https://t.co/2I5jeiBtaA
Physician intimidation comes in many ways... I have had colleagues warn me many times "Paul watch your back, powerful people are unhappy with your advocacy"...
1/5
March 3rd: This old guy came out of retirement two years ago to help because we are short ER doctors. I just worked three very long shifts in a small town near #yeg.
Despite our small ER being half blocked by ALC patients, we receive ambulances diverted from blocks away from the Misericordia Hospital in West Edmonton, including critically ill EMS transfers.
When ambulances are diverted 30 km out of the capital city to a small-town ER, you know the system in Edmonton remains in CRISIS, as "the flu" is fading.
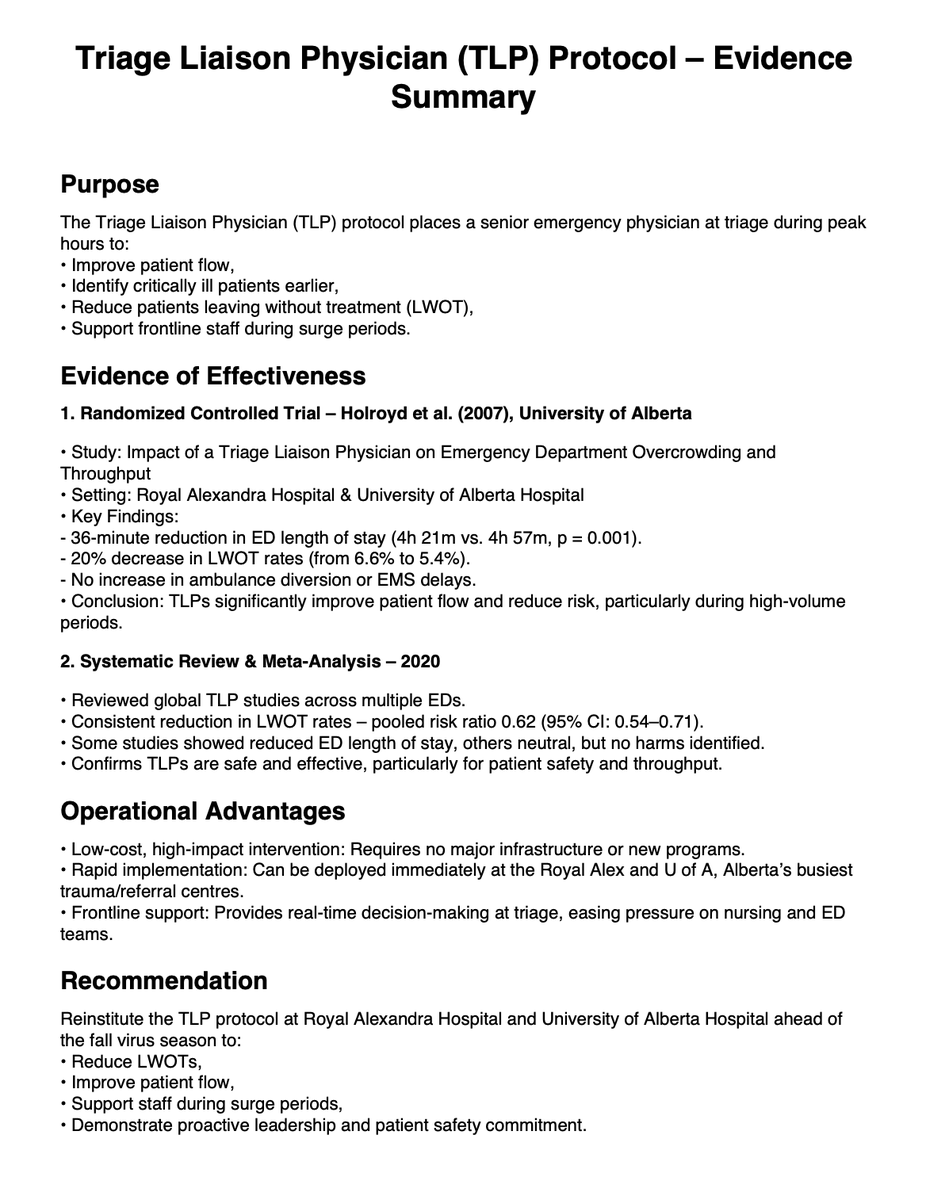
More on Triage Liaison Physicians and the ER crisis:
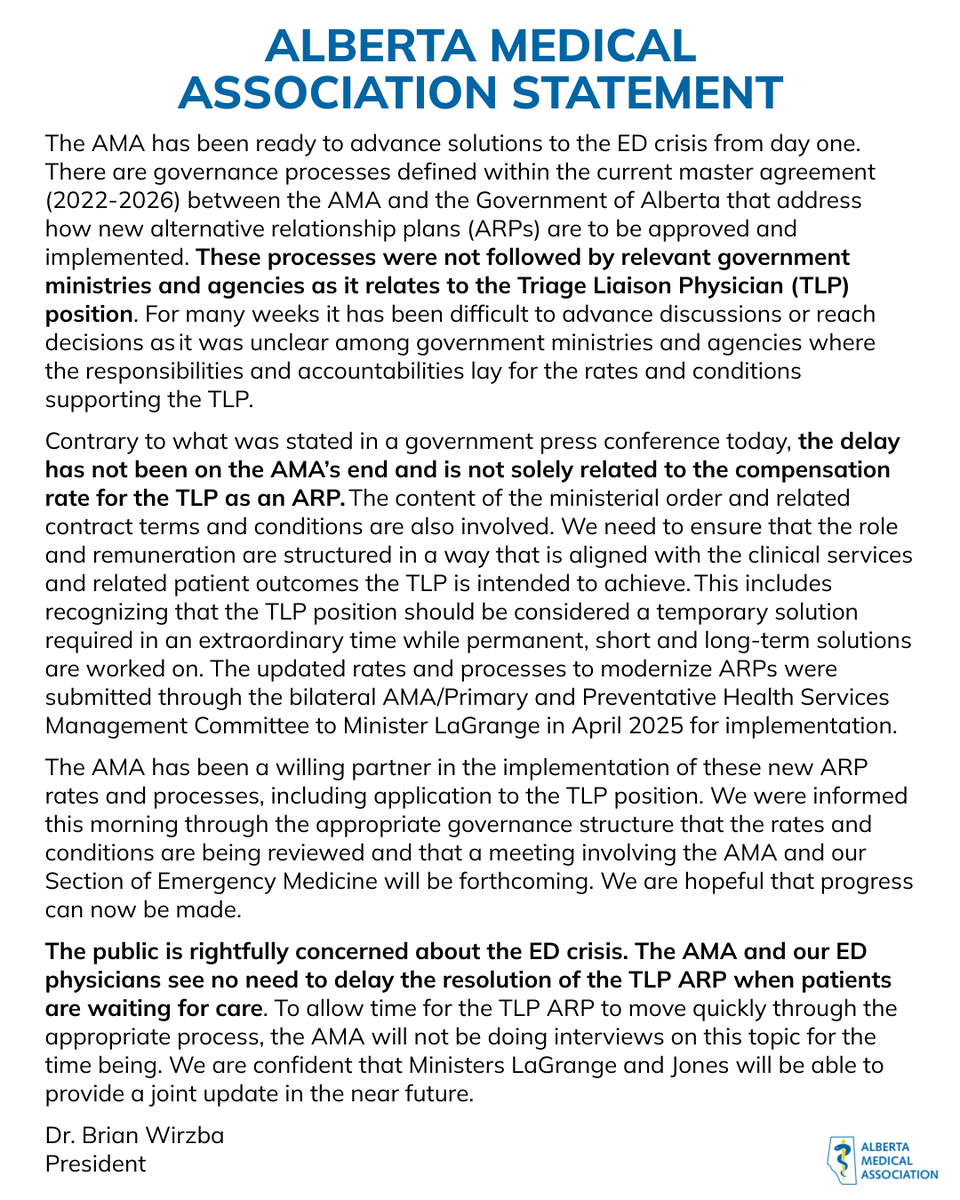
1. @Albertadoctors state clearly: “The delay in implementing Triage Liaison Physicians has not been on the AMA’s end.” (see letter below)
2. Premier @ABDanielleSmith says “it takes two parties to negotiate.” (see video in other tweet)
3. I say: Time to stop the NONSENSE and implement TLP ASAP while @JasonNixonAB clears ALC beds so flow can happen again.
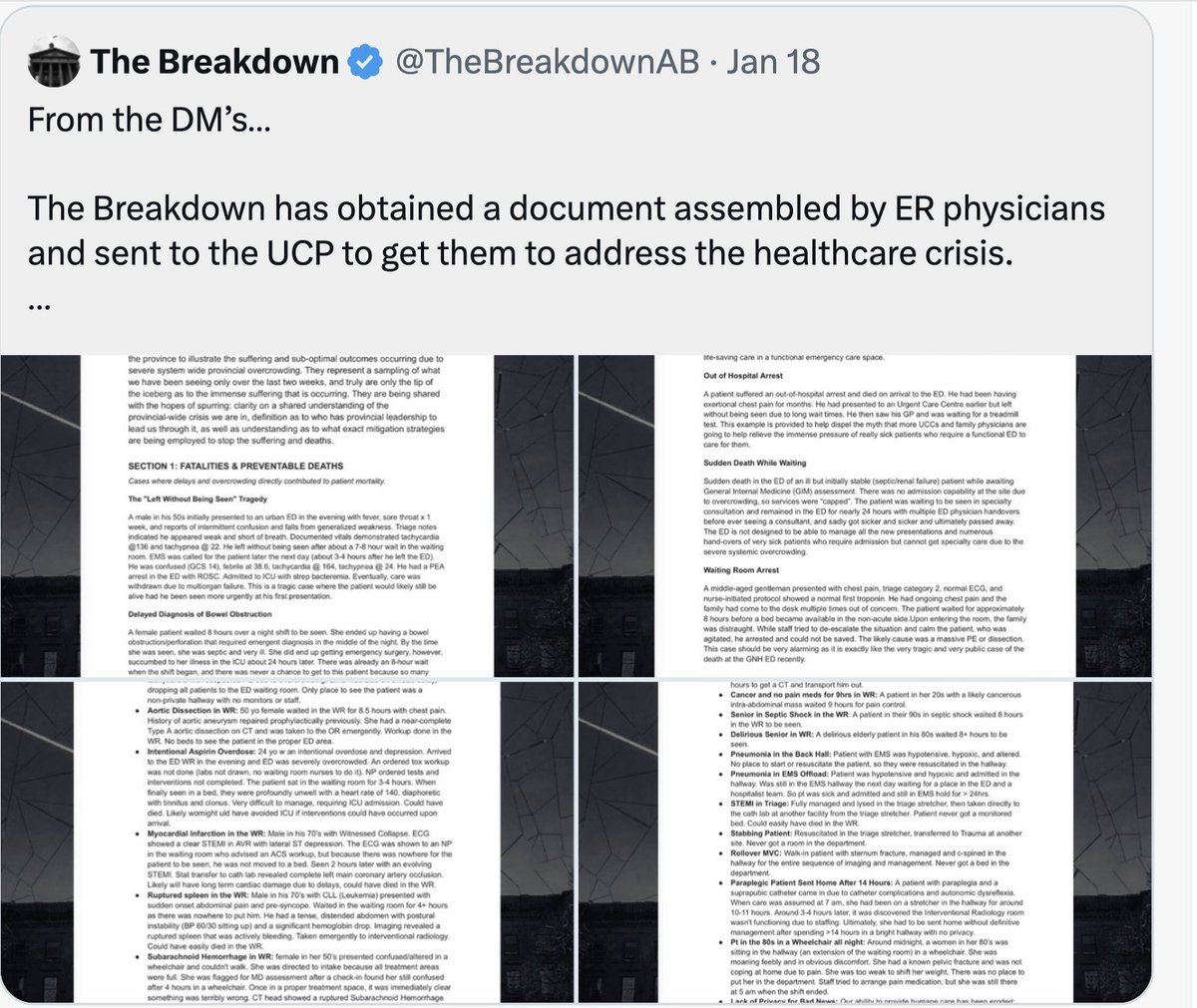
Albertans are suffering needlessly: leaving ERs without treatment, some later dying at home following delayed access, others arresting in hallways, or waiting 8 hours in septic shock.
Facts:
1. A tragic death in an ER on Dec 22 and many more documented cases since (see below).
2. Feb 1: Ministerial Jones acknowledged it is a crisis by introducing a Ministerial Order and “immediate TLP implementation.”
3. March 3: Roles remain unfilled and government is litigating this via media.
ERs remain in crisis mode, with CTAS 2s and 3s sitting in waiting rooms for hours and city ambulances transporting critically ill patients 30 km to small towns.
Two ministers (@AdrianaLaGrange and @MattJonesYYC) are involved in decisions on TLP (a highly specialized crisis protocol) without fully engaging those who designed and delivered it previously.
For context, I have worked on ER access crisis solutions over two decades as:
• Former Chair, HQCA
• Advisor to three health ministers
• Former Associate Minister of Health
• Former Emergency Medicine Section President
• Practicing ER physician who performed the TLP role
I respectfully urge Minister Jones to sit down with Dr. Warren Thirsk and Alberta’s emergency leaders, make a safe and rational decision grounded in frontline expertise, and implement this immediately.
The Minister is ready, as evidenced by the Ministerial Order. ER physicians are ready: with proper private space, dedicated nursing support, medico-legal clarity, and fair 2026 compensation for high-risk overtime work.
There is $1.4 billion in additional physician healthcare spending.
This fix costs only a few million out of a $34.4Billion budget. One serious lawsuit alone could exceed the difference between 2009 and 2026 compensation.
Decisions are best made from the bottom up:
1. AHS/Covenant administration/One Minister & frontline staff
2. Not top-down from Premier/Two Ministers/Two Sets of Bureaucrats & AMA President/AMA Board
Albertans deserve operational leadership now.
Attachments below:
1. AMA Letter
2. Verified & Documented bad outcomes
3. Aug/25 Hospital data: >100% capacity
4. Aug/25 data: Patients leaving without treatment
We can get this done, unless @ABDanielleSmith wants to "play chicken" to see who blinks first or she doesn't really want it done.
This is not a new rodeo. We have done this before.
#abhealth #abpoli #AbLeg
@PfParks@JMeddings@nenshi@UCPCaucus@Alberta_UCP@albertaNDP@AlbertaNDPHQ@ryanjespersen@cspotweet@TheBreakdownAB, despite t
A superb article by @BradenMannsYYC .
Worth reading every word. There is strong data that a parallel private system (such as AB is enacting) will worsen access to public healthcare.
That data comes from Cdn and international studies.
https://t.co/UcFPOklrw2
In a time where we seem to ignore the lessons history has taught us, here we go again ignoring the evidence. A parallel private-pay system will worsen access to publicly funded surgery | CMAJ https://t.co/QDva6LRbcN
“Alberta's flu season deadliest in recent memory…
“250 Albertans have died due to influenza as vaccination rates remain low”
The UCP sharply limited access to vaccines. They own this.
#abpoli#ableg#cdnpoli https://t.co/I8HvJwKVos
Wherein Smith claims that "newcomers" are costing the province $9 Billion in social programs.
In order for that to be true, every single newcomer would have to be accessing social programs that most don't even have access to.
These are evil misrepresentations.
#abpoli#ableg
This is absolutely shameful on the part of the UCP gov’t. The oncology phone line not only helps patients, but is cost effective. ERs are astronomically more expensive. Again, terrible governance by the UCP and reckless spending of our taxpayer dollars.
Remember this tomorrow when the UCP tables Budget 2026.
They will blame immigrants. They will blame WTI. They will blame Ottawa.
They won't blame sketchy health contracts. They won't blame separatist-related investment uncertainty.
It's everyone's fault but theirs #ableg
/1
https://t.co/Y2UIlxmBIJ
To be very clear: Minister LaGrange must not even know what Minister Jones is doing... because there has been NO "working very closely with AMA" on the TLP role. Minister Jones has not met with the AMA or with Emerg docs... NOTHING has happened by govt.
Even though the health care system is in crisis, the UCP shut down the Legislature early because they didn't want to talk about people dying in Alberta's emergency rooms.
We need solutions, not a government that shuts down debate.
Another Near Miss - govt aware, no response.
Pt in their 20s - with an intentional overdose and depression. Arrived to the ED WR in the evening and ED was severely overcrowded. An ordered tox workup was not done (no nurses to ensure labs drawn)
1/3
Long read - A very serious punchline is at the end.
I watched the Major Healthcare Announcement yesterday and, on the topic of the Triage Liaison Physician (TLP), I basically heard: “If ER doctors don’t want to do this job, we’ll get someone else.”
Let’s clarify what the TLP role actually is.
This is not a new innovation. It was created and staffed by emergency physicians during the last major ER crisis (2009–2014). At that time it was salaried, paid about 30% less than ER clinical shifts, required overtime, and carried significant medico-legal risk.
We stepped up anyway because during periods of low or no flow, critically ill Albertans in the waiting room required active surveillance and earlier intervention.
Patients should not deteriorate or die while waiting for care, something we have unfortunately recently seen and documented in overcrowded departments. When that happens, the human, legal, and financial consequences are serious.
The TLP role is not triage “support.” It is advanced emergency risk assessment.
It’s like a lifeguard monitoring 60–100 patients in a crowded waiting room and identifying who will deteriorate next.
That requires Emergency Medicine training.
Family physicians, NPs, and PAs are valued members of the team, but they are not trained to provide high-risk emergency triage oversight at this level in major trauma and referral hospitals.
For this role to function safely, three elements are required:
1. Reasonable compensation (even if below clinical shift rates)
2. A dedicated triage space beyond existing nursing capacity, with infrastructure support
3. Dedicated nursing support (RN + LPN)
It is my understanding that the compensation being discussed mirrors rates from 12–17 years ago. Cost estimates of the TLP program of $500–700K per ED (physician and nursing cost) annually likely underestimate the true cost.
When physician time, dedicated nursing support, infrastructure, and governance oversight are fully accounted for, a realistic estimate approaches $1 million annually per department in 2026 dollars.
This is a meaningful investment, but modest in the context of system-wide spending, particularly when compared to the potential human and legal costs of unmanaged risk in crowded waiting rooms.
Emergency physicians have been willing to do this role for two years and remain willing, even though it involves overtime, higher clinical and legal risk, and lower compensation than regular shifts. This is not about making doctors richer. It is about the safety of Albertans.
That said, the TLP does NOT fix hospital flow. It does NOT move ALC patients, create inpatient capacity, or accelerate movement of admitted patients to wards.
It is a harm-reduction measure, not a system solution. Until Minister @JasonNixonAB moves a significant number of ALC's out of hospital to reduce bed block, this position will be needed.
The underlying crisis remains blocked inflow, throughput, and outflow across our hospitals. If we want durable improvement, we must address system flow, not just triage optics.
There is also a governance concern.
Operational emergency department decisions have historically been made by hospital and clinical leadership. When the TLP was previously implemented, it was funded by AHS and Covenant because it improved patient safety and hospital performance.
It did not require direct political or bureaucratic direction by the Premier, Minister or their deputy ministers.
Clear separation between governance (policy and funding) and operations (clinical delivery) is essential in complex systems like healthcare.
Blurring those lines risks delay and confusion at the bedside, and in emergency medicine, delays are a matter of life and death.
This role was meant to be instituted urgently on Feb 1st in the context of a crisis, yet it is Feb 24th and discussion is still occurring publicly rather than through structured engagement with frontline leaders.
Dr. Warren Thirsk, the elected leader of the emergency physicians in Alberta, has previously worked this role. To my knowledge, he has not yet been formally consulted by Minister @MattJonesYYC regarding the TLP position.
It is also my understanding that two different ministers and their respective bureaucracies are responsible for this decision.
In the middle of a healthcare access crisis, urgent collaboration with frontline emergency leaders is practical and essential.
Rural Albertans depend on major urban hospitals for specialized care. When large centres are operating at or beyond capacity, transfers become difficult. We are all connected in this system.
@ABPremierSmith 's comments to "get someone else" are not helpful.
Premier, this is akin to saying, "if you cannot do the job of Premier, maybe we should hire someone else".
This should concern every Albertan.
@AdrianaLaGrange@Albertadoctors@AHS_media@CovenantCA@PfParks@JMeddings@NightShiftMD@TheBreakdownAB@ryanjespersen@cspotweet@Alberta_UCP@UCPCaucus@albertaNDP@nenshi
Have we forgotten this man who died in after an eight hour wait in an AB waiting room?
Danielle Smith promised to immediately have emergency triage doctors in place, feigning urgency.
Its been over a month, there hasn't even been a meeting about this, and Smith blames the AMA.