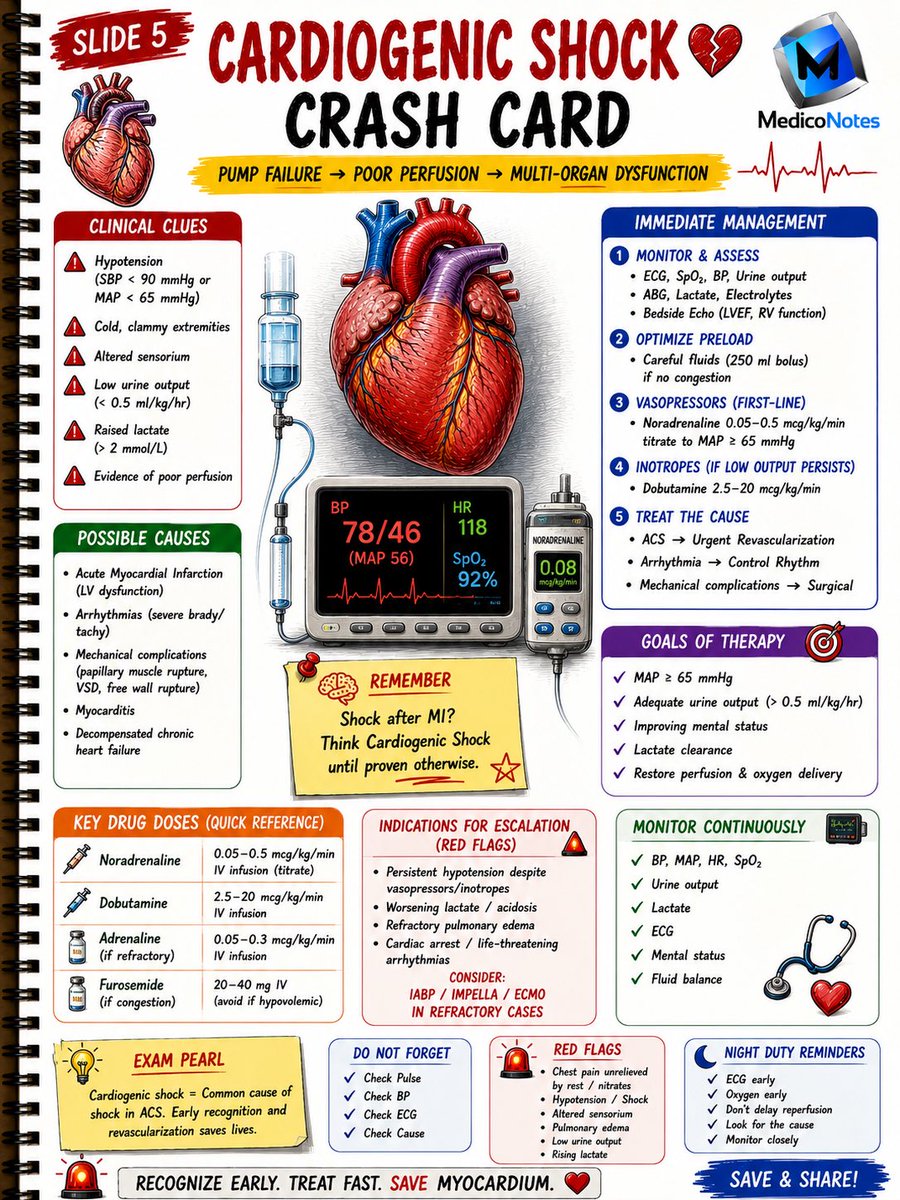
🚨 Not all cardiogenic shock is the same.
In this meta-anaylsis, patients with cardiogenic shock due to AMI or ADHF showed distinct clinical phenotypes and outcomes, highlighting the need for tailored management strategies.
https://t.co/XKz6G42xlY
@EJHFEiC@AmrAbdin10@GiuseppeGalati_@HanCardiomd
#EJHF
Possible rhythms in Wolff-Parkinson-White (WPW) syndrome.
Schematic representation of possible rhythms in a patient with an accessory atrioventricular (AV) bypass tract.
A. During sinus rhythm, the ventricle may be activated by conduction over the accessory pathway (AP) and through the normal AV conduction system. The QRS complex may be narrow if ventricular activation occurs primarily via the AV node, or wide and preexcited if activation occurs mainly through the AP.
B. During orthodromic reentrant tachycardia, antegrade conduction occurs through the AV node and normal conduction system, while retrograde conduction occurs via the AP. The resulting tachycardia shows a narrow QRS complex.
C. In antidromic tachycardia, the AP serves as the antegrade limb of the reentrant circuit, and the AV node with the normal conduction system serves as the retrograde limb. The resulting tachycardia shows a wide QRS complex.
D. When atrial fibrillation (AF) occurs in a patient with a manifest accessory pathway, antegrade conduction to the ventricle may occur through either the AV node or the AP. The QRS morphology may be narrow when conduction is primarily via the AV node, or wide and preexcited when conduction occurs through the AP. The QRS morphology may vary from beat to beat during AF.
@TrackYourHeart
Source: Morton’s Cardiac Catheterization Handbook( pge 314
Mau share kasus bagus yg ku bawa ke sympo!!!
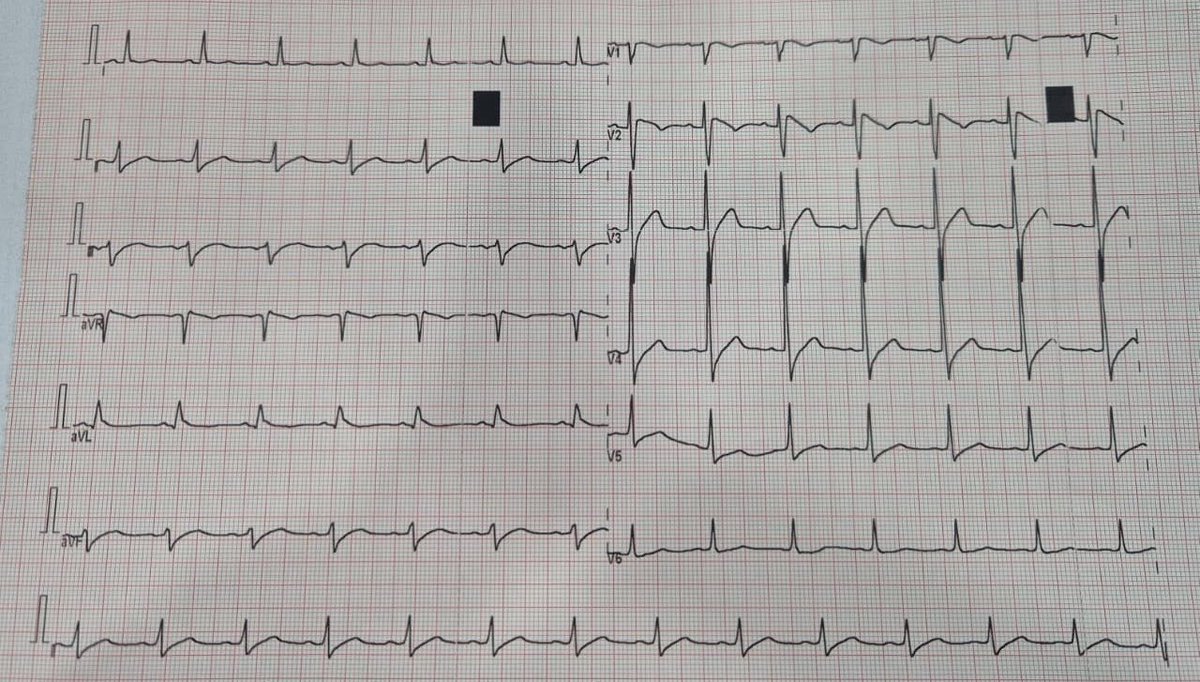
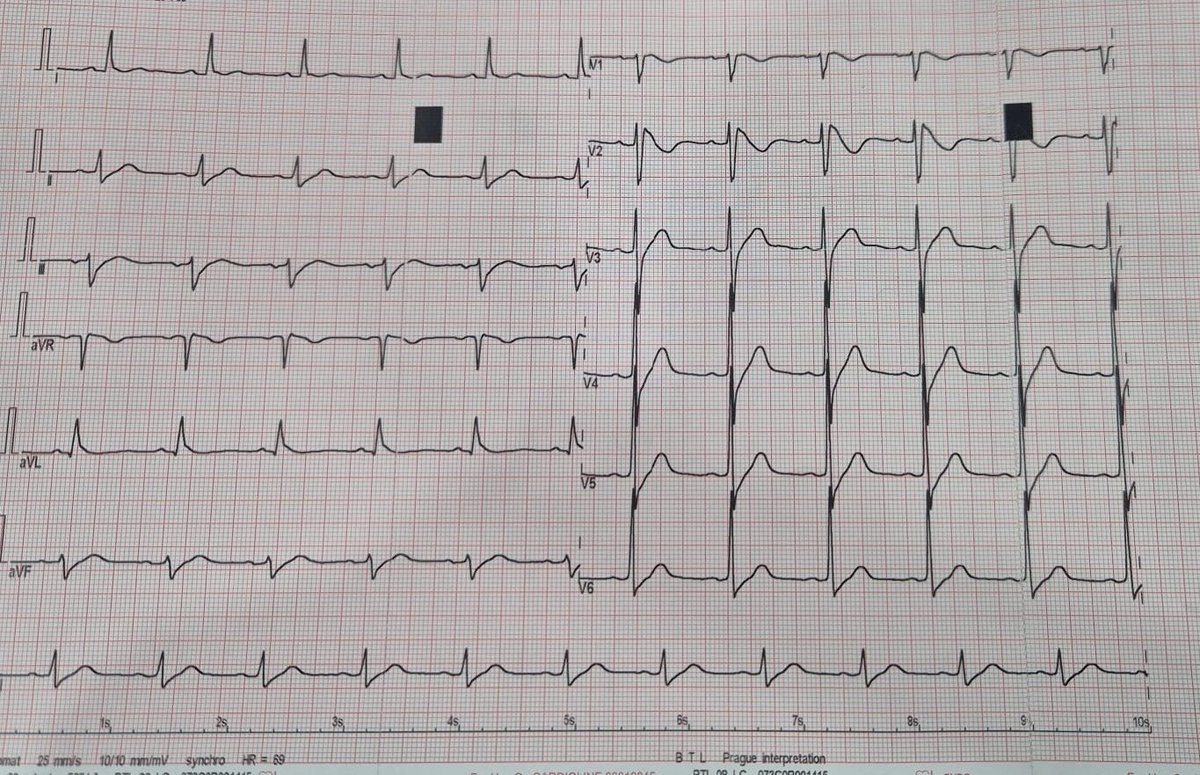
Pertama kali dateng dengan syncope dirumah, ga ada nyeri dada. Sakit jantung ga ada, tiba tiba 30 menit sadar dia bilang keluhan mual aja, ekgnya begini😔😔😔, ada yg tau ??? Khas bngt loh
In this State-of-the-Art review, Craig et al. examine one of the most debated questions in valvular heart disease: when to intervene in aortic stenosis?
From watchful waiting to early TAVI, the review analyses recent randomised trials including EARLY TAVR and EVOLVED, highlighting the balance between preventing heart failure hospitalisations and procedural/lifetime risks.
🔗https://t.co/5sdBaKSF2z
#TAVI #AorticStenosis #CardioTwitter #ValvularHeartDisease #EuroPCR
@neiljcraig@bernardprender1
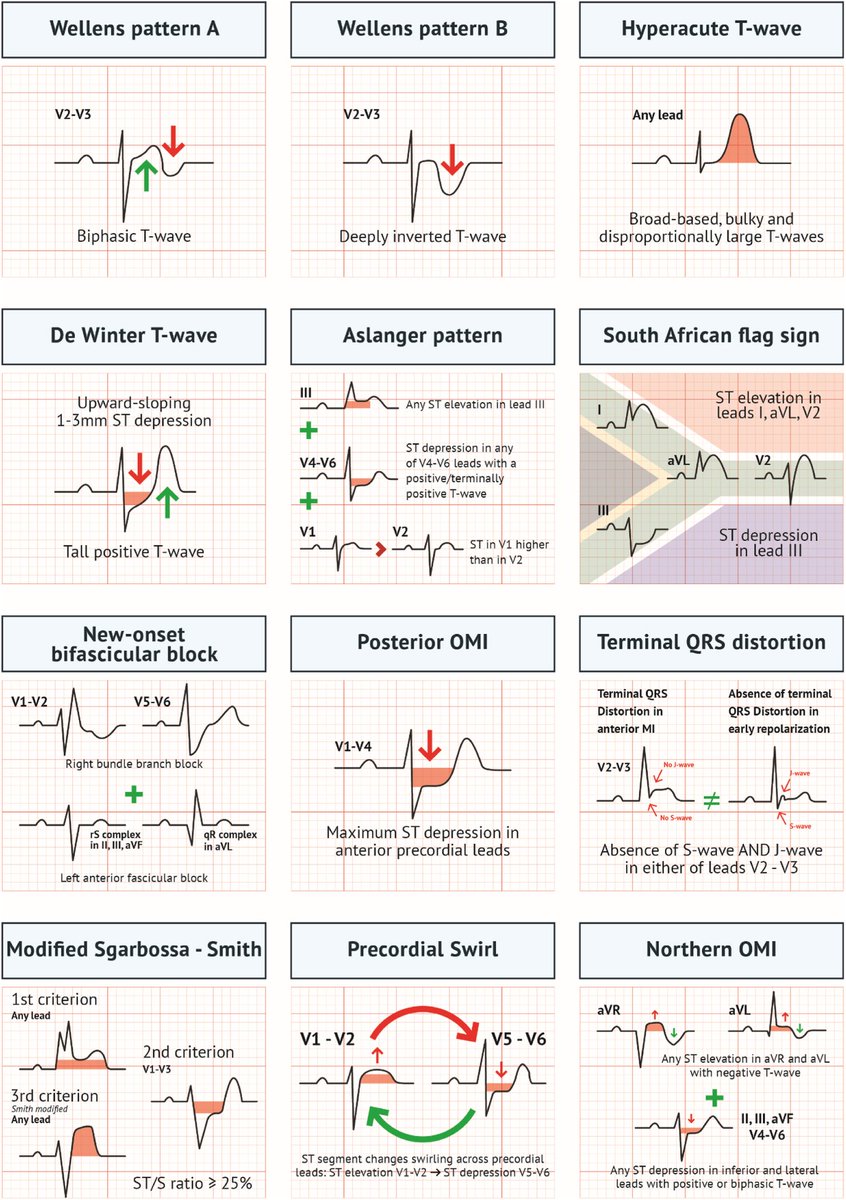
Acute MI is not always STEMI.
A major 2025 review highlights why relying only on classic STEMI criteria can miss dangerous coronary occlusions.
A thread on OMI (Occlusion Myocardial Infarction): 🧵
Understanding ECG Lead Placement ➡️A Visual Guide
This image beautifully explains how different ECG leads are recorded. Let’s break it down:
Standard Limb Leads
Lead I: RA (-) to LA (+) ➡️measures electrical activity across the chest.
Lead II: RA (-) to LF (+) ➡️ follows the heart’s natural conduction path; often best for rhythm.
Lead III: LA (-) to LF (+) ➡️ captures inferior wall activity.
These leads form the basis of the Einthoven triangle.
Augmented Limb Leads (not shown individually here but derived from same electrodes):
aVR: Views the heart from the right shoulder.
aVL: Views from the left shoulder.
aVF: Views from the foot (inferior aspect).
Precordial (Chest) Leads
- V1: 4th ICS, R sternal border
- V2: 4th ICS, L sternal border
- V3: Between V2 & V4
- V4: 5th ICS, midclavicular line
- V5: Anterior axillary line, same level as V4
- V6: Midaxillary line, same level as V4
These leads provide horizontal plane views of the heart.
Wilson Central Terminal (WCT)
- Formed by connecting RA, LA, and LF electrodes through 5kΩ resistors.
- Acts as a common negative reference for all chest (V) leads.
Accurate placement is crucial for proper diagnosis.
Ref: brauwald's heart disease 12th Edition
🫀⚠️ We’ve been selecting patients for revascularization… wrong.
👉 ischemia = treat... not really?
For years the rule was simple:
👉 find ischaemia
👉 fix the artery
But what if ischaemia is NOT the key?
This editorial on CTO-PCI says something uncomfortable:
👉 Ischaemia does NOT predict outcomes.
Even when:
👉 ≥10% ischaemic burden
👉 PET or SPECT proven
There was:
❌ no reduction in death
❌ no reduction in hard events
So what actually improves?
👉 Symptoms.
👉 Quality of life.
That’s it.
Let that sink in.
We are:
👉 opening complex CTOs
👉 taking procedural risks
👉 chasing ischaemia
But:
⚠️ Ischaemia is NOT driving prognosis.
The real paradigm shift
From: ❌ Ischaemia-driven cardiology
To: 👉 Patient-driven cardiology
The new selection logic:
👉 refractory angina
👉 functional limitation
👉 patient suffering
FIRST.
Imaging?
Still crucial��but:
👉 as a SUPPORT tool, not the decision-maker
Even the paper states it clearly:
👉 Ischaemia alone is an insufficient arbiter for revascularization
And there’s a deeper problem
We love measurable things:
👉 % ischaemia
👉 flow reserve
👉 perfusion maps
But we ignore:
👉 symptoms
👉 daily function
👉 real patient experience
My take
This is the same cognitive error we see everywhere:
👉 We treat numbers
instead of
👉 treating patients
Final thought
If your indication for CTO-PCI is:
👉 “there is ischaemia”
You’re already outdated.
The future is brutally simple:
👉 No symptoms → think twice
👉 Symptoms → act
⚡ Because in modern cardiology:
The most important endpoint is not the image.
It’s the patient.
#Cardiology #CTO #PCI #Ischaemia #Imaging #PrecisionMedicine #CardiacCT #CardiacPET
I tested 3 AI tools on the same ECG case.
1. ChatGPT
2. Google Gemini
3. PMcardio
A 65-year-old man. Chest pain. Subtle but dangerous pattern.
Here’s what happened 👇
The most likely diagnosis: VT.
A wide QRS complex tachycardia (WCT) (rate >100 bpm, QRS >120 ms) should be treated as Ventricular Tachycardia (VT) until proven otherwise, as VT accounts for roughly 80% of cases and >90% in patients with structural heart disease.
Misdiagnosing VT as Supraventricular Tachycardia (SVT) can lead to inappropriate, fatal treatments; hence, immediate assessment for hemodynamic instability and potential ACLS management is crucial
Ventricular tachycardia signs😍
1. Fusion beat
2. Capture beat
3. Josephson's sign
4. Brugada sign
5. +Ve or -Ve Concordance
6. AV dissociation