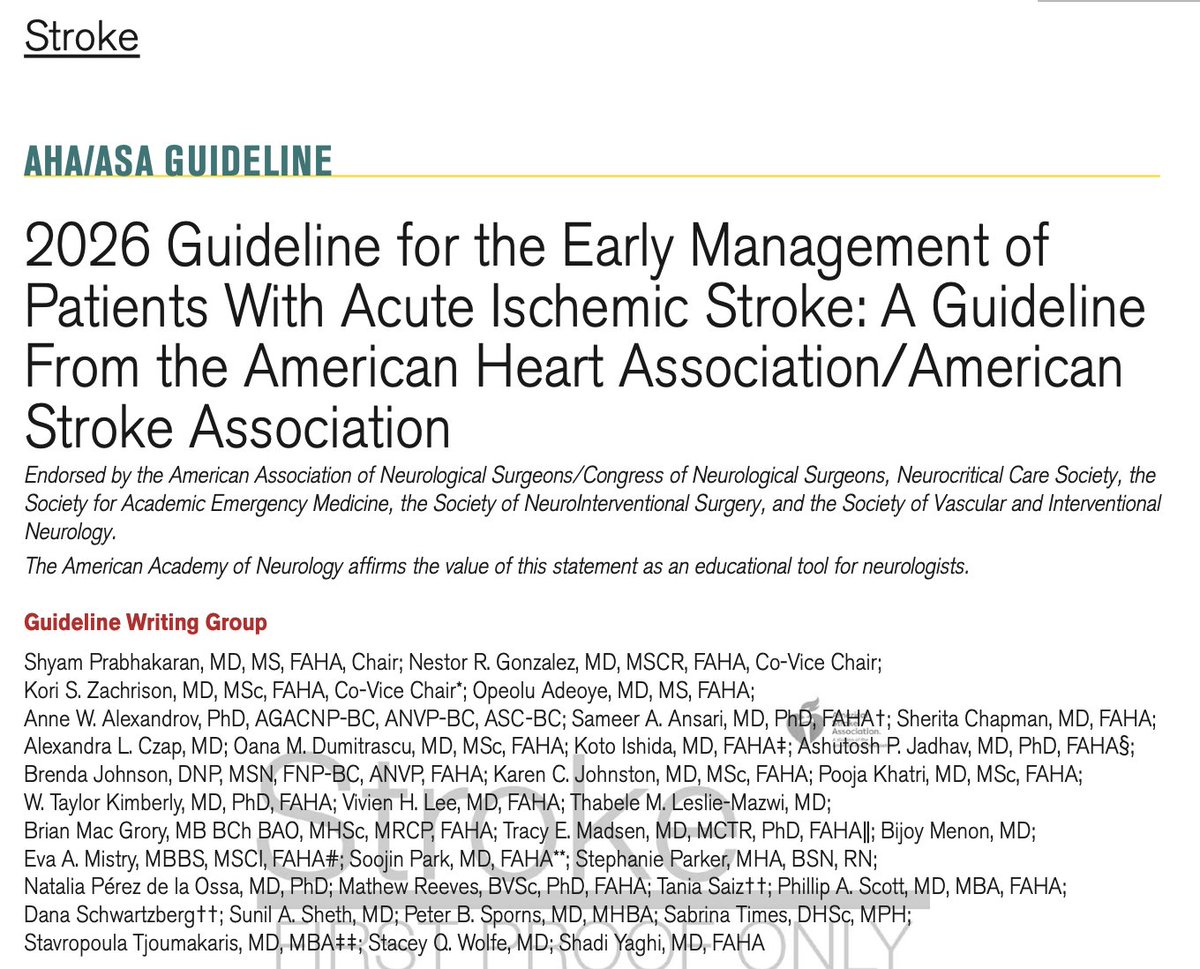
Recién salidas del horno: Guía AHA, 2026, de Evento Vascular Cerebral (EVC) Isquémico. Cambios o puntos relevantes:
🔴 Tenecteplase vs. Alteplase (Cambio Mayor) Se recomienda el uso de Tenecteplase (0.25 mg/kg, bolo único, máx. 25 mg) como una alternativa de primera línea, no inferior a la Alteplase, para pacientes elegibles en la ventana de 4.5 horas. Nota: La dosis de 0.4 mg/kg de Tenecteplase no se recomienda por falta de beneficio adicional y mayor riesgo de seguridad.
🔴 Ictus Leve No Incapacitante: En pacientes con déficits leves que no son incapacitantes (ej. síndrome sensitivo aislado, NIHSS bajo sin impacto funcional) dentro de las 4.5 horas, no se recomienda la trombolisis IV. Se prefiere la doble antiagregación plaquetaria (DAPT).
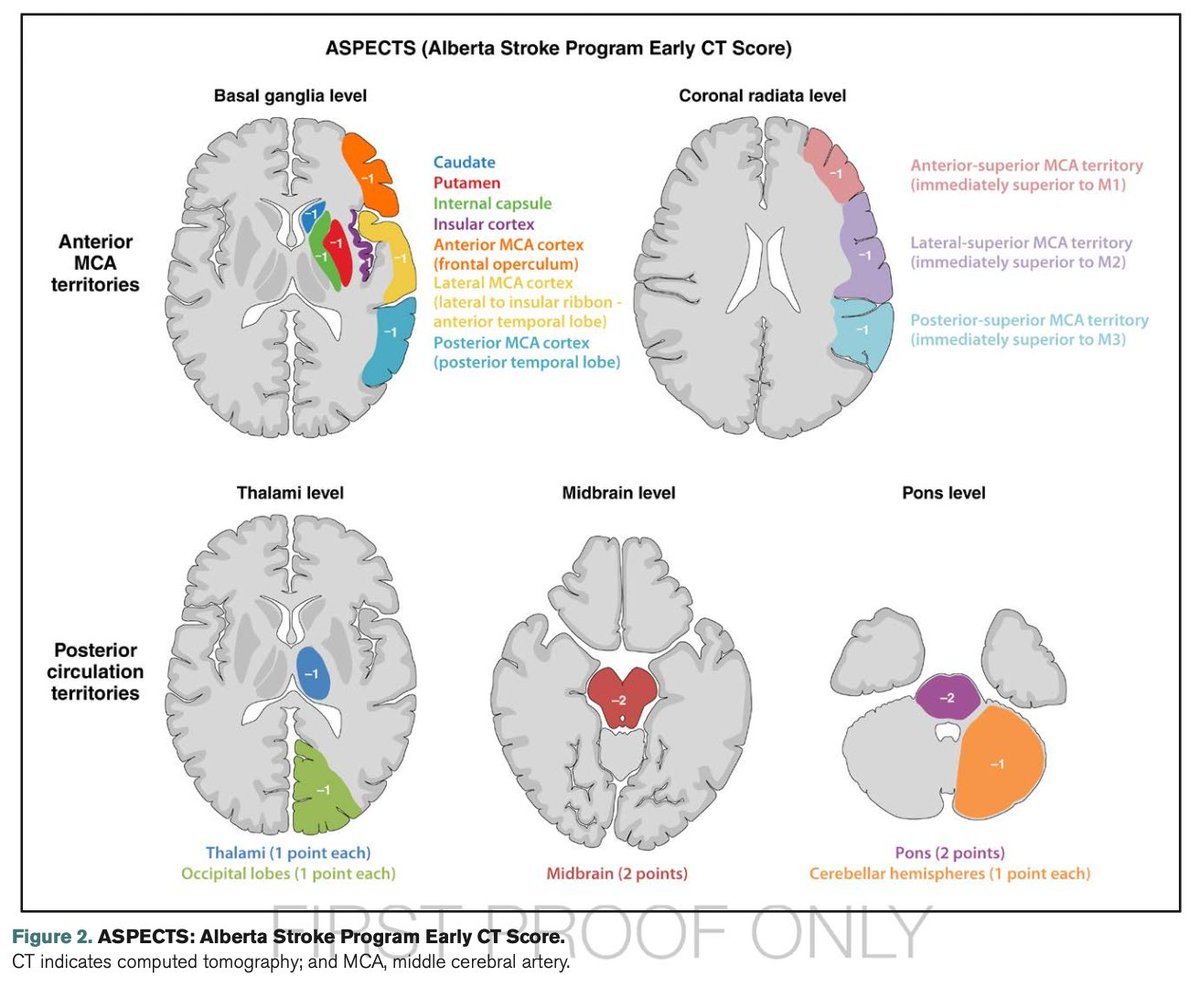
🔴 Trombectomía (EVT) en "Large Core": Se amplía la indicación de trombectomía mecánica para incluir pacientes con infartos de núcleo isquémico grande establecidos (ASPECTS 3-5), (antes eran excluidos).
🔴 Se desaconseja la reducción intensiva de la PAS (<140 mmHg) tras una reperfusión exitosa. Objetivo: TA <180/105 mmHg en las primeras 24 horas.
🔴 Oclusión de Arteria Basilar: realizar trombectomía en pacientes con oclusión de la arteria basilar a las <24 horas si NIHSS ≥10.
🔴 Control Glucémico: mantener entre 140-180 mg/dL.
🔴 Ventanas Extendidas de Trombolisis: Se recomienda el uso de trombolisis IV en ventana extendida (4.5 a 9 horas o ictus del despertar) en pacientes seleccionados mediante imagen avanzada que demuestre mismatch (DWI-FLAIR o Perfusión).
🔴 Nuevas Guías Pediátricas: Por primera vez se incluyen recomendaciones específicas para pediatría
Vamos a revisarlas a fondo para actualizar las apps.
🚨 BREAKING — CREST-2 Changes the Game in Asymptomatic Carotid Stenosis
A landmark NEJM paper (Nov 2025) delivers the most rigorous evidence to date on how to manage ≥70% asymptomatic carotid stenosis — and the results will ignite global discussion. 🔥🧠
🔍 What CREST-2 found
Across 2 parallel randomized trials, comparing intensive medical therapy (IMT) vs. Carotid Stenting or Carotid Endarterectomy (CEA):
🩺 1️⃣ Stenting Trial
Primary outcome at 4 years:
IMT alone: 6.0%
Stenting + IMT: 2.8%
➡️ 53% relative risk reduction
NNT ≈ 31
More peri-procedural events with stenting (1.3% vs 0%), but much fewer long-term ipsilateral strokes.
🔧 2️⃣ Endarterectomy Trial
Primary outcome at 4 years:
IMT alone: 5.3%
CEA + IMT: 3.7%
❌ Non-significant difference (P=0.24)
Trend favors CEA but underpowered to prove superiority.
⭐ Strengths of CREST-2
💪 Rigorous design: Two parallel RCTs, observer-blinded primary outcome adjudication.
🌍 Large, multinational cohort: 2,485 patients across 155 centers.
📈 Excellent risk-factor control: IMT arm achieved LDL <70 mg/dL and SBP <130 mmHg in the majority (Figure 1, pages 6–7).
🧠 High-fidelity event capture: Stroke adjudicated with MRI preferred (82%), improving sensitivity vs. prior studies.
🔬 Modern therapies included: PCSK9 inhibitors, updated BP targets, structured lifestyle intervention.
⚠️ Limitations to consider
🧪 Operators were high-volume, certified experts — results may not generalize to all centers.
⌛ Outcome affected by evolving medical therapy: Improved BP, LDL, diabetes & obesity treatments may reduce incremental benefit of revascularization.
🧭 No evaluation of transcarotid revascularization (TCAR): Now widely used but not incorporated.
🔍 Periprocedural risk remains: Especially for stenting (1.3%) and CEA (1.5%).
📉 Borderline tipping-point analyses: A few additional or removed events could shift significance — especially for stenting.
🧩 Some post-procedure strokes may not be carotid-related, limiting causal inference.
🧩 Take-home message
For asymptomatic ≥70% carotid stenosis:
Stenting + IMT → significant reduction in 4-year stroke risk, despite a small procedural risk.
CEA + IMT → trend to benefit, but not significant.
Intensive medical therapy performed exceptionally well — far better outcomes than historical controls.
The debate isn’t over — but CREST-2 redefines the landscape.
Stroke prevention will never be the same. 🔄🧠✨
🧠 Tongue tremor is rare in most CNS infections but occurs in up to 30% of patients with tick-borne encephalitis.
Watch the video and read the case:
🔗 https://t.co/ZcGwU3YyLj
#neurotwitter#neurology#infectiousdisease#MedEd
Have you been missing the 'head snap sign?' It is a subtle but important clinical observation that is expanding our understanding of tremor. The head snap sign, first described in essential tremor, may actually reach beyond essential tremor into thalamic tremor and possibly other disorders.
Key points:
- The head snap sign is an involuntary jerk-like head motion observed during finger to nose testing and has been traditionally linked to essential tremor.
- A new case demonstrates that the sign can also occur w/ thalamic tremor following brain injury.
- The finding suggests the sign may be under-recognized and not completely exclusive to essential tremor.
My take: If you haven't appreciated this sign during essential tremor, you are missing cases. It makes sense that the movement is underpinned by the circuitry and would not be exclusive to essential tremor. 1- The head snap sign is a quick head jerk seen during coordination testing. 2- It is different from regular head tremor which is rhythmic and ongoing. 3- Health care providers once thought it was only seen in essential tremor however, it may appear in other tremor conditions. This observation reminds us how complex tremor and movement disorders really are. 5- Of course I will say more studies are needed so we can better understand and not misclassify these movements.
https://t.co/dfuwvQe4z8 #tremor @tremorjournal@movedisorder@AANmember@SfNtweets@FixelInstitute@ParkinsonDotOrg
Myoclonus-dystonia: will you know it when you see it? T-minus 3 days and counting to the Aspen Movement Disorders Course. Myoclonus-dystonia is a fascinating and frequently under-recognized movement disorder characterized by quick shock-like jerks called myoclonus that are paired with twisting or abnormal postures called dystonia. Myoclonus-dystonia typically affects the upper body, however it is not exclusive to the upper body. It’s commonly linked to SGCE gene mutations and may be alcohol-responsive, which can be a diagnostic clue. The differential includes essential myoclonus, juvenile Huntington’s, Wilson’s disease, mitochondrial disease, metabolic disorders, and functional movement disorders. Always think genetic, think metabolic and don’t forget that these patients frequently have psychiatric comorbidities like anxiety or OCD. Always get a brain MRI scan. Bonus causes include: 1- DYT-KCTD17 (formerly DYT26) as an early-onset myoclonus-dystonia. This one is severe and progressive. 2- ADCY5 mutations w/ possible facial dyskinesias, chorea, dystonia and myoclonus. This form may fluctuate and worsen w/ sleep. 3- GCH1 mutations or dopa-responsive dystonia. 4- Cerebellar ataxia syndromes such as SCA2 and SCA17. 5- Mitochondrial disorders like MERRF or myoclonic epilepsy with ragged red fibers. 6- Lysosomal storage diseases such as GM1/GM2 gangliosidosis or Niemann-Pick type C. If we miss you on July 27th-August 1st watch our social media channels for tips on diagnosing and treating movement disorders. @movedisorder@FixelInstitute@ParkinsonDotOrg
Clinical Clue from Dr. Abhimanyu Mahajan: Learn how to recognize mirror movements in early PD and how they may differ in corticobasal syndrome. @AMahajanMD
¡Orgullosos de estar entre los 3 mejores servicios de Neurologia de esta país en el monitor de reputación sanitaria!
Un reconocimiento al esfuerzo, dedicación y trabajo en equipo de todos nosotros.
💪 #Equipo@mercoranking@H12Octubre
Acute nutritional axonal neuropathy (dry beri-beri) is more common than many believe.
In patients with malnutrition, intractable vomiting, heavy alcohol use, or a poorly balanced diet, this condition is more likely than Guillain-Barr�� Syndrome (GBS). #NeuropathyBites
1/
Inauguramos las nuevas instalaciones del área de neurología en el nuevo hospital. Y nos despedimos de un lugar donde, por más de 50 años, formamos generaciones de neurólogos. Con ilusión y pasión, afrontamos este nuevo reto en la Hospitalización y en la nueva Unidad de Ictus 😊👏
@seneurologia Disculpad el canal, no sabía por dónde dirigirme a vosotros. Dadas las condiciones en Valencia, ¿habría posibilidad de presentaciones online opcionales para los que tengamos comunicaciones y nos planteemos la presencialidad? Un saludo y muchas gracias.
Julio Anguita: ¿Qué es libertad?
Cuánto echamos de menos al gran Julio Anguita. Aquí da una brillante explicación de qué significa libertad, pero libertad de verdad, no la que piden Ayuso y demás fauna de derecha extrema y de extrema derecha.