☢️Neoadjuvant CRT vs. ChT for initially unresectable locally advanced "Colon" cancer
@eClinicalMed
➡️45 patients
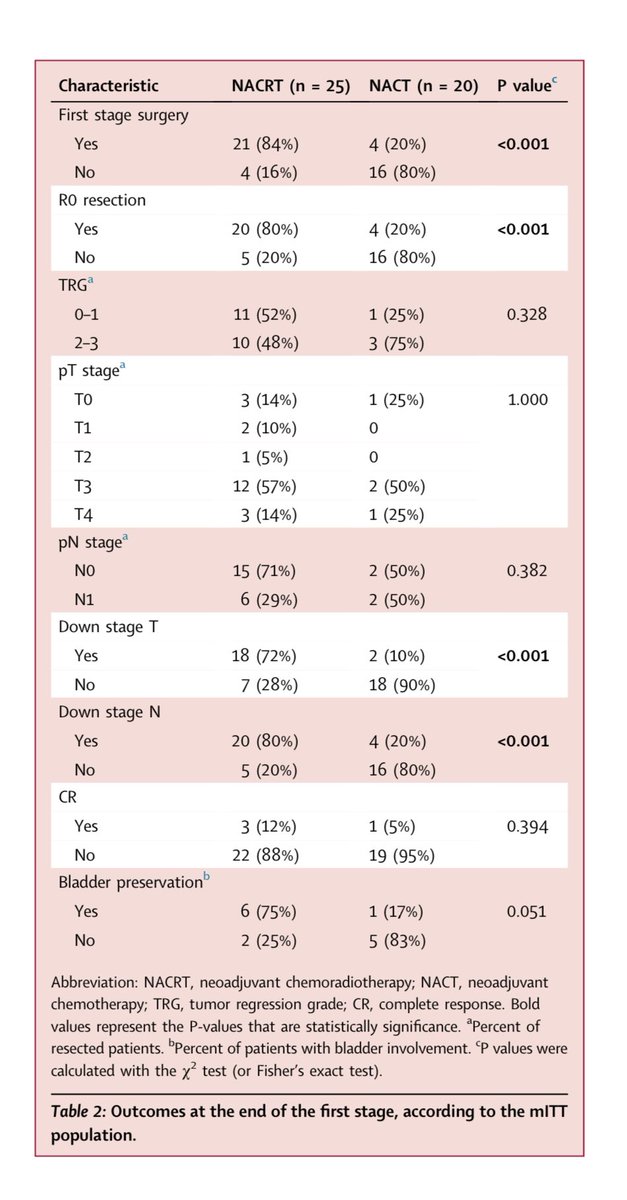
✅R0 resection: 80% vs. 20%, P < 0.001
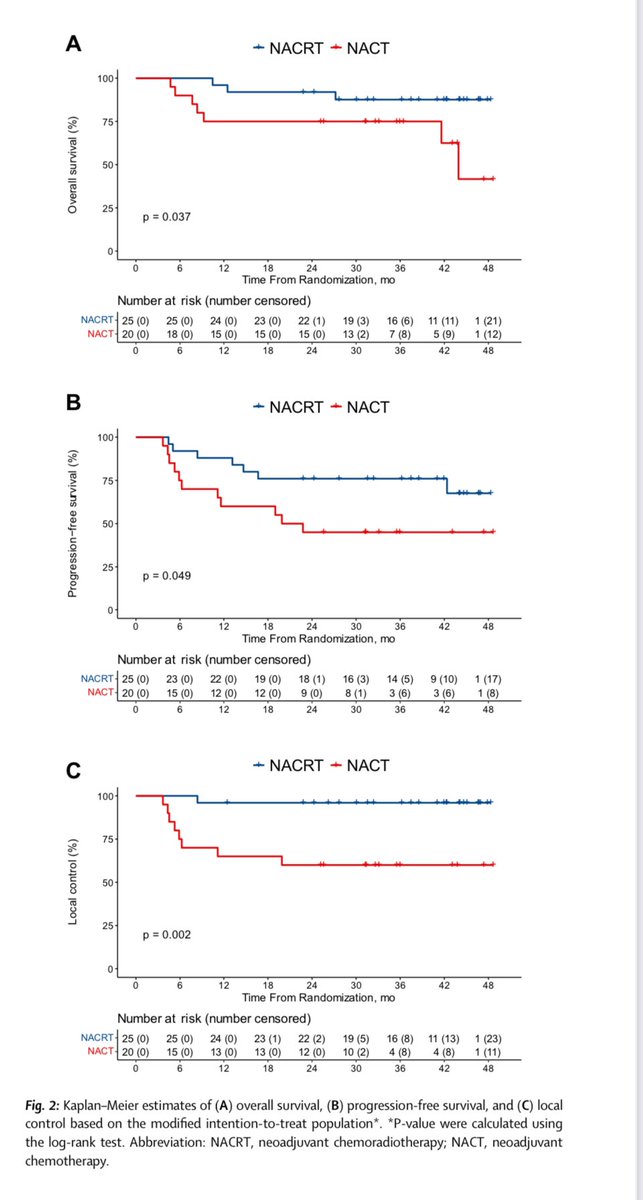
✅3-year PFS: 76% vs. 45% , P = 0.049
✅3-year OS: 87.6% vs. 75% , P = 0.037
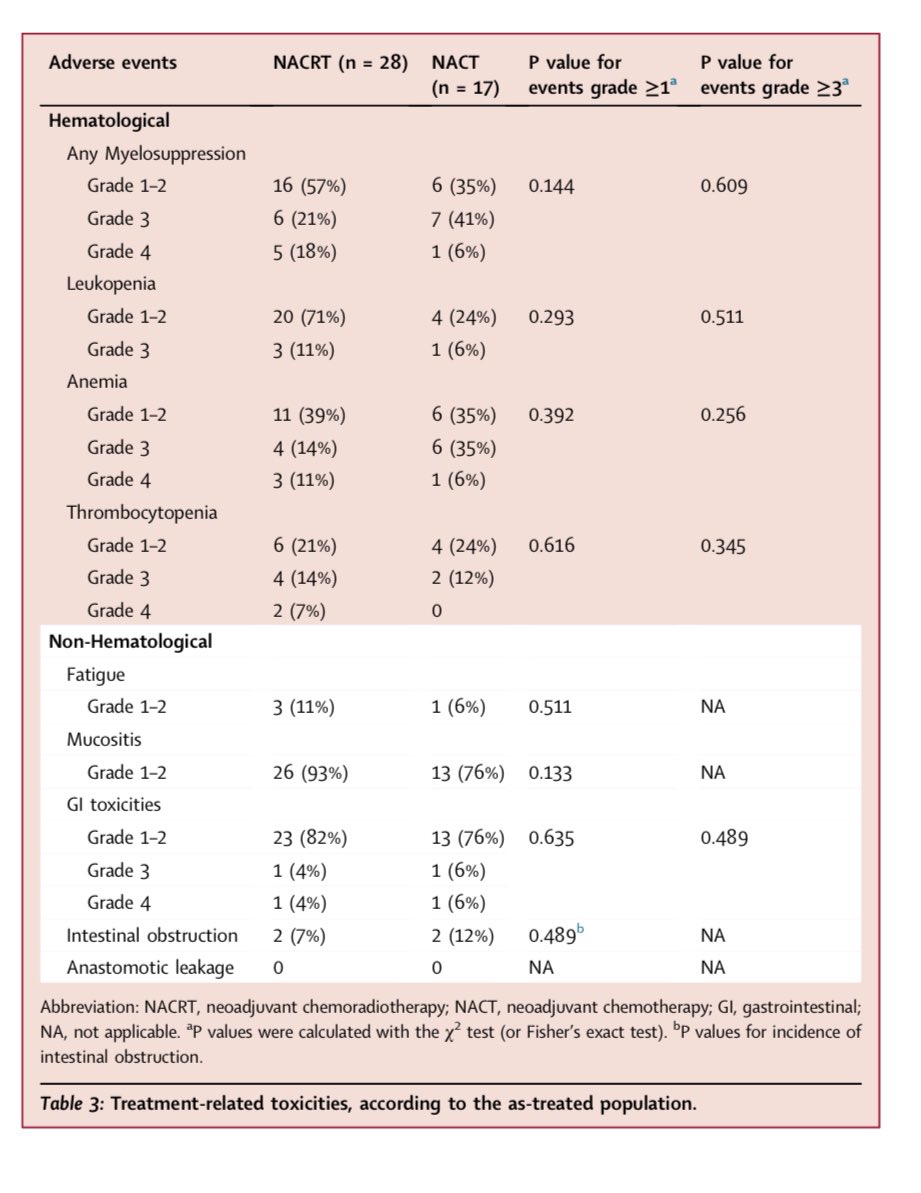
✅No differences in severe AEs
❗️Study was terminated prematurely because of R0 resection benefit of CRT
👉https://t.co/WqFpJLSwaN
@TheLancetOncol@TheLancet@LancetGastroHep@myESMO@OncoAlert #cancer #oncology #MedX
🎙️ PBT hás similar OS, but ⬆️ PFS and LC compared to TACE for #HCC❗️❗️ 🚨@OncoAlert
📌Ph3 RCT: TACE vs PBT for #HCC
-PBT:70.2Gy/15fx, TACE until max response
🥇🎯:OS
📊RESULTs
👉2-y OS :68% PBT vs 65% TACE
👉PBT ⬆️ PFS & LC than TACE
👉Post-treatment hospitalization significantly ⬇️PBT (24 days) ✖️ to TACE (166 days)
👉Mean 💰 analysis PBT⬇️ 28% of total costs, being a⬆️⬆️ efficient treatment option
#HCC #radonc #proton https://t.co/OXMQ4TGGUo
TACE vs. SBRT for HCC: randomized phase II TRENDY trial
- stoped early due to poor a accrual
- all endpoints significantly or numerically better after SBRT
👉 time to progression 19 vs 12 mo
👉 median OS 44 vs 37 mo
👉2a local control 100% vs 44%
CONGRATS
https://t.co/XQt9uNqiIs
Sharing our recent work on brain metastases from biliary tract cancers, led by outstanding Baylor medical student Grace Dodoo and senior authors @eugenekoay and @ebludmir
Pleased to share our latest work in @IJROBP examining costs of radiotherapy under the Oncology Care Model. This was a fantastic collaboration with @NGThaker_XRT and the team at @AZOncology. https://t.co/vO9AivplAX
Very interesting work by Linda Cao (R5 @JohnsHopkins) at #astro22 using @Elekta CORE OMD multicentre database:
✅ LC predictive of progression and OS
✅ GTV/ITV Dmin a/b 60 most predictive of LC
✅dose thresholds for 95% LC in radioresistant histologies
#radonc
Excited to share the first prospective study of MR guided RT in #PancreaticCancer@IJROBP. Ablative RT with concurrent full dose chemo. All tumors abutted at least 1 OAR. 2-yr LC 85%. Median OS for ECOG 0 and CA 19-9<90 pts were 34 and 43 mos.
https://t.co/AwJp296FMP
@gar02118@Aiims1742@ChaurasiaMD@Vince_BernPag@TaniguchiMD@rweichselbaum One potential solution is for each program to contract 1 position every other year, an average of 45 fewer residents per year. Every program would be impacted and it would decrease residents by 20-25%. Contraction requires a collective effort.
@AshwinShindeMD@adapthyun Figure 1 from our paper. A total of 87 pts treated with SC-RT+chemo. 73 had endoscopic evaluation, of which 33/73 (45.2%) had CR while 40/73 had non-CR. Seems like CR rate was 50% in WashU study and ~75% in OPRA (included CR and near CR).
Excited to share the Johns Hopkins experience on NOM in rectal cancer treated with SC-RT and consolidation chemo. ☢️
-25Gy/5fx -> chemotherapy
-26 achieved complete response (CR) and managed with NOM
-LARS and EORTC surveys to assess anorectal function
https://t.co/nwr1cogouT
Conclusions: NOM is safe and feasible in pts who achieve CR to SC-RT and consolidation chemotherapy. Our findings support initial experience/data from WashU on SC-RT. @adapthyun@ReIChinMD@DrEmmaHolliday
Here's our series of children treated with craniospinal RT using ELECTRONS ⚛️for spinal fields since 1983.
https://t.co/TaltFvGBlX
-84 pts, 48 followed for ≥ 5 yrs
-MC histology: Medulloblastoma/PNET (59%)
-Median age at RT 5 yrs
-Median follow up 19 yrs
All of this commentary about the omission of RT being valid with only 5 years of follow-up LUMINA when even EBCTCG data says the maximum benefit of AI in years 1-4 is highly problematic.
Modern RT is nontoxic and can be delivered in 5 days for most omission candidates. #bcsm