🗣️☢️Intriguing abstract #ESMO25 - possible increased systemic response after hypofractionated RT (36Gy/12fx) with pembro for R/M-HNSCC?
Looking forward to more details!
Great work by @MayoRadOnc emphasizing our specialty’s need to engage with the cultural perception of radiation.
Congrats to Drs. Elsa Sutton, Scott Lester, and the study team for this unique perspective. #ASTRO2025
An intriguing poster at #ASTRO25 demonstrates that major North American TV Shows are leading viewers to believe radiation might cause "internal melting, burning, or crumbling, or even a food allergy". @ASTRO_org@PRJeffWhite@NehaVapiwala@sueyom https://t.co/r6yOOgQrJ0
Congrats to @DavidRoutmanMD@KatieVanAbelMD@LindaXYinMD and our stellar MS4 Cecelia Hidalgo for presenting our real world data with DART (30-36 Gy) for HPVOPC.
282 patients and 97% PFS for int risk group. DART is a standard tx for int risk pts @MayoCancerCare#ASTRO25
Thank you @DavidSherMD and the other commentators for their insightful thoughts concerning MC1675 (DART).
It's a pleasure and privilege to respond back to their astute observations, which I'll include below.
It was such a pleasure to read the results of this juicy and terrific randomized trial of postop RT dose de-escalation for HPV+ OPSCC from @DanielMaMD and colleagues at @MayoRadOnc.
The field has been waiting for the formal results, and this paper does not disappoint.
https://t.co/fV9yfPXxDG
@DavidSherMD@DavidRoutmanMD 5. Finally, more research in biological selection is needed. Whether it's functional imaging ala @imrtlee, ctDNA ala @DavidRoutmanMD, AI-assisted involved node selection ala @DavidSherMD, or chromosome instability ala @pipcosper (and many more strategies!), we need better data.
@DavidSherMD Absolute numbers for recurrence were small, so perhaps we were unlucky. But it's challenging for me to reconcile a difference in primarily distant control based upon differences in locoregional RT dose.
I would stress our thoughts on cis vs doce are hypothesis generating.
@DavidSherMD We were very happy to report a statistically sig difference in grade 3 toxicity, and like David points out, a large difference in grade 2 toxicity. This is reflected in the SS difference in patient QOL even at 2 years. Grade 2s really do matter.
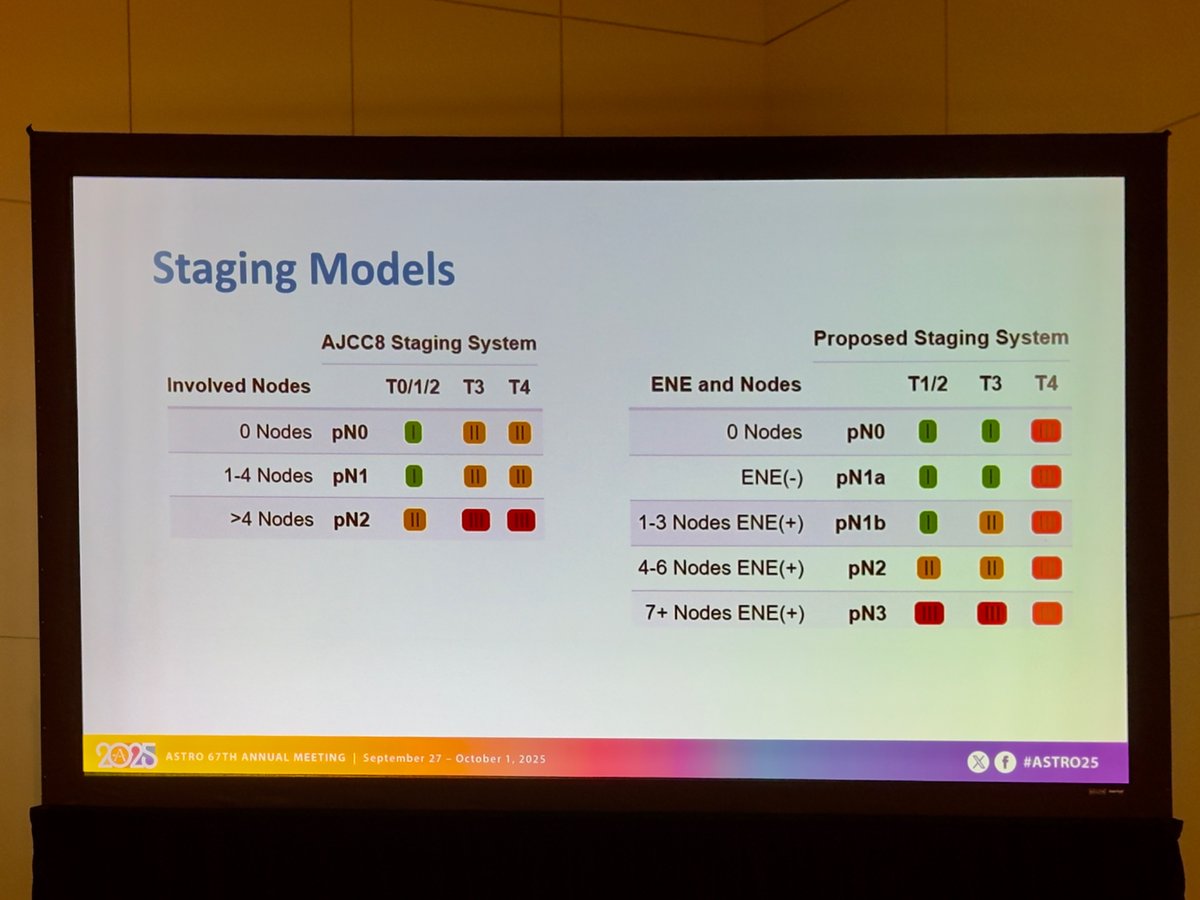
@DavidSherMD Concerning the int risk (ENE-) cohort, the AJCC 7 table regrettably requires a correction.
The majority of of int risk pts were AJCC N2b. AJCC staging changed mid study which introduced some confusion in the CRFs. This was caught post-pub and a correction is actively pending.