🚨 Out today in Cell! @CellCellPress
Path2Space: #AI that predicts spatial transcriptomics (ST) from H&E pathology, enabling spatial biomarker discovery in #BreastCancer at scale.
📄 https://t.co/GtrmH9zIDs
🧵1/8
Grateful for our team effort featured by Mayo Clinic News Network—developing a blood test to detect germ cell tumors missed by standard markers.
https://t.co/HR7nFfaJJa
Our paper in @Nature today 🥳 We tracked 6,438 mice from puberty to death and mapped the genetics of *when* you die, not just whether a gene associates with lifespan.
https://t.co/EoeexqJoHk
59 loci. Two decades of data. Thread 👇
#Longevity#Aging#Genetics#Healthspan
Why do only some cancer patients develop #paraneoplastic neurological syndromes (PNS)? 🧠
This review explores the immune mechanisms behind PNS and how tumor genetics & immune tolerance shape risk. Kudos to @AKunchok. Open access link: https://t.co/glF1CAIhn5
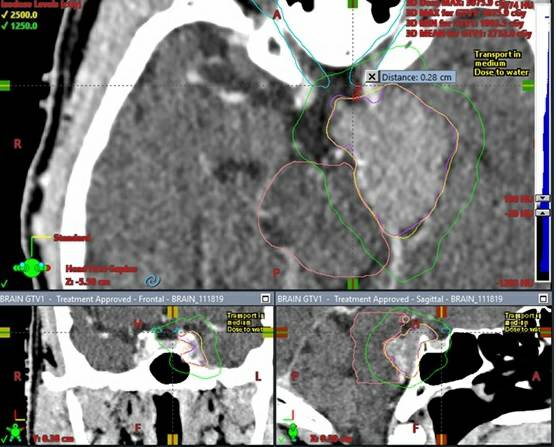
Should we treat higher SRS doses for brainstem mets (than the typical lower doses used)?
Tumor control probability MODELING:
1 Yr 90%LC 18.9 Gy/1, 25.7/3, 28.6/5
2 Yr 90%LC 20.5 Gy/1, 28.2/3, 31.5/5
https://t.co/mipCmC609f
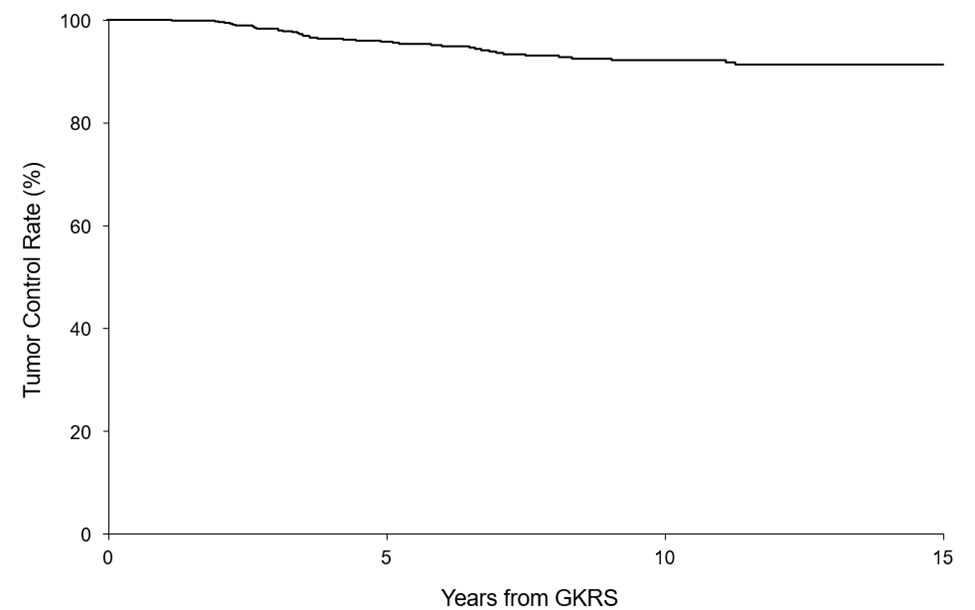
What is the long term control Sporadic Vestibular Schwannoma after radiosurgery?
LC 5, 10, & 15 years 96%, 92%, & 91%
13% pseudoprogression median time 0.5 yrs (only 4% >5yr after SRS) https://t.co/x4MHXTUNC9
Gonzalez-Aponte et al. reported circadian rhythms in MGMT promoter methylation and protein levels in GBM, with peaks at midday and CT4, respectively, predicting time-of-day differences in temozolomide efficacy. #JNO
Read more:https://t.co/2eDZ6vL8fo
Cognitive recovery after radiation brain mets meta-analysis
· 1/3 cognitive recovery @6mo after initial decline
· Recovery more likely if SRS or HA-WBRT compared to WBRT
https://t.co/S7aeKaiHAA
A decade after our world-first BBB opening for #GBM, our newest trial shows FUS is safe, well-tolerated, with signals of benefit.
A major milestone for a devastating illness.
Grateful to @INSIGHTEC, @FUSFoundation, our donors, and brave patients.
https://t.co/eoBYfieJQR
This is a great description of what is was like for @BobbyMukkamala, incoming AMA President and ENT surgeon, to have an awake craniotomy. @MayoClinicNeuro @MayoClinic https://t.co/907ljr5qGJ
When I have a new fellow or resident in our peripheral nerve clinic, I always teach them the importance of defining the neuropathy clinical syndrome. NCS/EMG are valuable, but the neurological exam is the most important (as it should be in neurology but many have forgotten).
This is the neuropathy clinical phenotype classification I find the most helpful:
- Isolated small fiber neuropathy
- Length-dependent peripheral neuropathy (or distal symmetric polyneuropathy)
- Multiple mononeuropathies
- Mononeuropathy
- Asymmetric neuropathy
- Polyradiculoneuropathy
- Plexopathy (brachial or lumbosacral, many times a radiculoplexus neuropathy)
- Sensory neuronopathy
- Motor neuronopathy
I always tell my trainees they don’t have to memorize the causes of each phenotype. If you define the syndrome correctly, you can ask Google or ChatGtp what are the most likely causes. 😊
Definitions 👇👇👇
#NeuropathyBites
1/x
Our new CASPR2 paper is out @ANA_journals 🤩
Headlines: Patients have neuropathic pain & fatigue as their main long term complaints which determine QoL. 😰
These are NOT immunotherapy responsive. 👩🏾⚕️💊
We also report other nuggets in this thread 🧵 ⬇️
https://t.co/rngFbpplVF
In celebration of the legendary career of Professor Peter J. Dyck, who officially retired last month, I kick off today this series with a hidden gem: The 10 P's in the characterization and differential diagnosis of peripheral neuropathy.
#NeuropathyClassics#DyckPapers
1/
Instead of listing my publications, as the year draws to an end, I want to put pressure on the commonplace assumption that productivity must always increase. Good research is disruptive and thinking time is central to high quality scholarship and necessary for disruptive research