biostatistics reference. All in one place, on your phone or computer, at the bedside.
No paywall. No login required to browse.
https://t.co/xyBY0GeNCX
#NeuroCritCare #NeuroTwitter #MedEd #FOAMed #CriticalCare
Consenso Internacional para el Ayuno Perioperatorio
Para que ya dejen de hacer cosas como:
🫤 ayuno después de las 10 pm previo al día de la cirugía
😑 cancelar cirugías por haber tomado agua o té recientemente
😐 y ayuno por 1, 2 o 3 días en el posoperatorio…
https://t.co/pM2FhX3FBd
🫀New and improved version of my hemodynamic simulator to help you understand cardiac PV curves!
You can see the effect of changing preload, afterload, & contractility. You can also add various mechanical circulatory support (MCS) devices: IABP, Impella, and ECMO.
https://t.co/V8IO2pHjIM
🧵
1/
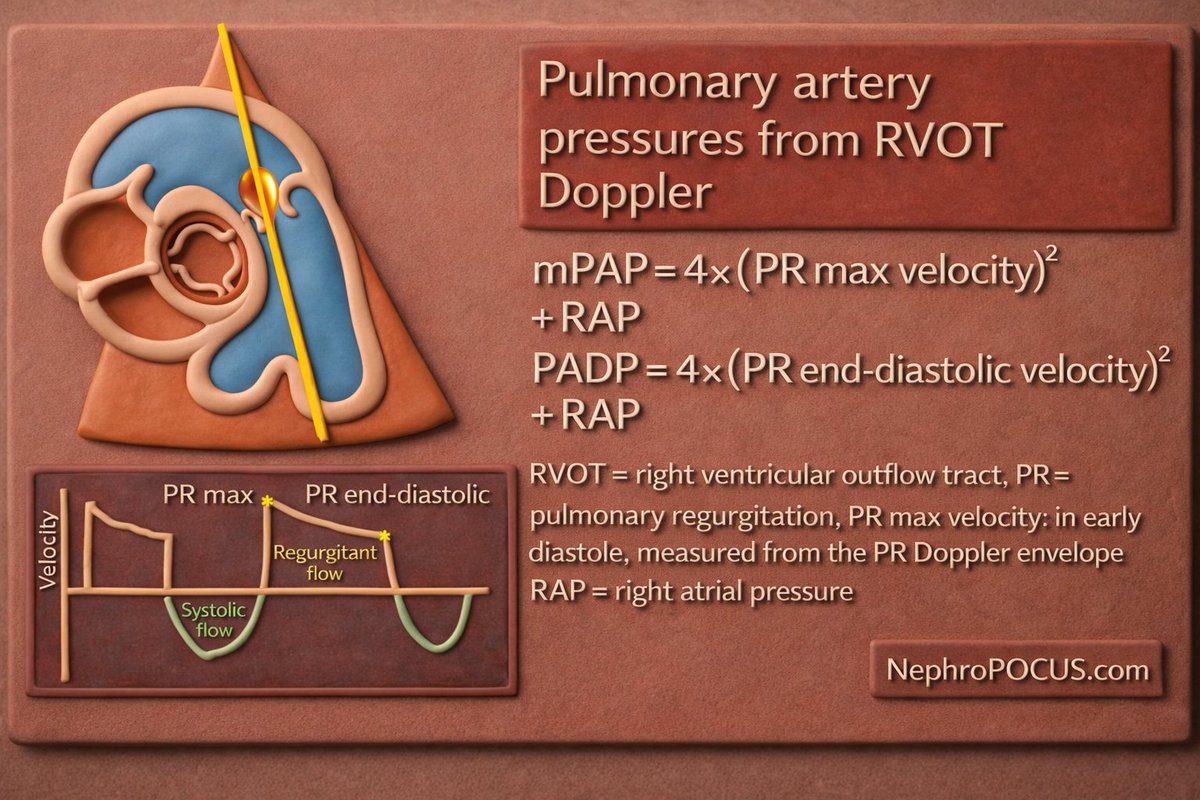
Estimation of mPAP and dPAP on #POCUS#echofirst#FOAMed#Nephpearls
Accuracy depends on a few things:
• A clean, well-defined PR Doppler envelope
• A reasonable RAP estimate (often the weakest link)
In severe PR, PADP can be underestimated as RV and PA pressures equalize late in diastole.
PR-derived mPAP correlates with cath data, but it’s not a substitute for invasive measurements in all settings.
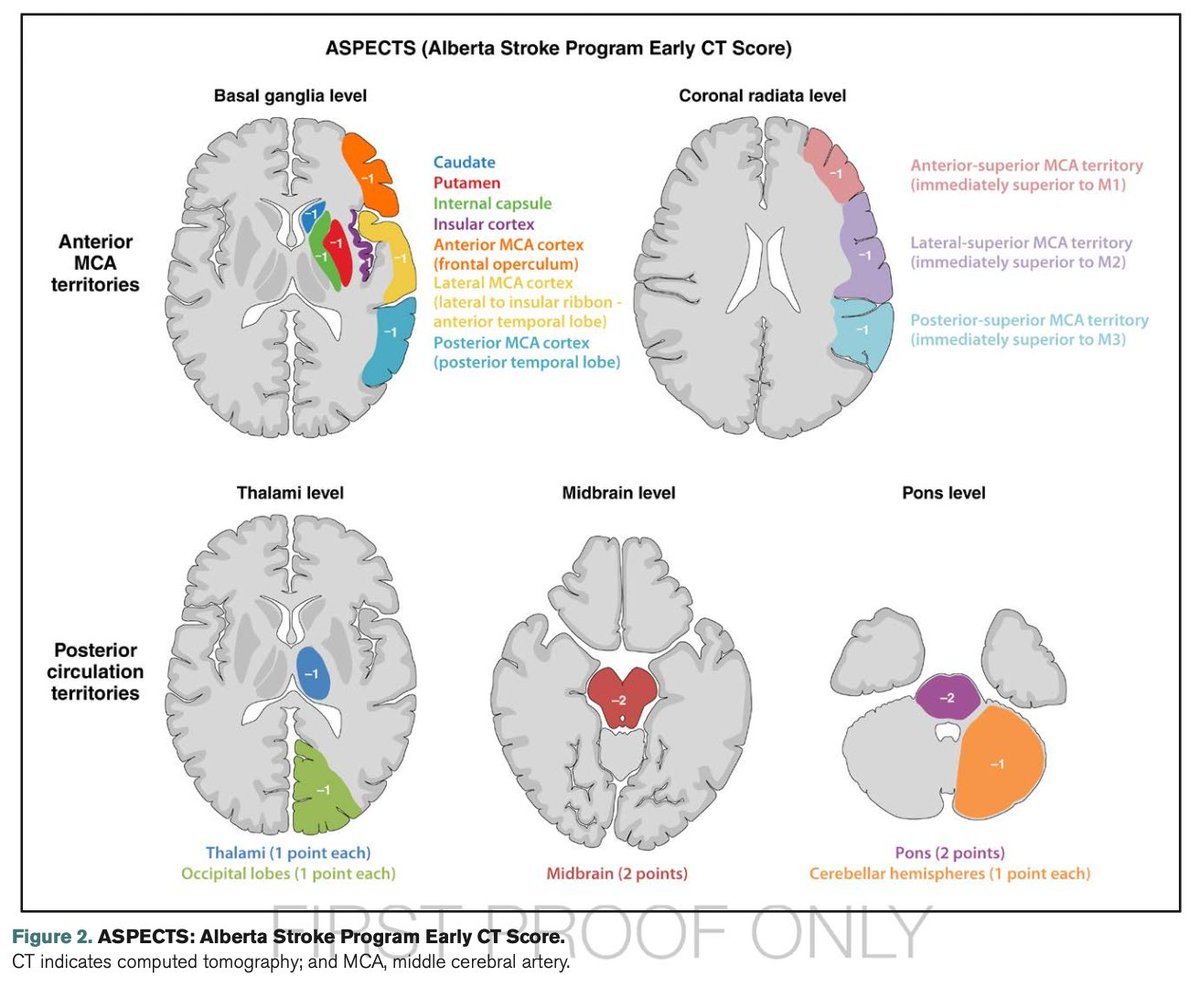
Recién salidas del horno: Guía AHA, 2026, de Evento Vascular Cerebral (EVC) Isquémico. Cambios o puntos relevantes:
🔴 Tenecteplase vs. Alteplase (Cambio Mayor) Se recomienda el uso de Tenecteplase (0.25 mg/kg, bolo único, máx. 25 mg) como una alternativa de primera línea, no inferior a la Alteplase, para pacientes elegibles en la ventana de 4.5 horas. Nota: La dosis de 0.4 mg/kg de Tenecteplase no se recomienda por falta de beneficio adicional y mayor riesgo de seguridad.
🔴 Ictus Leve No Incapacitante: En pacientes con déficits leves que no son incapacitantes (ej. síndrome sensitivo aislado, NIHSS bajo sin impacto funcional) dentro de las 4.5 horas, no se recomienda la trombolisis IV. Se prefiere la doble antiagregación plaquetaria (DAPT).
🔴 Trombectomía (EVT) en "Large Core": Se amplía la indicación de trombectomía mecánica para incluir pacientes con infartos de núcleo isquémico grande establecidos (ASPECTS 3-5), (antes eran excluidos).
🔴 Se desaconseja la reducción intensiva de la PAS (<140 mmHg) tras una reperfusión exitosa. Objetivo: TA <180/105 mmHg en las primeras 24 horas.
🔴 Oclusión de Arteria Basilar: realizar trombectomía en pacientes con oclusión de la arteria basilar a las <24 horas si NIHSS ≥10.
🔴 Control Glucémico: mantener entre 140-180 mg/dL.
🔴 Ventanas Extendidas de Trombolisis: Se recomienda el uso de trombolisis IV en ventana extendida (4.5 a 9 horas o ictus del despertar) en pacientes seleccionados mediante imagen avanzada que demuestre mismatch (DWI-FLAIR o Perfusión).
🔴 Nuevas Guías Pediátricas: Por primera vez se incluyen recomendaciones específicas para pediatría
Vamos a revisarlas a fondo para actualizar las apps.
.@WHAAsstSecty: Las voces de 3.8 millones de hondureños han hablado, y el Consejo Nacional Electoral ha certificado los resultados de las elecciones. Cualquier intento de revertir ilegalmente las elecciones de Honduras tendrá consecuencias graves. La violencia política no tiene cabida en el proceso democrático. El pueblo hondureño merece una transición pacífica del poder. Esperamos trabajar con el presidente electo @titoasfura para avanzar en nuestros objetivos compartidos.
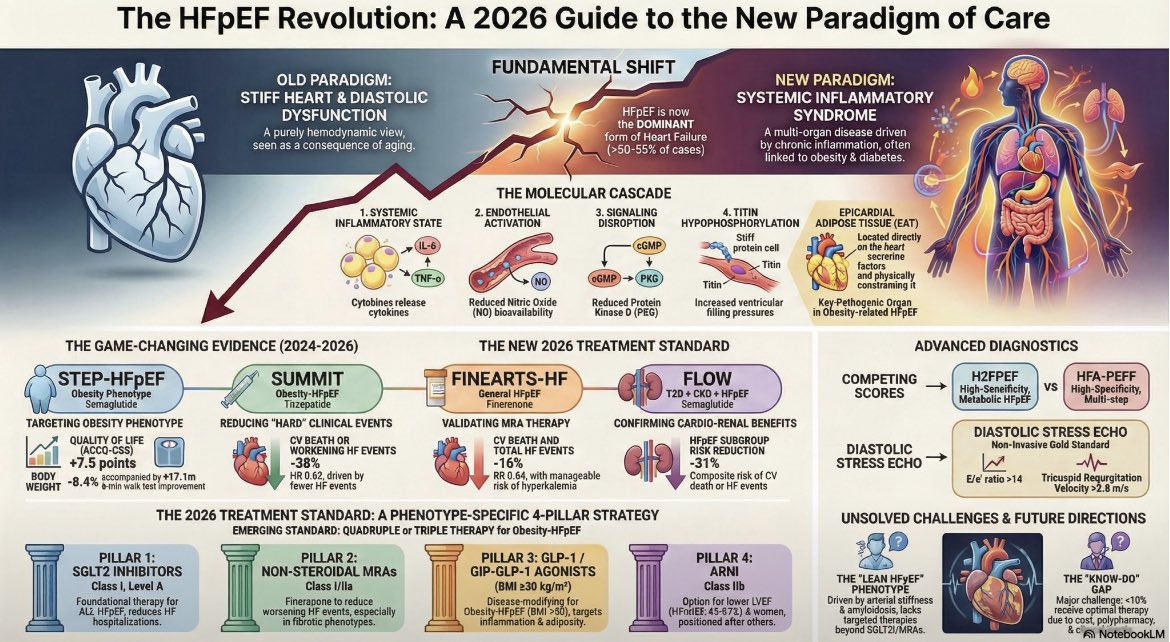
Heart Failure with Preserved Ejection Fraction (HFpEF) is no longer a "black box." It is now the dominant form of Heart Failure, accounting for >50-55% of cases.
This infographic synthesizes the radical shift we have witnessed in the last 24 months:
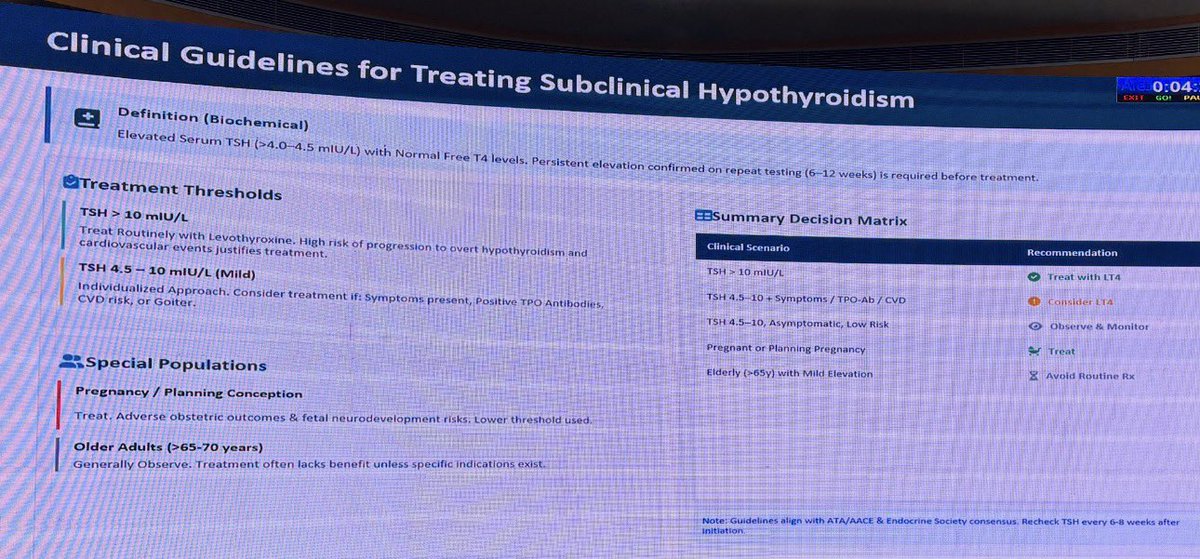
Clinical guidelines for treating subclinical hypothyroidism.
#ISNCON25
You see this often in clinical practice, TSH mildly elevated and free T4 is normal. Should you Rx?
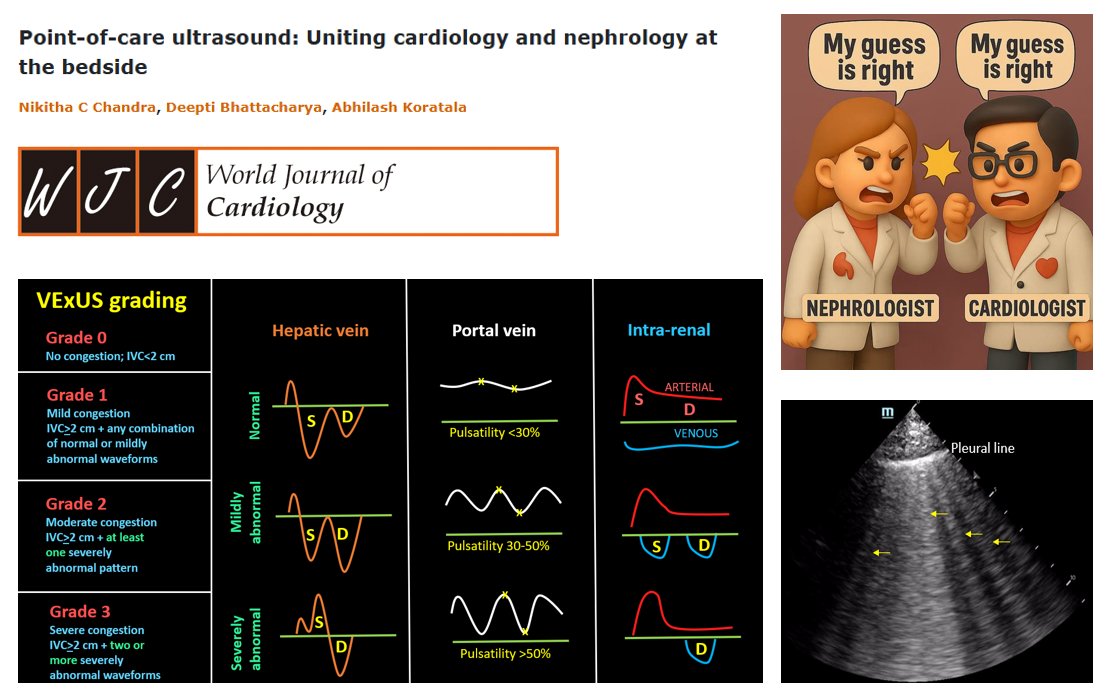
Grateful to be part of this work on #POCUS bringing cardiology and nephrology together at the bedside. #Nephpearls
The first author is a current IM residency #Match2026 applicant and has been a pleasure to work with -thoughtful, hardworking, and dependable throughout.
Program Directors who are still offering interviews should strongly consider her. AAMC ID 16169777 🔗https://t.co/reqC1ERWFc
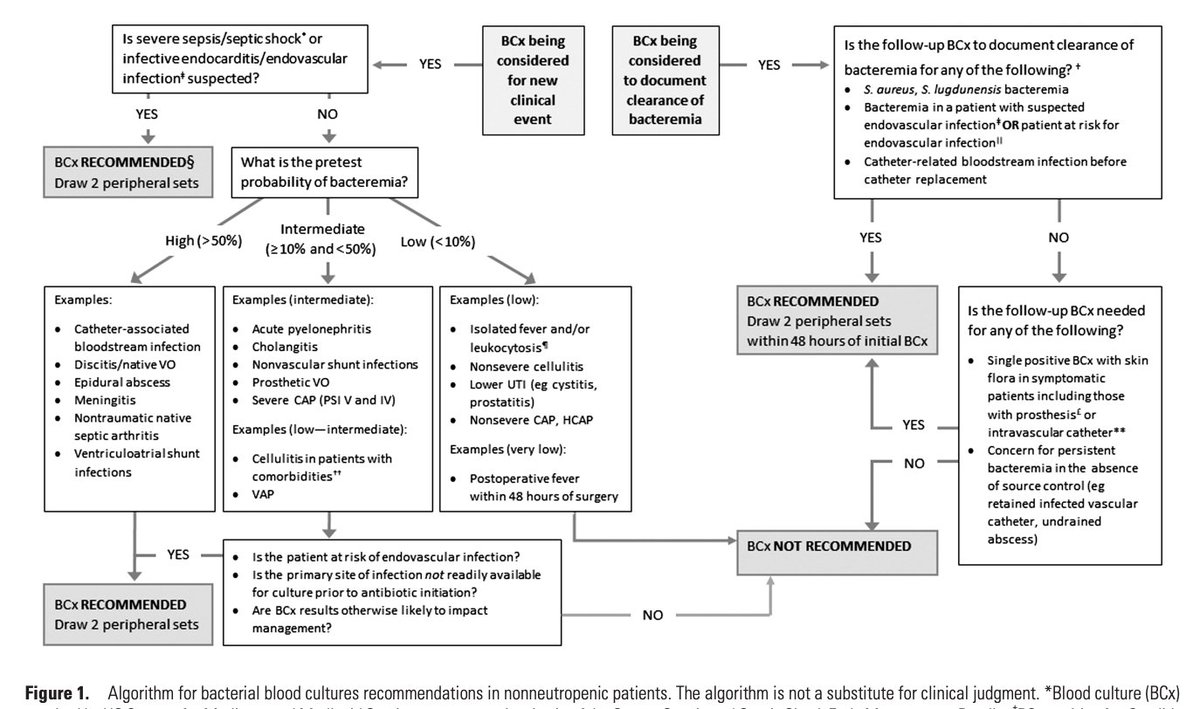
【Does This Patient Need Blood Cultures? A Scoping Review of Indications for Blood Cultures in Adult Nonneutropenic Inpatients】@CIDJournal 2020
👉A key paper highlighting the necessity and optimal timing of blood cultures!
👉Figure 1 and Table 1 are useful!
#IDMedEd#IDFellow
Today I learned the cut off for a normal d-dimer is adjusted by age. Less than 50 yo normal is less than 500. Above that it’s the patient’s age multiplied by 10. So 65 yo normal is less than 650. 80 yo normal is less than 800.