Interventional Cardiologist/Cardiology 🫀/ Internal Medicine Physician 🩺/Facultad de Medicina. U.N.A.M. 🇲🇽 - Miembro de la Sociedad Europea de Cardiología
➡️ Angioplastia coronaria diferida o inmediata en enfermedad multivaso en IAM guiada por iFR (iMODERN Trial)
Oscar Manuel Granados Casas @cobygc
Lee el comentario completo: https://t.co/Bz5dGsbtHb
🫀 En IAMCEST multivaso, la ICP inmediata guiada por iFR no fue superior a la estrategia diferida guiada por resonancia magnética de estrés en el combinado de muerte, reinfarto u hospitalización por IC a 3 años (~9,3% vs 9,8%).
🧪 La estrategia iFR llevó a tratar muchas más lesiones no culpables (ICP en el 42,6% vs 18,7% de los pacientes) sin traducirse en más beneficio clínico.
🧲 Se registraron más eventos adversos graves en el grupo guiado por resonancia magnética (181 vs 145 pacientes).
🧠 Las diferencias entre iFR (gradiente epicárdico) y resonancia magnética (perfusión miocárdica) recuerdan que ambas técnicas valoran la isquemia de forma distinta y condicionan la selección de lesiones a revascularizar.
🧵 Sodium bicarbonate did not improve sustained return of spontaneous circulation, survival, or neurologic outcomes in adults with in-hospital cardiac arrest compared to placebo.
#CCR26@CritCareReviews
https://t.co/2KJGJOlyHu
-Ocular ☢️ of the IC from a radial approach - J of Invasive🫀
-LRA vs RRA ☢️ exposure of the IC, Circulation
-Influence of height on ☢️ exposure of the IC , American Journal of Cardiology
-LRA vs RRA operator ☢️ exposure
1st Meta analysis, 🇺🇸🫀journal
NAPs roles evolving 😁
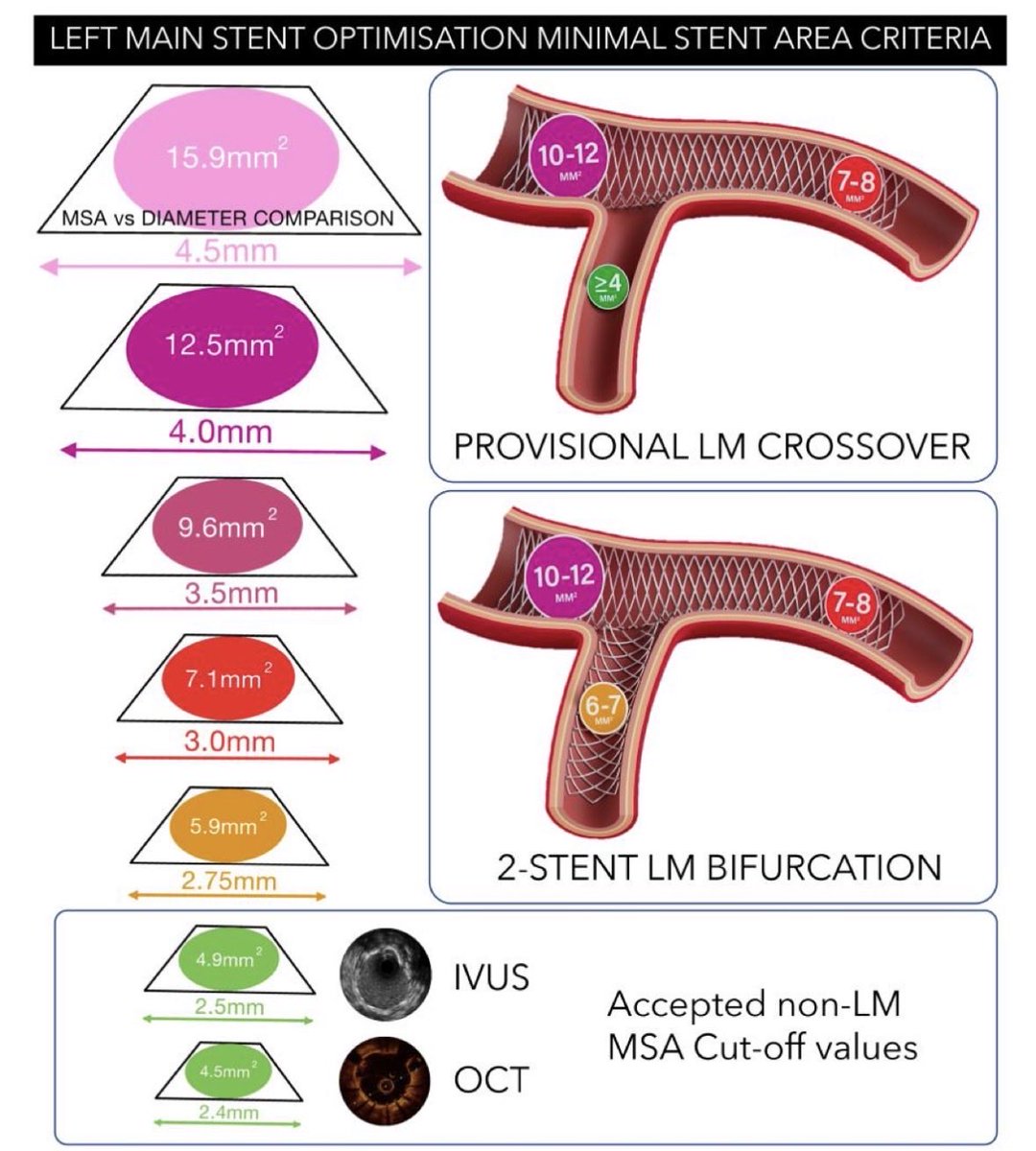
After 2 years of work, the 🇪🇺 consensus on #IVUS#OCT use in #LM#PCI is now published in #EHJ. Great international collaboration coordinated by #EBC and #EAPCI !!!
It includes fantastic practical images that can be hung on the walls of all cath labs…
https://t.co/2TbBTIoMxu
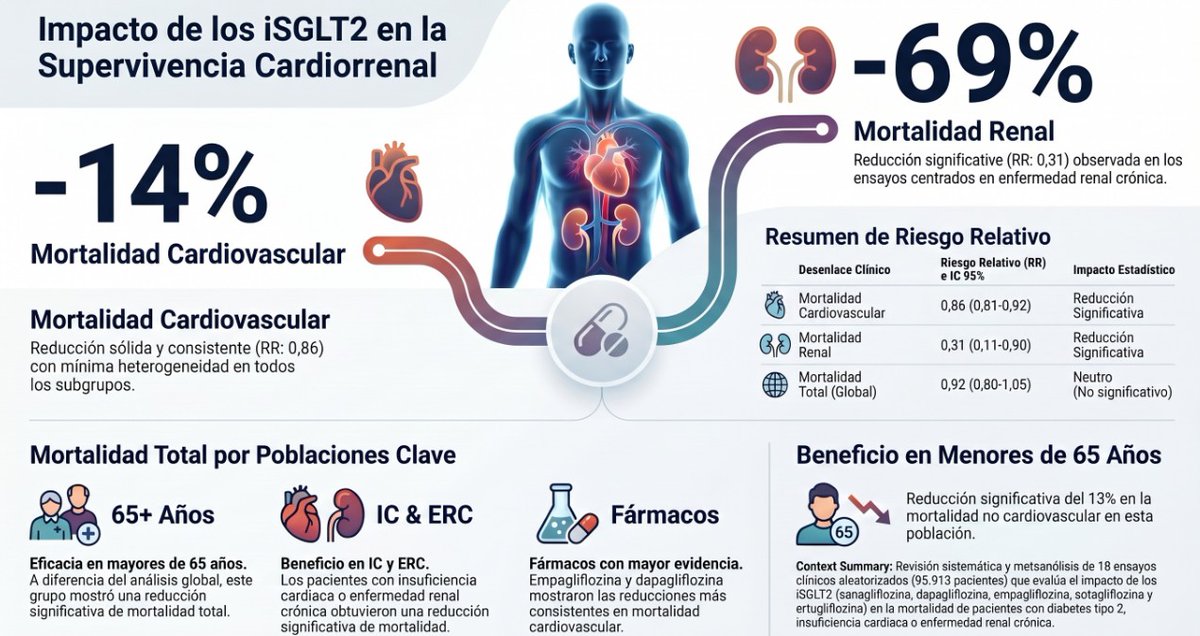
Casi 96.000 pacientes y 18 ensayos aleatorizados después, los datos sobre iSGLT2 y mortalidad son más claros que nunca.
📖 Accede al análisis completo en CardioTeca. https://t.co/leAk3otpHV
❤️ Reducción del 14% en mortalidad cardiovascular, con efecto consistente en todos los subgrupos de edad.
🫘 Mortalidad renal reducida un 69% en pacientes con enfermedad renal crónica.
👴 Mayores de 65 años: beneficio significativo también en mortalidad total.
💊 Empagliflozina y dapagliflozina, los fármacos con mayor respaldo en supervivencia.
PCI and Stenting for Treatment of Myocardial Muscle Bridges | JIC
“PCI & stent for symptomatic muscle bridges performed with physiological and intracoronary imaging assessment and guidance may be an acceptable management modality for symptomatic MB pts” https://t.co/09UZB7F2Go
📰 Lo mejor del congreso europeo de insuficiencia cardíaca 2026 en Barcelona
No te pierdas los hallazgos con mayor impacto científico del HFA-ESC 2026. Lee el artículo completo aquí: https://t.co/6sTJ0yn5h7
💊 El ensayo SUBCUT HF II demostró que la furosemida subcutánea en domicilio acorta el ingreso una media de 5,5 días con eficacia y seguridad equivalentes a la vía intravenosa hospitalaria
🫀 El metaanálisis de DECISION, DIGIT-HF y DIG (más de 9.000 pacientes) respalda los glucósidos digitálicos a dosis bajas como opción adicional eficaz y segura en IC con FEVI reducida o levemente reducida
🧬 El ensayo HF-REVERT, primer ensayo de inhibición de microARN en IC, no alcanzó su variable principal, aunque el perfil de seguridad del oligonucleótido CDR132L fue satisfactorio
📡 El estudio EXCALIBUR confirma que las arritmias clínicamente significativas son frecuentes y a menudo asintomáticas en la amiloidosis cardíaca, reforzando la monitorización prolongada en estos pacientes
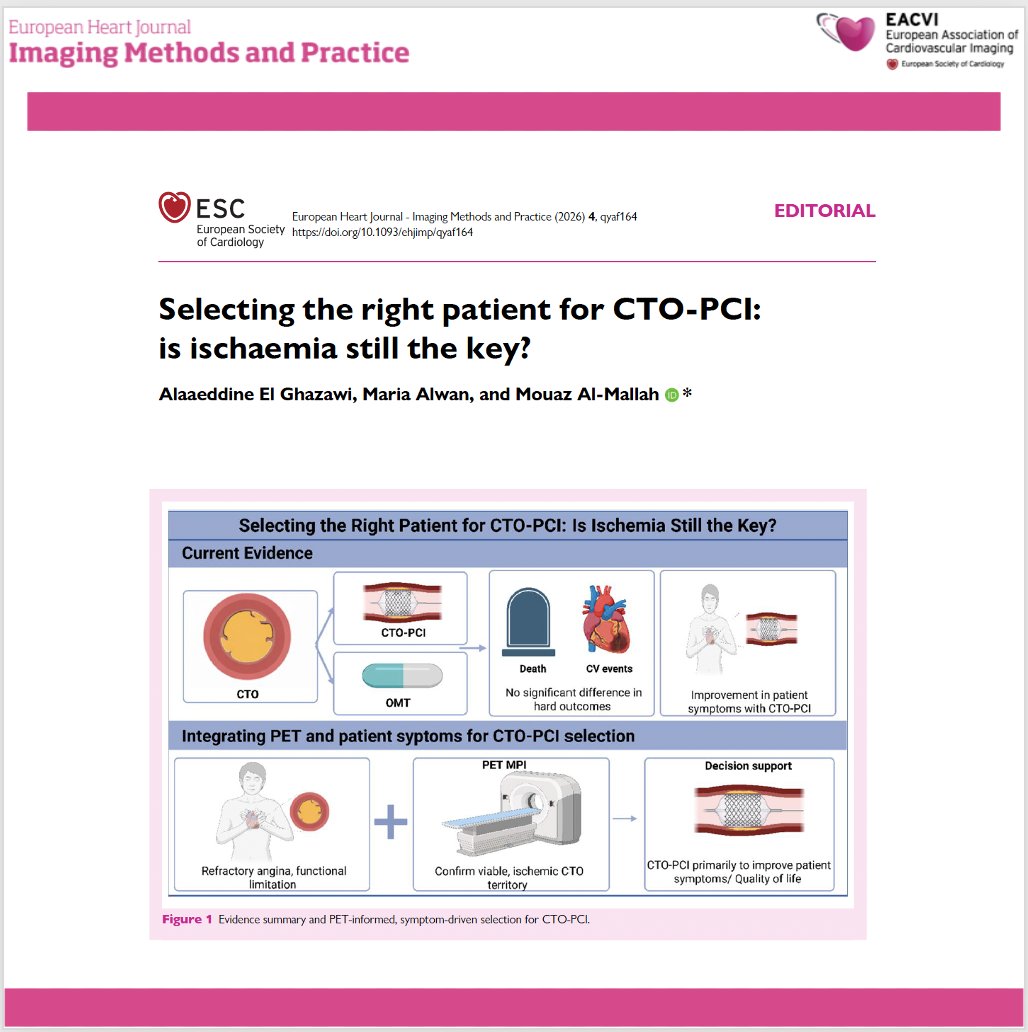
📄 CTO-PCI: is ischaemia still the key for patient selection?
🔗 DOI: https://t.co/1OtXRpQLiq
🫀 Chronic total occlusion (CTO) PCI has evolved significantly, with high success rates—but patient selection remains the real challenge.
This editorial questions a long-standing paradigm:
👉 Is ischaemia enough to guide revascularization?
✨ Key insights:
🔹 CTO-PCI is associated with:
✔ improved symptoms and quality of life
❗ but no clear reduction in mortality or major events
🔹 Randomized trials show:
➡️ similar hard outcomes vs optimal medical therapy
➡️ benefit mainly in angina relief
📊 Role of ischaemia:
👉 Imaging confirms ischaemia—but:
❗ baseline ischaemic burden does NOT predict outcomes after CTO-PCI
🔹 Even patients with ≥10% ischaemia:
➡️ no difference in mortality or MACCE
➡️ but fewer angina hospitalisations
⚠️ Why ischaemia alone is insufficient:
👉 CTO physiology is complex:
collateral circulation
multivessel disease
microvascular dysfunction
👉 SPECT may underestimate disease
👉 PET provides better quantification (MBF, MFR)
💡 Clinical paradigm shift:
👉 From “ischaemia-driven” → “symptom-driven” selection
✔ Revascularize when:
refractory angina
significant functional limitation
👉 Imaging role:
➡️ confirm viable, ischaemic myocardium
➡️ support—not dictate—the decision
🧠 Future directions:
🔹 PET-based quantification (MBF/MFR)
🔹 Territory-specific ischaemia assessment
🔹 Integration of patient-reported outcomes
🚨 Bottom line:
CTO-PCI is a tool to improve symptoms—not to change prognosis.
👉 Treat the patient, not just the ischaemia.
#Cardiology #CTO #PCI #Ischaemia #CardiacImaging #PET #CoronaryArteryDisease #InterventionalCardiology #PrecisionMedicine 🫀📊
The American Heart Association mourns the passing of the legendary cardiologist Eugene Braunwald, M.D., widely recognized as one of the most influential figures in the history of cardiovascular medicine. Over seven decades, his work reshaped the understanding and treatment of heart disease, leading many to call him the father of modern cardiology.
Braunwald was a lifelong contributor to the American Heart Association, helping advance its research and scientific mission, and was honored with some of the Association’s highest honors for his lasting influence on cardiovascular care and research. His influence extended well beyond his own discoveries, as generations of Association‑supported investigators, clinicians and academic leaders were trained by Braunwald or guided by the clinical trial standards and mentorship models he helped establish.
https://t.co/ieZuHYMyOP
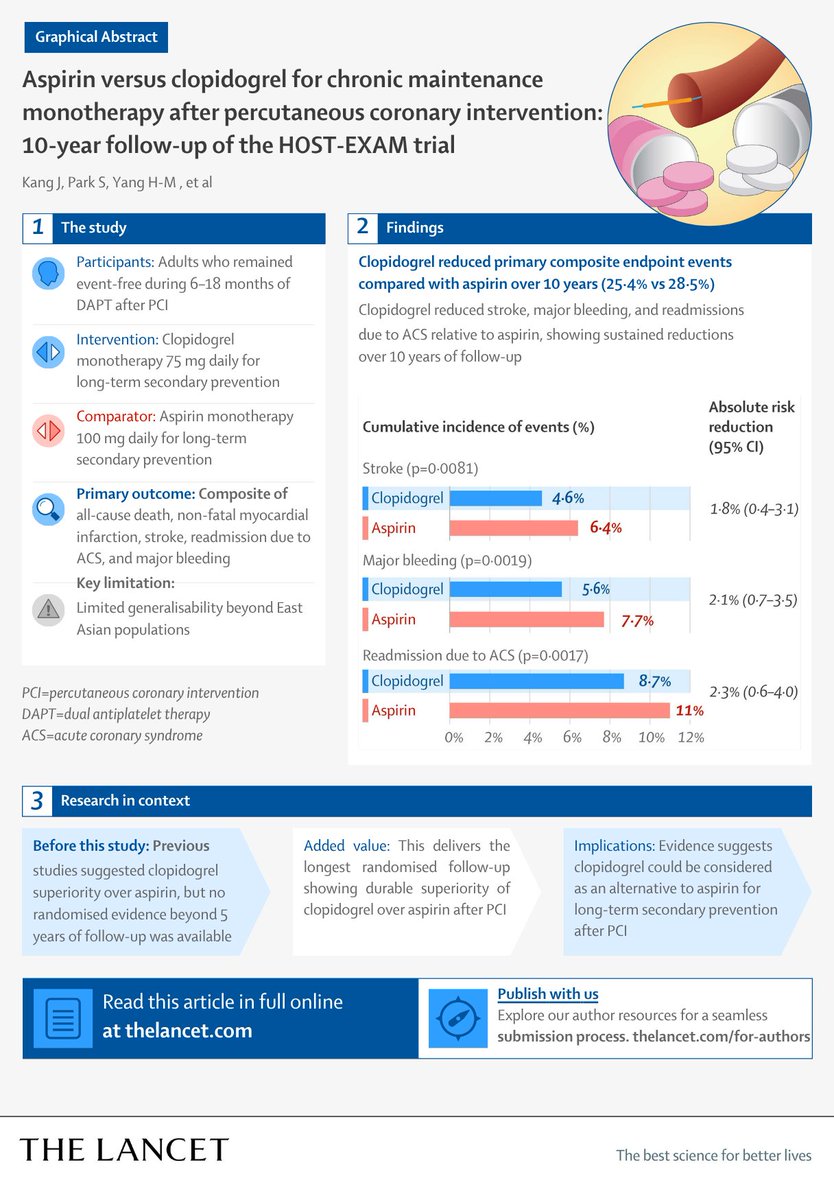
Clopidogrel vs aspirin after PCI:
10-year HOST-EXAM follow-up shows lower ischemic and bleeding events with clopidogrel—but no difference in mortality.
Read more: https://t.co/UrwslCemU8 #ACC26
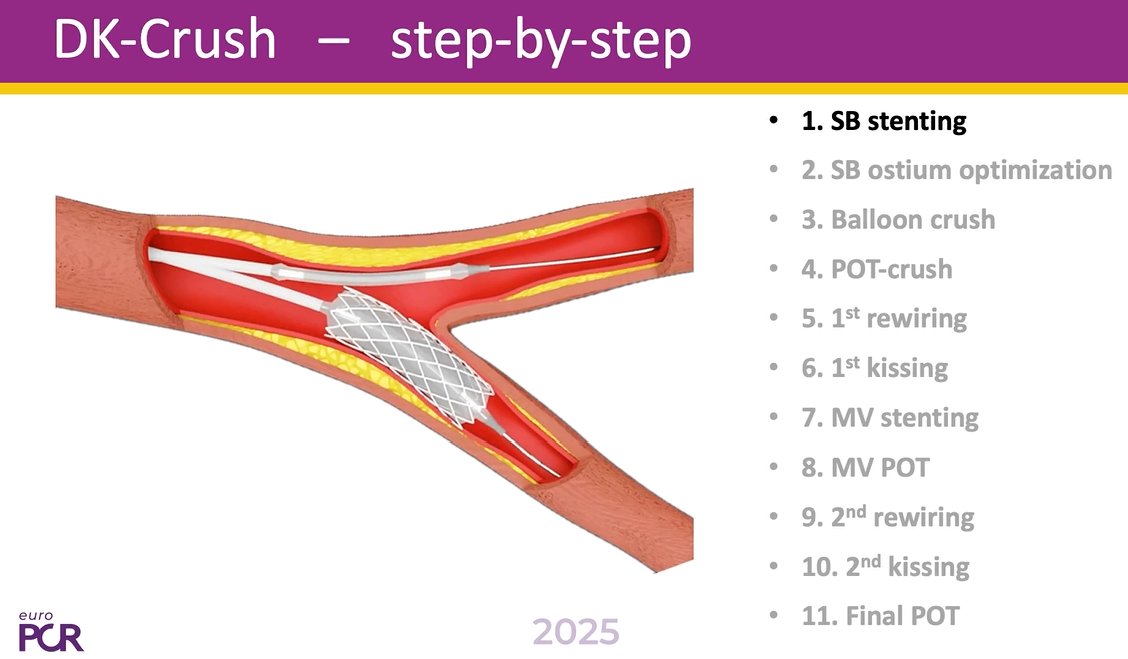
📢DK Crush like you’ve never seen it before!
Episode 1⃣ of this series on "How to perform DK-Crush for left main bifurcation stenting" now online
📺https://t.co/Y64RCYU1w3
In this episode, learn about:
🟣Multi-modality simulation to unveil the hidden parts & small obstacles that can result in complications
🟣Angioscopy directly inside the coronary artery to provide a better understanding of 3D stent configuration
In-depth commentary and perspective and perspective provided by @GoranEBC & William Wijns.
@twj1974@NievesGonzalo1@BURZOTTA_F@M_Lesiak@gabor_gt@RhianEDavies1@esbrilakis@VisibleHeartLab
#interventionalcardiology #CardioEd #EuroPCR
Among patients with anterior myocardial infarction, adding low-dose rivaroxaban to dual antiplatelet therapy did not significantly reduce left ventricular thrombus formation at 1 month but increased minor bleeding.
https://t.co/TDDR0p8sWV
How to perform DK-Crush for left main bifurcation stenting
A new 3-part series is coming: a step-by-step approach to one of the most complex procedures in interventional cardiology, with additional in-depth commentary and perspective shared by @GoranEBC and William Wijns.
Breaking down the 11 key steps to success, from real-world practice to emerging technology:
🟣A LIVE educational case from Poznań, Poland
🟣Angiography and intravascular imaging
🟣Machine learning, AI and 3D simulation
Watch this space!
@twj1974@NievesGonzalo1@BURZOTTA_F@M_Lesiak@gabor_gt@VisibleHeartLab
#interventionalcardiology #CardioEd #EuroPCR
@sbrugaletta
🫀The failing right ventricle:
the most misunderstood chamber in critical care
For years, we focused on the left ventricle.
But in the ICU, the real killer is often the right ventricle.
->What is acute RV failure?
👉 Not just “weak contraction”
It’s a hemodynamic collapse syndrome:
RV dilation
↓ LV preload
↓ cardiac output
↑ venous congestion
➡️ → multi-organ failure
->The key pathophysiology (the vicious cycle)
1. ↑ Afterload (PE, ARDS, PH)
2. → RV dilation
3. → Septal shift → LV underfilling
4. → ↓ CO → hypotension
5. → ↓ RCA perfusion
6. → RV ischemia
👉 And the cycle accelerates
->The most important concept
👉 The RV does NOT tolerate pressure
Handles preload very well
Fails rapidly with afterload
➡️ Even small ↑ PVR → collapse
->Main causes you MUST think first
🔴 Pulmonary embolism
🔴 RV myocardial infarction
🔴 ARDS / mechanical ventilation
🔴 Decompensated pulmonary hypertension
🔴 Post-cardiac surgery
->Diagnosis is NOT obvious
There is no single sign.
👉 It requires suspicion + integration:
Clinical: congestion + hypoperfusion
ECG + biomarkers
POCUS (your best friend 🤓)
Hemodynamics
->Echo mindset (fast ICU approach)
👉 Don’t overcomplicate
Look for:
✔ RV dilation
✔ Septal shift (D-sign)
✔ TAPSE ↓
✔ Venous congestion
The real ICU mistake
❌ Treating RV failure like LV failure
->Management principles
👉 Think in 4 pillars:
1. Preload — “not too much, not too little”
Hypovolemic → small fluid
Congested → REMOVE fluid
👉 CVP is not a target, it’s a warning
2. Afterload, THE key target
✔ Treat PE
✔ Optimize ventilation
✔ Reduce PVR
👉 If afterload stays high → RV will fail
3. Contractility
Dobutamine
Milrinone
Levosimendan
👉 Choose based on context
4. Perfusion pressure
👉 Norepinephrine is your anchor
✔ Maintains coronary perfusion
✔ Supports RV function
->Ventilation: the silent killer
⚠️ Positive pressure = ↑ PVR
👉 Over-ventilate → worsen RV failure
->When nothing works
👉 Think early:
VA-ECMO
RV assist devices
🤓Key insight
This is NOT just a cardiac problem.
👉 It is a ventriculo–arterial coupling failure
When:
Ees / Ea ↓ → RV collapses
🤓Bottom line
✔ RV failure is preload dependent BUT afterload sensitive
✔ Small mistakes → rapid collapse
✔ Early recognition + physiology-based treatment saves lives
->Clinical mindset
👉 Don’t ask:
“Is the RV failing?”
👉 Ask:
“Why is the RV failing and, what is driving the afterload?”
📃Reference
Giannakoulas G. et al. European Heart Journal (2025) 00, 1–16 https://t.co/gri8ZaHHsI
🫀💊 ¿Suspender los beta-bloqueadores después de un infarto? 🧐
SMART-DECISION encontró que suspender los BB al año NO fue inferior a continuarlos en cuanto a:
✔️ Muerte por cualquier causa
✔️ Infarto recurrente
✔️ Hospitalización por insuficiencia cardíaca
#ACC26#Cardiology
SMART-DECISION: Discontinuing beta-blocker therapy was found to be noninferior to continuing the therapy among stable, low-risk patients who took it for at least one year following a #cvMI.
Get the latest insights from the #ACC26 LBCT: https://t.co/Q4BGcET3E3
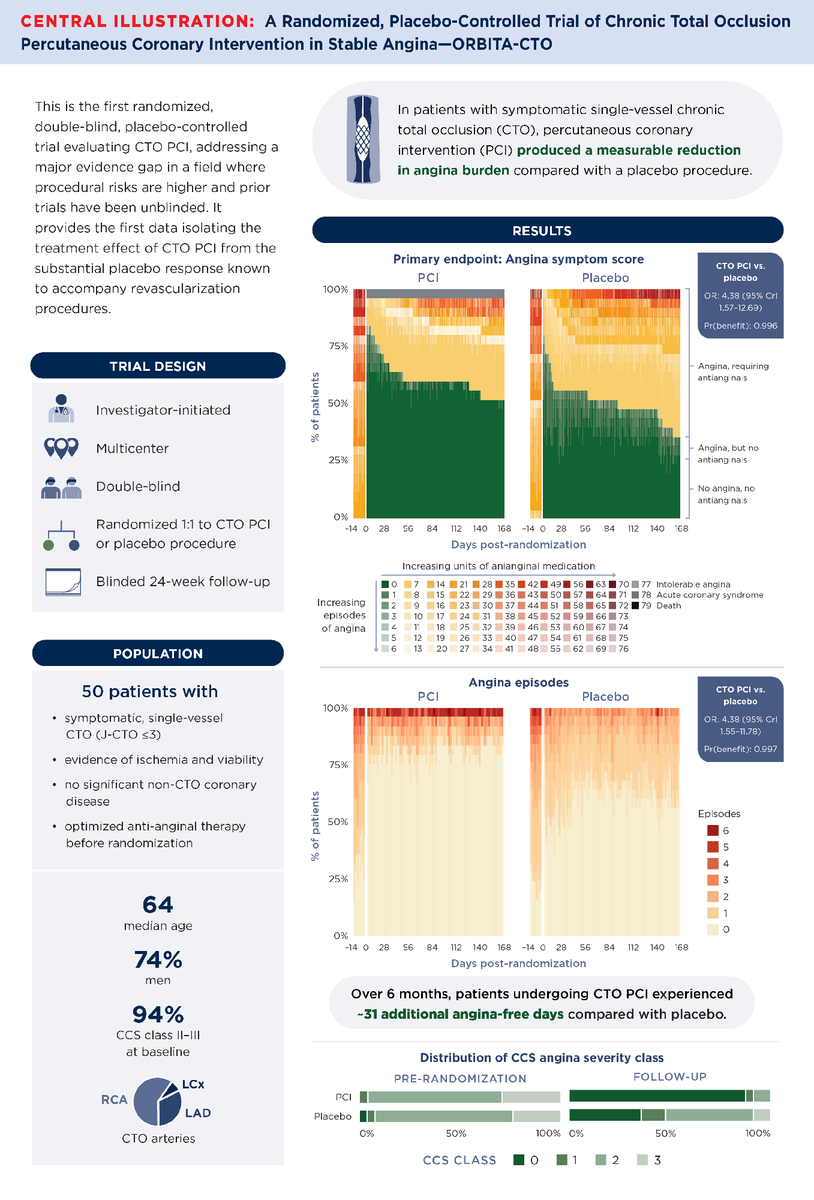
In patients with symptomatic single-vessel chronic total occlusion, percutaneous coronary intervention for coronary chronic total occlusion (CTO PCI) improves angina beyond placebo.
Get the details in #JACC: https://t.co/yX0FDuSOjl #ACC26#PCI#CTO@dr_skhan1
Presented at #ACC26:
Among patients with intermediate coronary lesions, angiography-guided revascularization was noninferior to pressure-wire–based guidance with respect to death, myocardial infarction, or revascularization. FAST III trial results: https://t.co/lKLehrrpm1
Editorial: Redefining Physiology in the Cardiac Catheterization Laboratory https://t.co/tSiweN2Yjo
@ACCinTouch
Clopidogrel vs aspirin after PCI:
10-year HOST-EXAM follow-up shows lower ischemic and bleeding events with clopidogrel—but no difference in mortality.
Read more: https://t.co/lJxVcoJxzW #ACC26
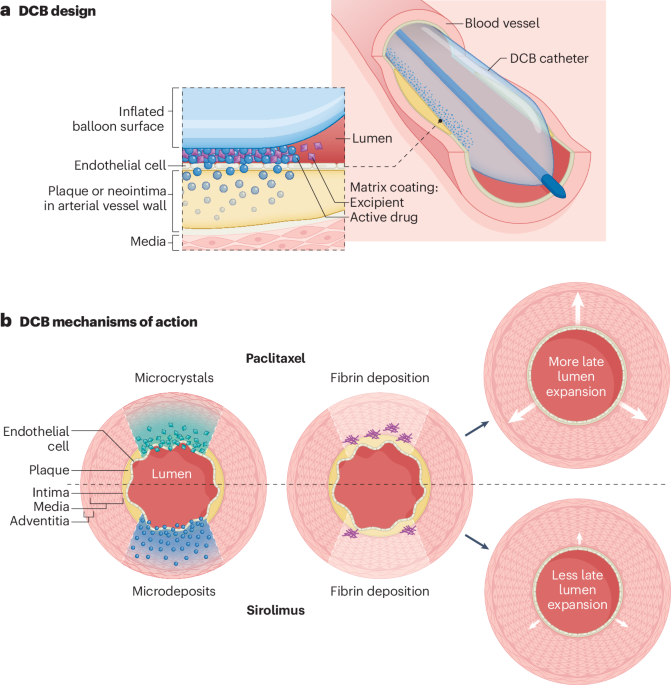
New online! Drug-coated balloon angioplasty for coronary and peripheral artery disease: latest evidence and clinical indications https://t.co/4TyqGr7viw