Cardioembolic stroke is a SOURCE-CONTROL diagnosis.
The approach is simple:
PATTERN → SOURCE → PREVENTION → TIMING
PATTERN
Suspect embolism when you see:
• sudden maximal deficit
• cortical signs
• LVO
• abrupt vessel cut-off
• multiple vascular territories
• bilateral infarcts
• anterior + posterior circulation lesions
• hemorrhagic transformation
• recurrent events despite antiplatelet therapy
But remember:
An embolic MRI pattern is a clue.
Not a prescription.
SOURCE
Now interrogate the heart.
Common suspects:
• AF / atrial flutter
• left atrial appendage thrombus
• LV thrombus after MI
• mechanical valve
• rheumatic mitral stenosis
• infective endocarditis
• NBTE / cancer / APS
• PFO with paradoxical embolism
• aortic arch plaque
Each source changes treatment.
TESTS
Minimum source hunt:
• ECG
• telemetry
• CTA/MRA head-neck
• TTE ± contrast
• TEE when LAA, valve, PFO, vegetation, or aortic arch source is suspected
• prolonged rhythm monitoring if no cause is found
• blood cultures if fever, murmur, prosthetic valve, or sepsis clue
• DVT/PFO workup in selected young strokes
A normal ECG does not clear the heart.
PREVENTION
Source selects treatment.
AF → DOAC usually
Mechanical valve → warfarin
Rheumatic MS + AF → warfarin
LV thrombus → anticoagulate + repeat imaging
IE → antibiotics/source control
NBTE/cancer → anticoagulation + treat driver
Selected PFO → closure discussion
ESUS → no empirical DOAC
This is the biggest trap:
ESUS is not hidden AF until proven otherwise.
Atrial cardiopathy is not AF.
PFO is not always causal.
AF does not mean stop looking.
TIMING
Do not anticoagulate the anxiety.
Use the brain scan.
TIA → day 0–1
Small infarct → day 1–3
Moderate infarct → day 3–6
Large infarct / hemorrhagic transformation → day 6–14+ and reimage
Modern trials support earlier DOACs in selected AF-related strokes.
But routine early anticoagulation for every AIS is still not the rule.
Final rule:
Pattern suggests embolus.
Proof names the source.
Source selects prevention.
Infarct size sets the clock.
Anticoagulate the source, not the vibe.
#Neurotwitter #MedX #Stroke #Cardioembolic
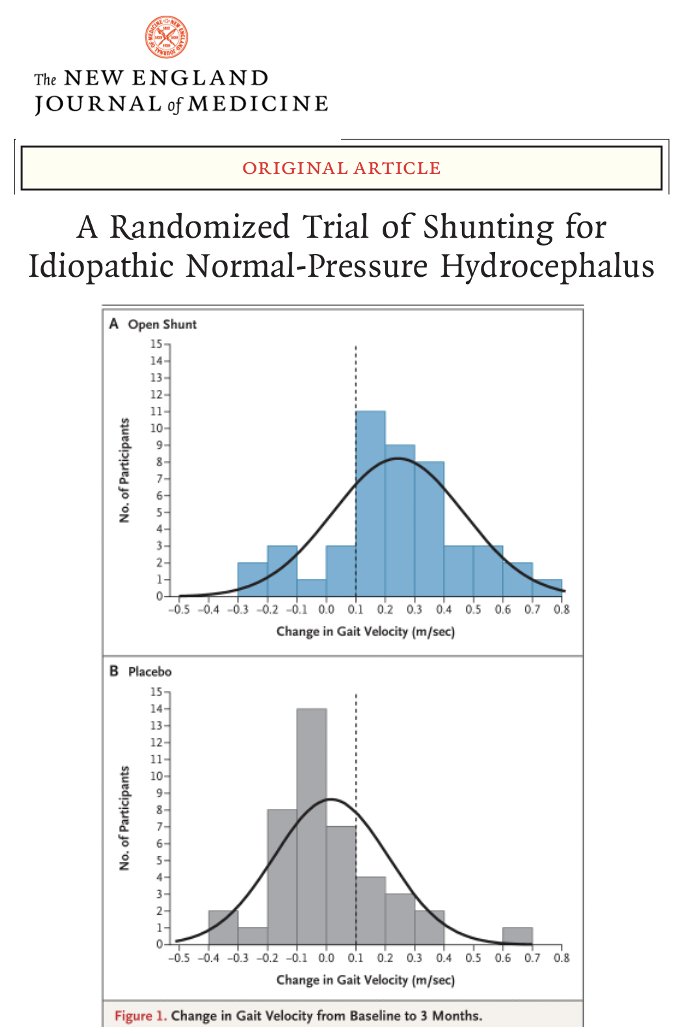
To shunt or not to shunt, that is the (NPH) question? The first large randomized trial of shunting for normal pressure hydrocephalus (NPH) just dropped in NEJM, and there was clear benefit for walking, and it favored the group receiving shunts. Spoiler alert: Walking improved, however thinking (cognition) and bladder function did not.
Key Points:
- NPH is a condition usually presenting in older adults where fluid builds up in the brain and it associated w/ trouble walking, memory and thinking challenges as well as bladder incontinence.
- Shunting significantly improved walking speed and balance compared w/ placebo.
- No meaningful change in cognition or bladder control observed at 3 months.
- Risks included subdural bleeding and headaches, underscoring the need for careful follow up.
My take: NPH has always been a tricky area for clinicians when trying to decidr 'to shunt or not to shunt.' Here are 5 points that resonated w/ me: 1- Shunting in well selected persons can restore some walking ability in NPH. 2- Thinking did not improve at 3 months. 3- Incontinence showed no clear benefit. 4- Risks to always discuss w/ people considering shunts should include bleeding and headaches (as not uncommon). 5- Walking gains may possibly reduce falls and boost independence, however we must be careful as sometimes improved walking w/o improved balance, can actually trigger falls.
https://t.co/yCnSCpclPL @FixelInstitute@ParkinsonDotOrg@alzassociation@SfNtweets@SfNtweets@NEJM
#MondayTip
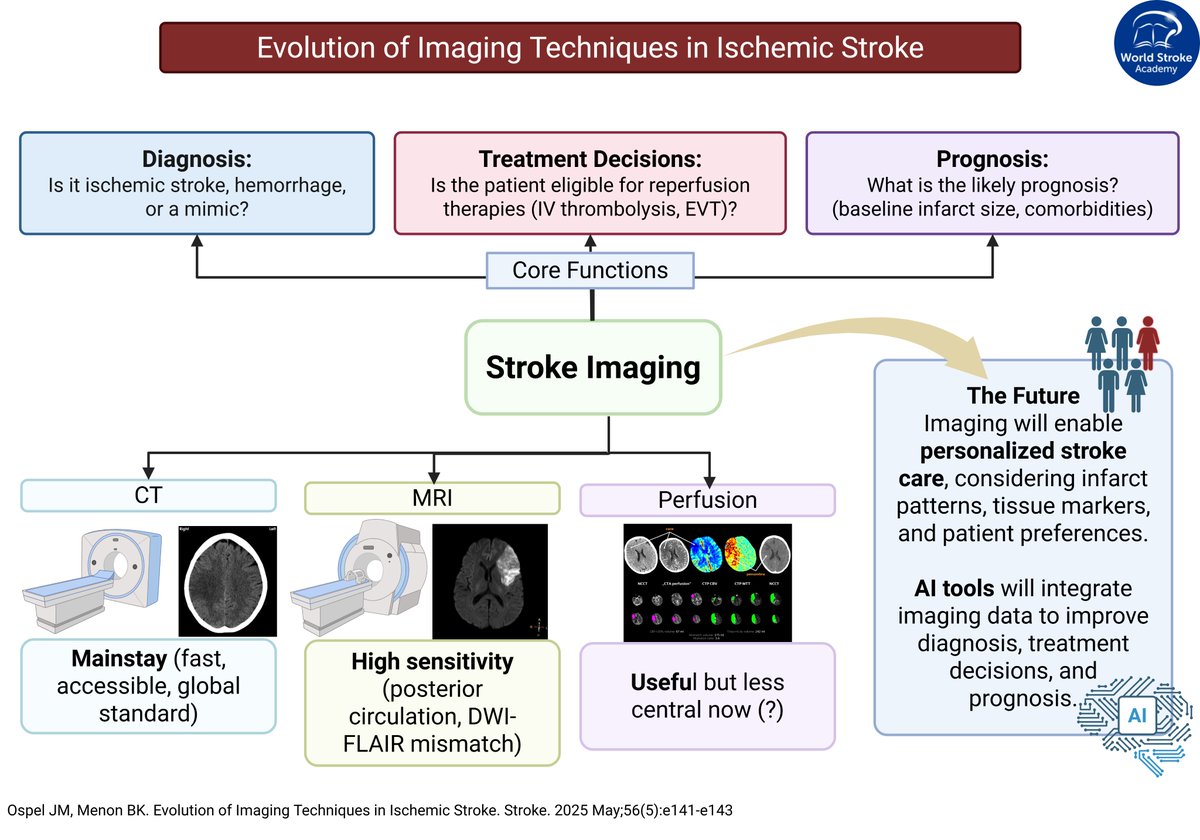
Imaging Techniques in AIS
📸Essential for diagnosis, guiding treatment & prognosis
⏱️Excessive imaging can delay treatment👉time is brain
🎯Targeted imaging is often sufficient for safe, effective decisions
From @bijoymenon@johanna_ospel https://t.co/Q9YO4I9eTb
Key Point 2 from the article Multiple System Atrophy Dr. Tao Xie from the August #MovementDisorders issue, which is available to subscribers at https://t.co/uMxlrXNllP.
#Neurology#NeuroTwitter#MedEd
Diagnostic accuracy of the STANDING algorithm in patients with isolated vertigo: a multicentre prospective study (STANDING-M) | Emergency Medicine Journal https://t.co/TyR3pUDgHx
¿Cuando Iniciar DOAC en ACVi?
🎯 Objetivo principal:
Estimar los efectos de iniciarDOAC en ≤4 días VS ≥5 días después de un ACVi en personas con FA
💊 Inicio temprano de DOAC📉 riesgo de ACVi recurrente, HIC sintomática o ACV no clasificado a los 30 días (OR 0.70, IC 95% 0.50-0.98, p=0.039).
🧠🩸No hubo evidencia de un 📈 en HIC Sintomática con inicio temprano de DOAC (10 [0.4%] de 2683 versus 10 [0.4%] de 2746; OR 1.02, IC 95% 0.43-2.46, p=0.96).
🚨#EducaciónContinua Invitamos al Curso Virtual "NeuroECHO Vascular, Actualidades en Infarto y Hemorragia Cerebral".🧠
👩💻👨💻 5 Sesiones en linea del 17 de julio al 14 de agosto
🔍🖊Consulta el programa y regístrate escaneando el código QR.
✅Actividad de carácter gratuita.🥼






















![CAlejandroneuro's tweet photo. ¿Cuando Iniciar DOAC en ACVi?
🎯 Objetivo principal:
Estimar los efectos de iniciarDOAC en ≤4 días VS ≥5 días después de un ACVi en personas con FA
💊 Inicio temprano de DOAC📉 riesgo de ACVi recurrente, HIC sintomática o ACV no clasificado a los 30 días (OR 0.70, IC 95% 0.50-0.98, p=0.039).
🧠🩸No hubo evidencia de un 📈 en HIC Sintomática con inicio temprano de DOAC (10 [0.4%] de 2683 versus 10 [0.4%] de 2746; OR 1.02, IC 95% 0.43-2.46, p=0.96).](https://pbs.twimg.com/media/GvizQauXEAAardZ.jpg)































