Canlı yayını 27 Ekim 2025 Pazartesi günü saat 20.00 da https://t.co/PCSoCpGJrf adresinden izleyebilir; sorularınızı, yorumlarınızı yazarak toplantıya katılabilirsiniz. Bekliyoruz…
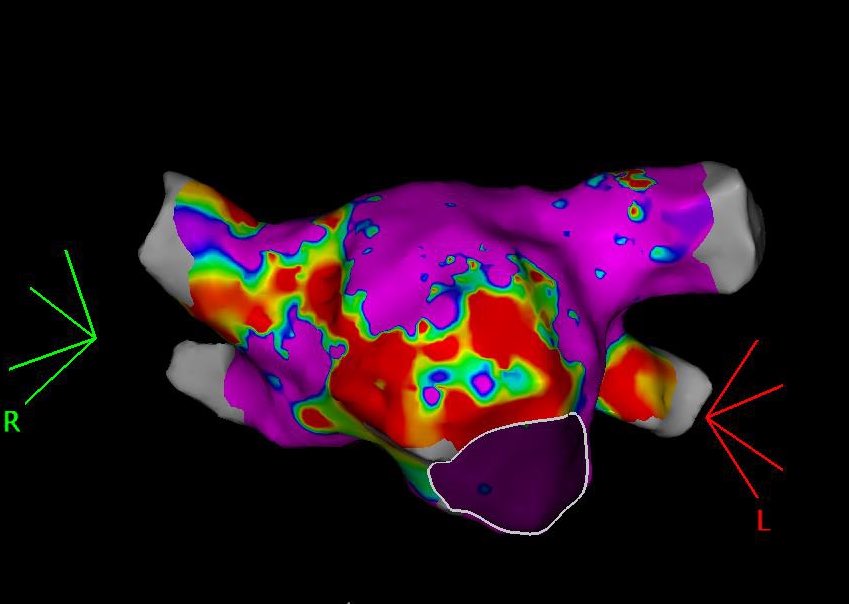
A biatrial flutter in a pt w septal scar w/o hx of abl! Easy to mistake for a cti flutter if only RA is mapped since only tiny portion of the cycle is missing. @akyurek_omer@timucin_alt#Epeeps
#Epeeps
Epi only mapping & #Rf in apical aneurism w endocardial thrombus precluding endo approach. #VT terminates shortly after Rf on mid isthmus. @timucin_alt@akyurek_omer
@syamkumarmd@pjsm83@akyurek_omer@timucin_alt@ozkanatfirat@seeenaaay@elifoykucelik @MiguelVldrbno No, tbh i try to avoid wire mapping when possible (poor signal qual, can’t determine max dv/dt etc). Etoh was infused anatomically between 1-2 and 3-4 MapIt pairs. I do not remove the wire as it would be hard to repositionthe monorail balloon.
#EPeeps LV summit VT(+ICDshock) in a pt w bioprosthetic AVR&MVR. Endo breakthrough@QRS onset. Only precocity @ annularV (30ms). Extensive anatomical abl (endo+PA) fails, while ETOH inf. makes VT non-inducible. @akyurek_omer@timucin_alt@ozkanatfirat@seeenaaay@elifoykucelik
@TimothyMaherMD1@BIDMC_VT@sarah_chomos Great maps. What was the final lesion set (aka was there any other VT with a different isthmus, not predicted by endocardial ILAM)?
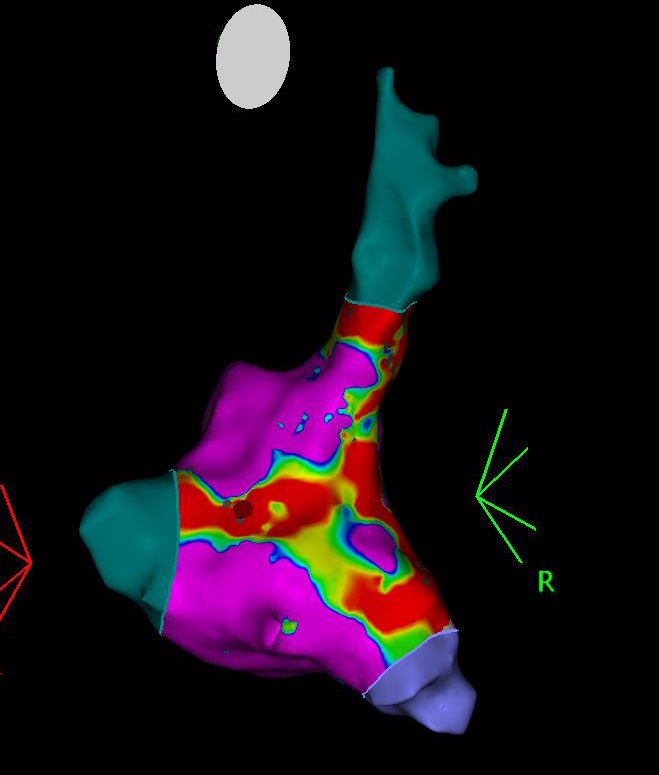
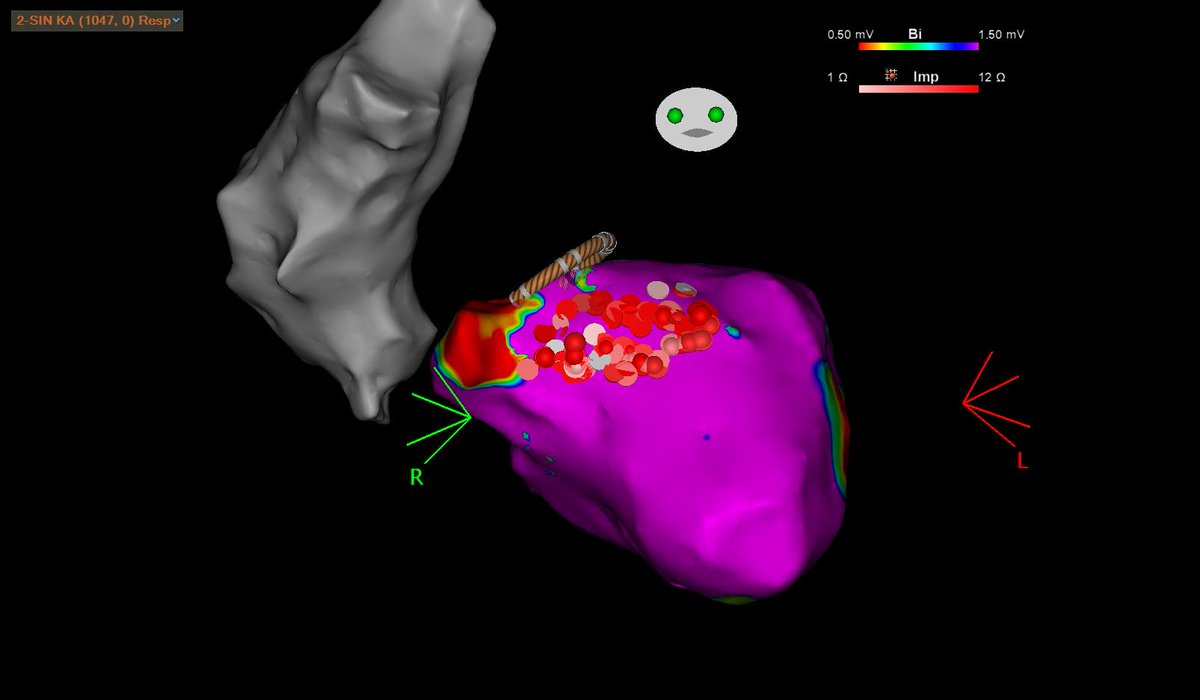
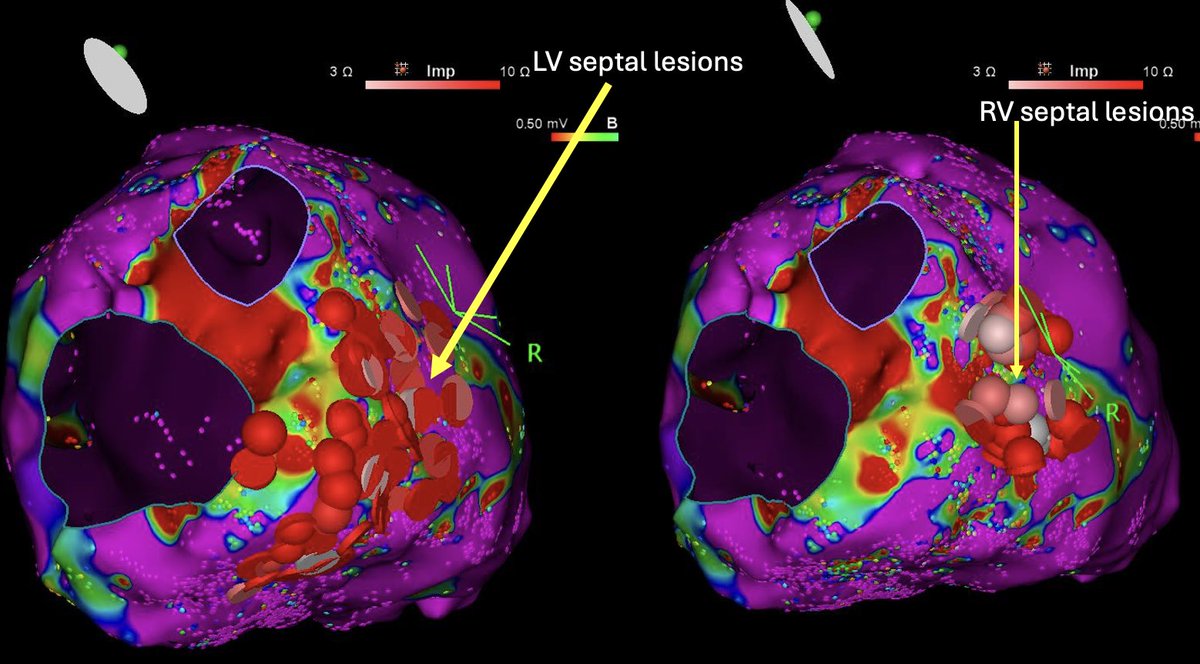
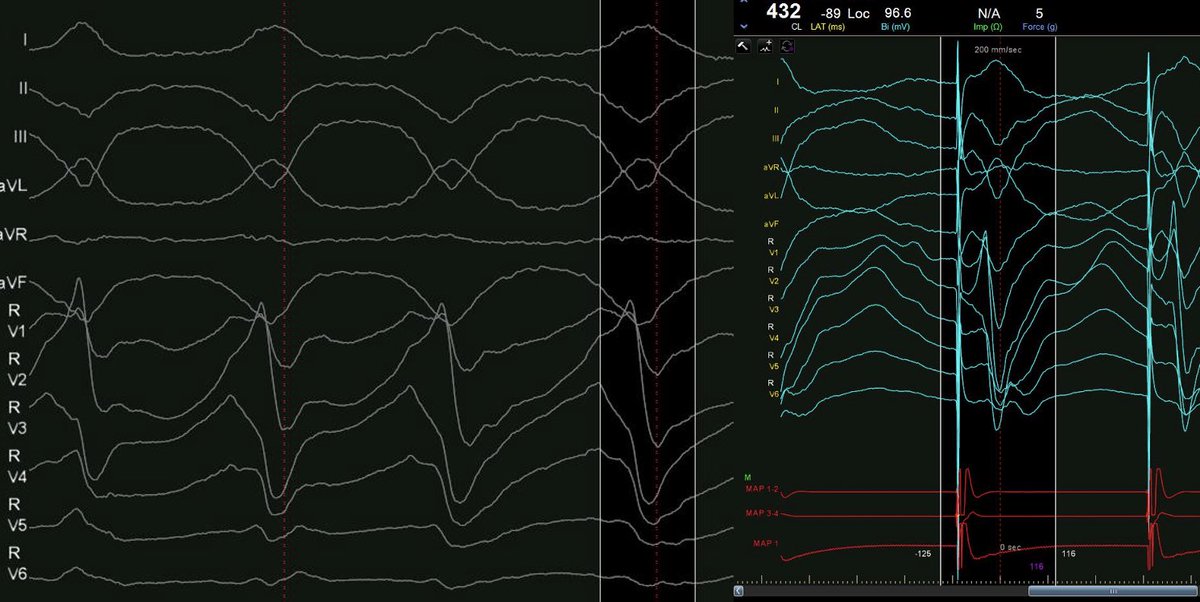
#Epeeps Classical presentation of midmyocardial septal scar and VT. Patchy biV LVA, low uniV and an unstable VT that has 94% pacematch at the RV septum. Sequential burn renders VT non-inducible. @timucin_alt@akyurek_omer
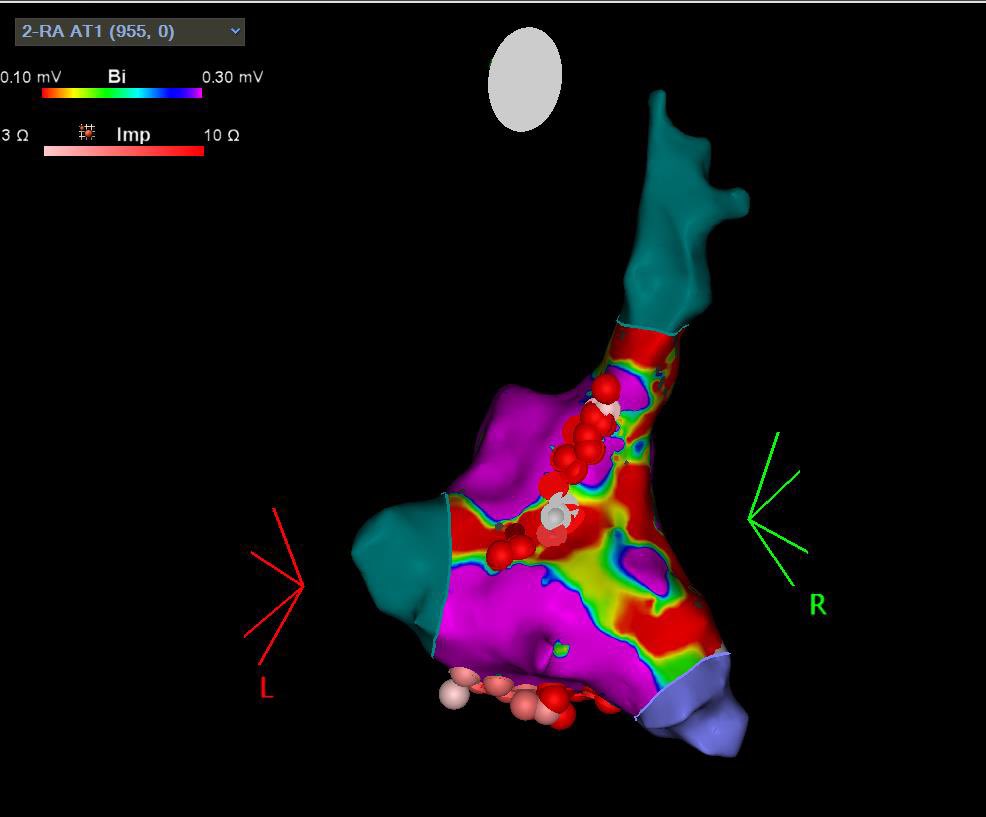
@finnakerstrom@akyurek_omer@timucin_alt PPI- TCL was 0 from both CSp and CSd with no act change compared to the AT. At CTI ppi-tcl was 10msec. Rf at endocardial RA breakthrough terminated the AT but i would imagine that CTI would have also terminated it.