Creatine is known for building muscle and improving athletic performance. A new UCLA study just found it does something completely different—it powers the immune cells that direct your body's cancer-fighting response.
Researchers published the findings in iScience after studying both mouse models and human cells. The discovery builds on earlier work showing creatine fuels killer T cells that attack tumors directly. Now they've found creatine also energizes dendritic cells—the immune cells that capture tumor fragments and train T cells where to strike.
Most cancer immunotherapies target killer T cells directly, but only 20-40% of patients respond. The limitation isn't the T cells themselves. It's the dendritic cells upstream that activate and direct them.
The research team started by examining which metabolic genes were most active in dendritic cells that had infiltrated tumors in mice. One gene stood out: the creatine transporter, which pulls creatine into cells. It was markedly elevated in tumor-infiltrating dendritic cells compared to those in healthy tissue.
To test whether this mattered, they engineered dendritic cells that couldn't transport creatine. These cells showed impaired survival, reduced activation, and weakened ability to prime T cells for tumor response. When grown alongside T cells in a lab dish, those T cells divided less and produced fewer cancer-fighting signaling molecules.
Then they tested the opposite intervention—increasing creatine instead of removing it. Daily creatine injections in melanoma-bearing mice significantly slowed tumor growth and boosted both the number and activation of dendritic cells infiltrating tumors. The creatine-treated dendritic cells produced higher levels of chemical signals that recruit additional immune cells to the tumor site.
Metabolomics analysis revealed the mechanism: creatine supplementation raised intracellular ATP levels in dendritic cells. ATP is the energy currency cells use to power nearly every function. Creatine acts like a battery—storing and releasing energy on demand, helping dendritic cells maintain stable energy levels even when competing with fast-growing tumor cells for nutrients.
The effect extended to human cells. Creatine treatment enhanced activation of human monocyte-derived dendritic cells—the type often used in dendritic cell cancer vaccines—and improved their ability to stimulate human T cells against cancer-associated targets.
The findings suggest incorporating creatine during manufacturing of dendritic cell vaccines may boost their therapeutic potency. More broadly, they reveal that creatine doesn't just help the immune cells fighting cancer directly—it energizes the infrastructure that supports and guides them.
Immuotherapy works for some patients but fails for most. The difference may come down to whether dendritic cells can maintain enough energy to properly activate the T cell response. Creatine supplementation addresses that metabolic constraint.
A supplement taken by millions for muscle growth and athletic performance turns out to support immune cell function at a fundamental metabolic level—powering both the killer T cells that attack tumors and the dendritic cells that train them where to go.
¿Estás pensando en salir fuera este verano y eres paciente con #EPOC o asma? El Dr. @CMLChang, especialista de nuestro Servicio de Neumología, ofrece las claves para viajar con seguridad teniendo una enfermedad respiratoria crónica
🔗 https://t.co/8hs1jEW9F4 vía @Copedelasierra
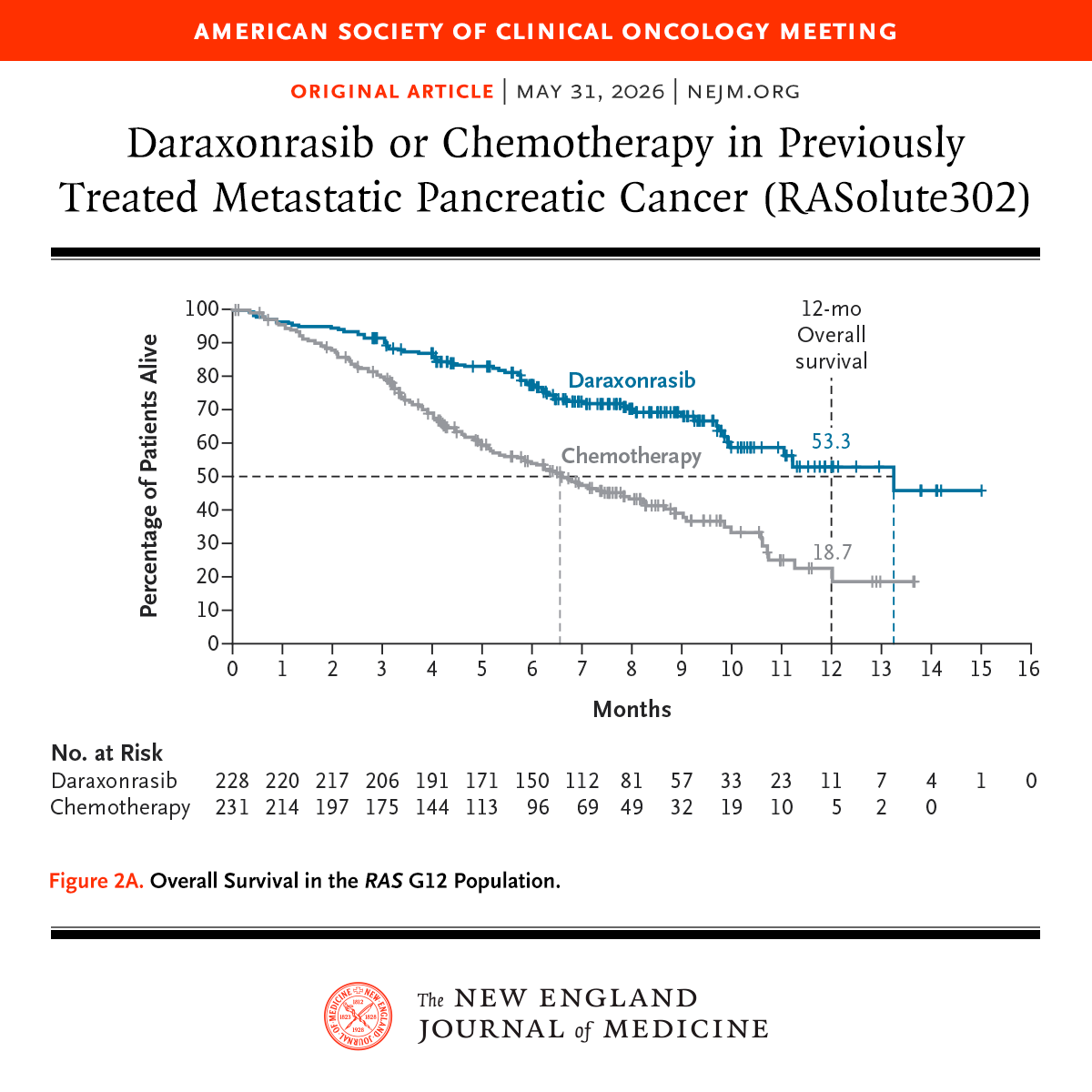
Presented at #ASCO26:
Among patients with previously treated metastatic pancreatic ductal adenocarcinoma, the RAS(ON) inhibitor daraxonrasib led to significantly longer overall survival and progression-free survival than chemotherapy. Full phase 3 RASolute 302 trial results: https://t.co/xwLWBZYRzq
@ASCO
Me entristece mucho saber que los viajeros españoles del MV Hondius, en su trayecto hacia Canarias, han expresado a las autoridades del Ministerio de Sanidad que “tienen miedo e inquietud sobre si hay oposición a su llegada”.
Es de vergüenza ajena la posición de cierto sector político que desconoce completamente el significado de la palabra solidaridad.
Y luego van dándose golpes de pecho en su falso cristianismo e intentan engañarte con lo de su “prioridad nacional”. Lo suyo es lo del “sálvese el que pueda”.
Nuestro hospital implementa el primer dispositivo médico inteligente que permite controlar y personalizar la oxigenoterapia en tiempo real
🔗 https://t.co/xVpuBee51P
La diferencia del Lactato Arterial y Venoso positiva se asocia a mortalidad en ARDS… novedoso… del Prof. Jesus Sanchez Diaz
Descarga gratis:
https://t.co/rjxIm14Qvq
Consenso Delphi por Expertos sobre ASINCRONÍAS en Ventilación Mecánica 🫁
🫁 Doble Disparo, Trigger Reverso (tal vez) y Esfuerzo Inefectivo se asocian a Más Días de VM
🫁 Flujo Insuficiente, Ciclado Prematuro y Ciclado Retrasado se asocian a Disconfort (las otras también)
https://t.co/EpzXcWg7Uj
Ante una hemoptisis, conviene ordenar el diagnóstico diferencial en 3 grandes bloques:
🔹 Vía aérea
🔹 Parénquima
🔹 Vasos pulmonares
Una forma sencilla de no olvidar causas frecuentes y causas potencialmente graves.
#NeumocitoCurioso#Hemoptisis#Neumología
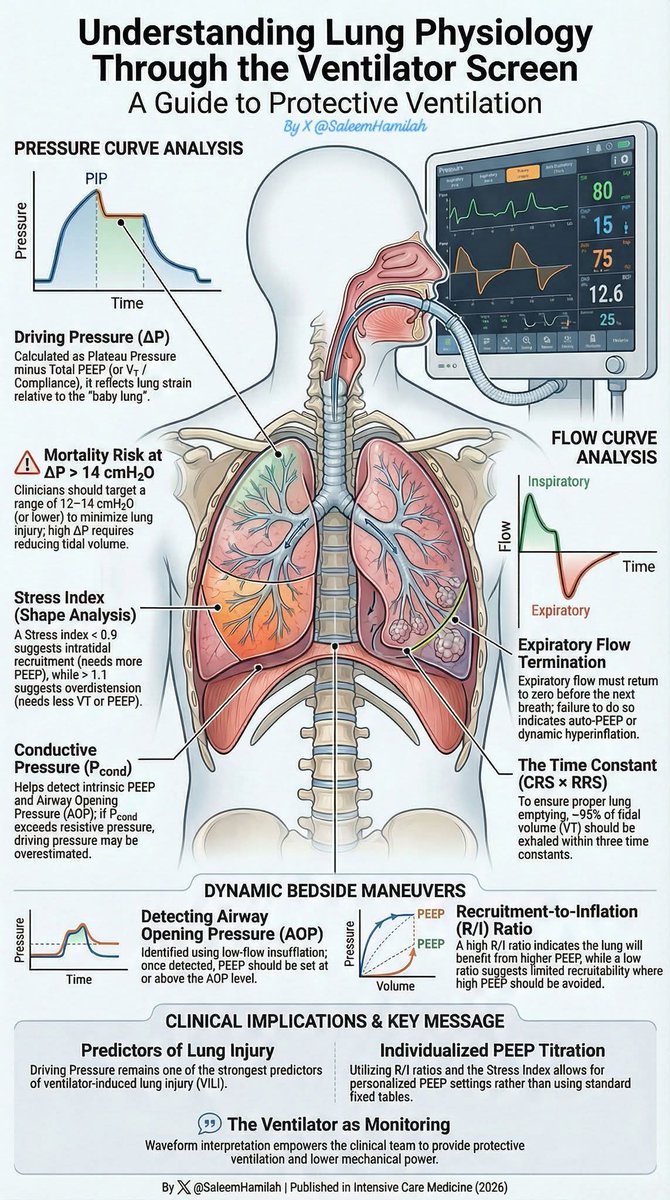
Understanding Lung Physiology Through the Ventilator Screen
💡 The ventilator screen is continuous physiological monitoring.
Interpreting pressure and flow curves allows:
🛡 Protective ventilation
🎯 Individualized PEEP
📉 Lower mechanical power
🫁 Reduced risk of VILI
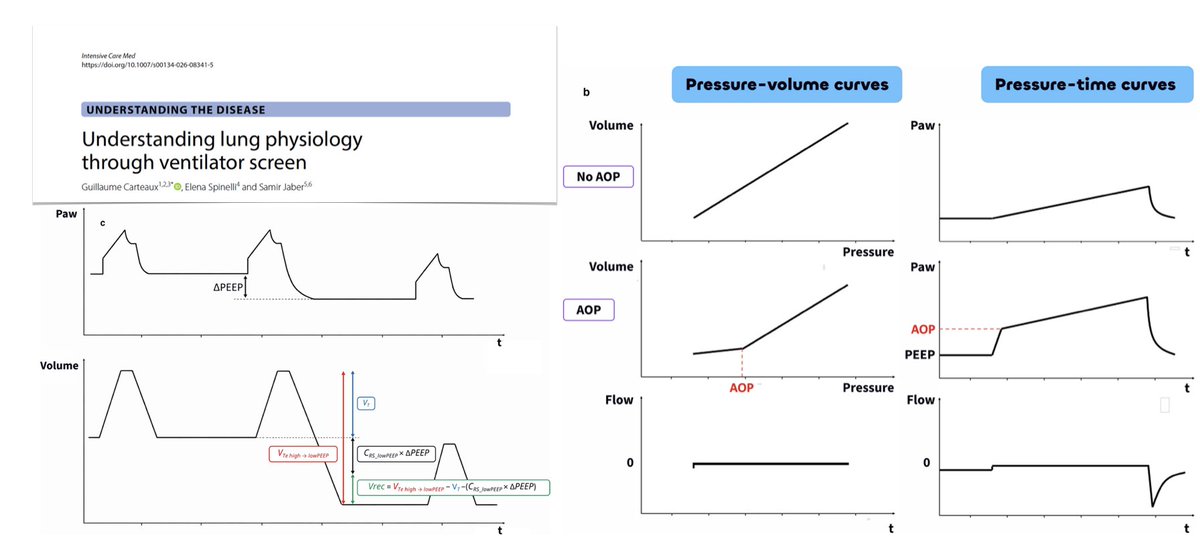
Understanding lung physiology through ventilator screen
🫁 airway pressure waveform at a glance: respiratory system equation of motion, conductive pressure, stress index, driving pressure
🌊 flow waveform during pressure-controlled ventilation
💨 expiratory flow and the time constant of the respiratory system
🛌 dynamic bedside maneuvers: airway opening pressure, recruitability & recruitment-to-inflation ratio
🚧 the way forward
#FOAMcc
🔓 https://t.co/TzWW9gtLOB
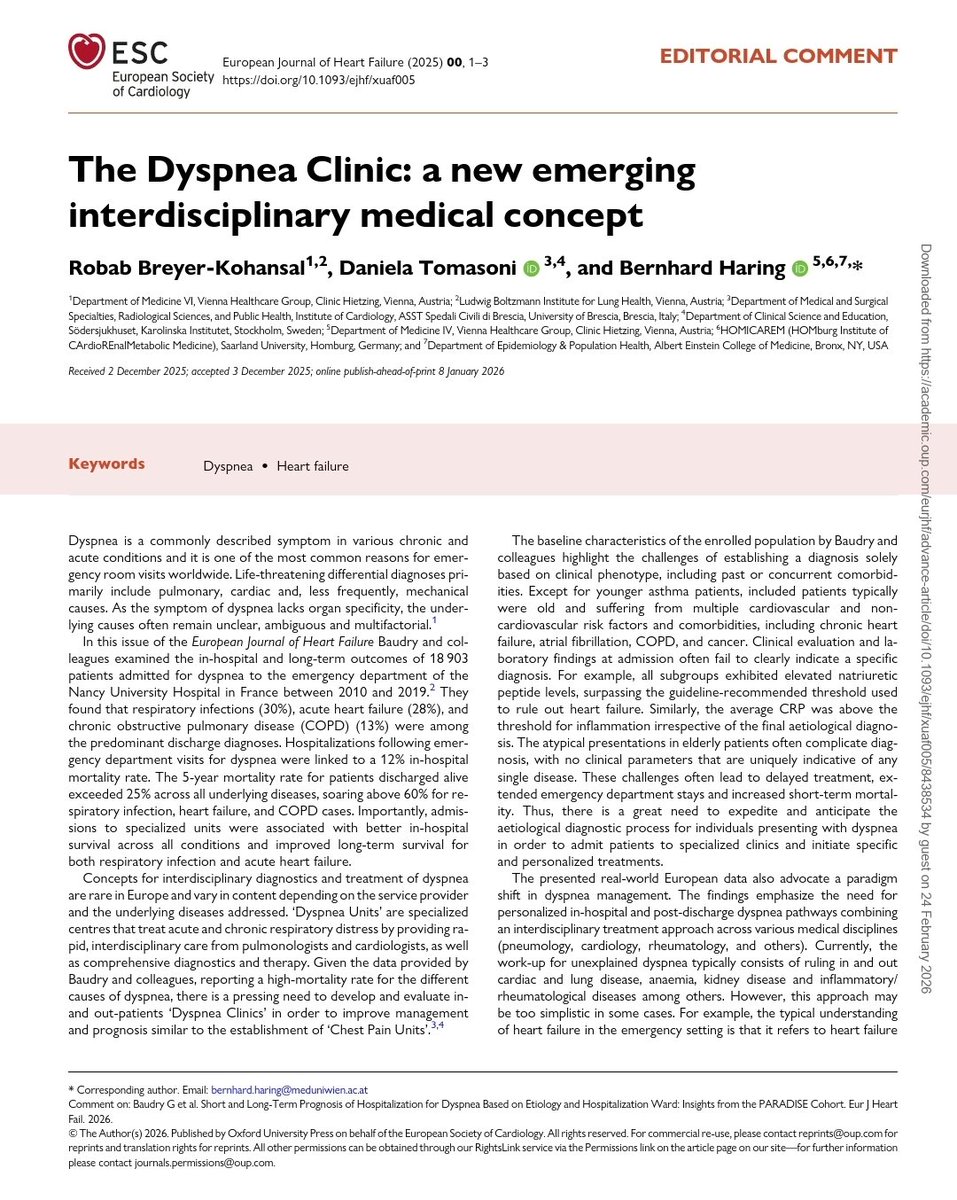
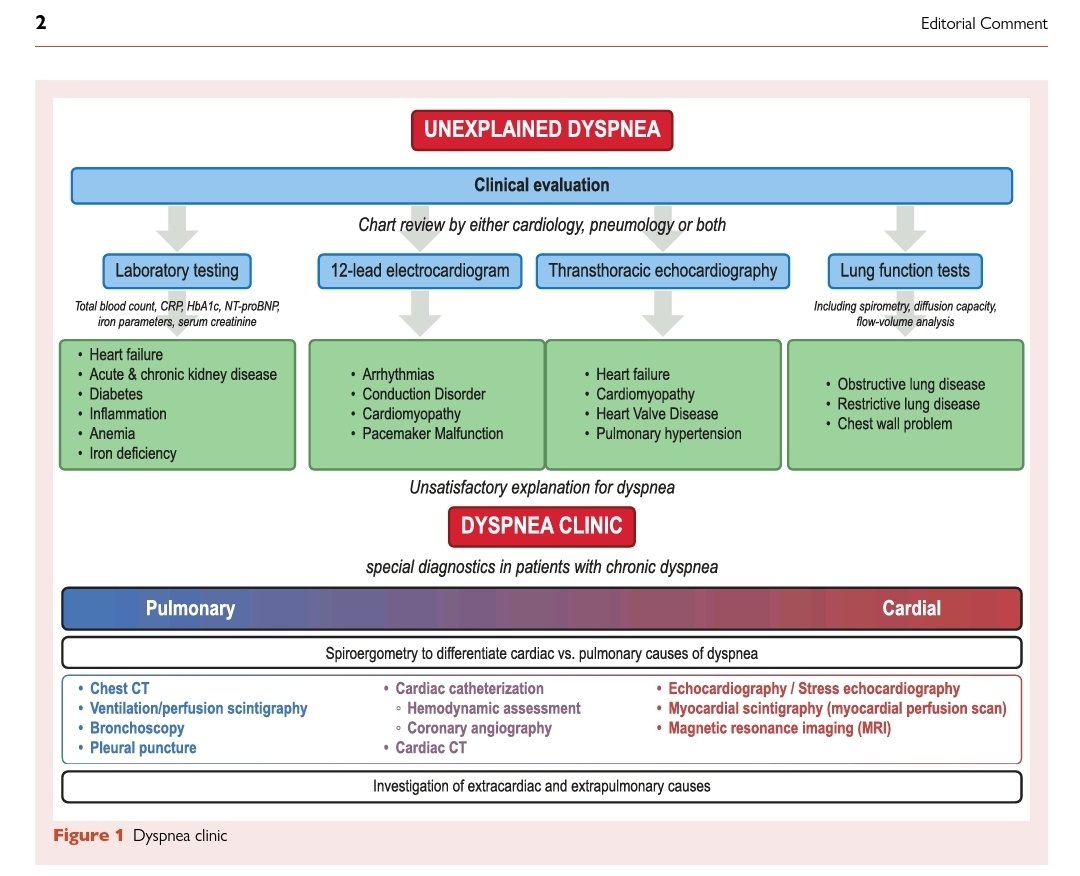
📌 ¿La disnea es solo un síntoma… o estamos frente a un síndrome de alta letalidad mal abordado?
✅El editorial “The Dyspnea Clinic: a new emerging interdisciplinary medical concept”, publicado en European Journal of Heart Failure, plantea un cambio de paradigma urgente en el abordaje de la disnea. 👇
🔎 1️⃣ La magnitud del problema
Basado en la cohorte PARADISE (18.903 pacientes en urgencias por disnea):
📊 Diagnósticos principales:
⚠️Infección respiratoria: 30%
⚠️Insuficiencia cardiaca aguda: 28%
⚠️EPOC: 13%
⚠️ Mortalidad intrahospitalaria: 12%
⚠️ Mortalidad a 5 años: >25% en todas las etiologías
⚠️ En IC, infección respiratoria y EPOC: >60%
👉 Conclusión: La disnea NO es un motivo banal de consulta. Es un marcador de alto riesgo.
🧠 2️⃣ El gran problema clínico: la ambigüedad diagnóstica
✅La disnea es inespecífica por órgano.
✅En pacientes añosos y pluripatológicos:
➡️Péptidos natriuréticos elevados en múltiples etiologías
➡️PCR elevada sin especificidad
➡️Presentaciones atípicas
➡️Comorbilidades superpuestas
❗ Error frecuente en urgencias: Si la FEVI es normal → se descarta insuficiencia cardiaca.
✅Pero la IC con fracción de eyección preservada (HFpEF) es altamente prevalente en >75 años.
👉 La ausencia de edema o estertores NO excluye insuficiencia cardiaca. 👉 El NT-proBNP sigue siendo clave para rule-out / rule-in precoz.
🏥 3️⃣ Propuesta disruptiva: “Dyspnea Clinics”
✅Inspiradas en las Chest Pain Units.
✅Una Dyspnea Clinic integraría:
🫁 Neumología
❤️ Cardiología
🩸 Evaluación metabólica e inflamatoria
🖥️ Ecocardiografía avanzada
🏃 Prueba de esfuerzo cardiopulmonar
🫀 Cateterismo derecho con ejercicio
📸 TAC de tórax cuando esté indicado
🎯 Objetivo:
✅Reducir retraso diagnóstico
✅Mejorar asignación a unidades especializadas
✅Optimizar tratamiento personalizado
✅Impactar supervivencia a largo plazo
🫀 4️⃣ El punto fino fisiopatológico
✅El cateterismo derecho + CPET permite detectar:
✅Hipertensión pulmonar oculta
✅HFpEF con alteraciones hemodinámicas solo inducibles por esfuerzo
✅Insuficiencia mitral dinámica
✅Alteraciones de gasto cardiaco no evidentes en reposo
👉 Muchos pacientes etiquetados como “disnea inexplicada” tienen patología hemodinámica subdiagnosticada.
💉 5️⃣ Prevención cardiovascular vía vacunación
🫁Uno de los mensajes más potentes del editorial:
✅Las infecciones respiratorias aumentan eventos CV.
🦠 Influenza → ↑ hospitalización por IC
🦠 SARS-CoV-2 → ↑ eventos CV
🦠 RSV y neumococo → ↑ morbimortalidad CV
La vacunación: ✔ Reduce infección
✔ Reduce eventos cardiovasculares adversos
✔ Actúa como prevención CV secundaria
✅La prevención también debe integrarse al modelo de disnea.
🔄 6️⃣ Cambio de paradigma
✅Actualmente:
“Descartar pulmón vs corazón”
🫁Nuevo modelo:
🔬 Evaluación interdisciplinaria estructurada
📈 Vías clínicas post-alta
🧭 Seguimiento dirigido por etiología
🛡️ Prevención intensiva
🫁La disnea debe considerarse un síndrome complejo de alto riesgo, no solo un síntoma.
📢 Para reflexionar🩺
✅Si la mortalidad a 5 años supera el 25% en todos los grupos… ¿por qué no tenemos clínicas estructuradas de disnea como tenemos para dolor torácico?
✅Este editorial es un llamado a reorganizar sistemas de salud.
🔎 Sígueme en X → @rksanti
📚 Únete al grupo de Telegram →https://t.co/VwX4ZJAhRe
What’s optimal PEEP for your patients with an increased BMI?
Our study showed a simple equation you can use:
PEEP = BMI/3
There’s variability, but BMI/3 approximates the mean optimal PEEP (by esophageal manometry) from BMI 25 to > 40
#foamcc
https://t.co/qwHioxtP6H
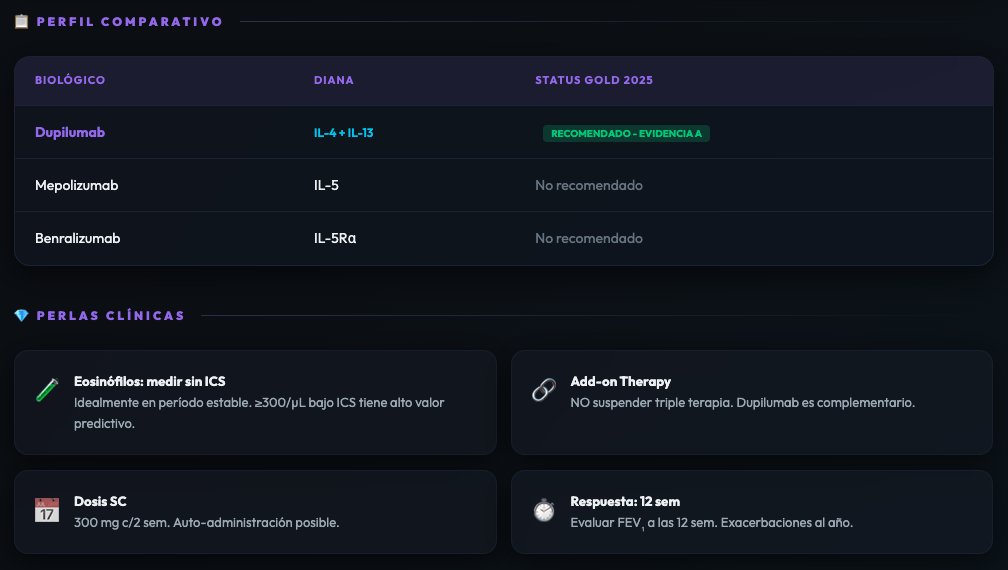
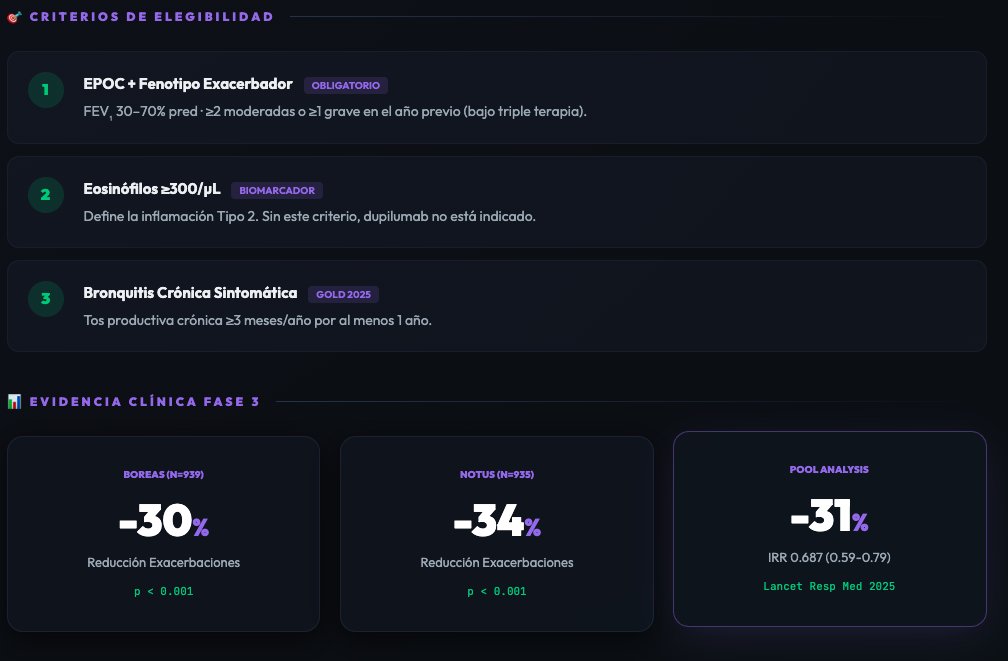
🫁 Dupilumab en EPOC — lo que necesitas saber antes de indicarlo:
✅ Eos ≥ 300/µL → obligatorio ✅ Triple terapia → mantenerla como base ✅ Bronquitis crónica → parte del criterio ✅ ≥ 2 exacerbaciones → sobre terapia óptima
Resultado: ↓31% exacerbaciones · +83 mL FEV₁ desde sem 12
No es para todos. Es para el paciente correcto.
▶ https://t.co/gXbU54ntXv
🚨Se acaba de publicar la primera guía de la AHA/ACC sobre embolia pulmonar aguda.
Y tiene 75 páginas 📄
Te hemos resumido los 10 puntos clave que destacan las guías, con ilustraciones y explicaciones.
Dentro hilo 👇🏼1/12