"Ultimately, the secret of quality is love. You have to love your patient, you to have to love your profession, you have to love your G-d." Avedis Donabedian
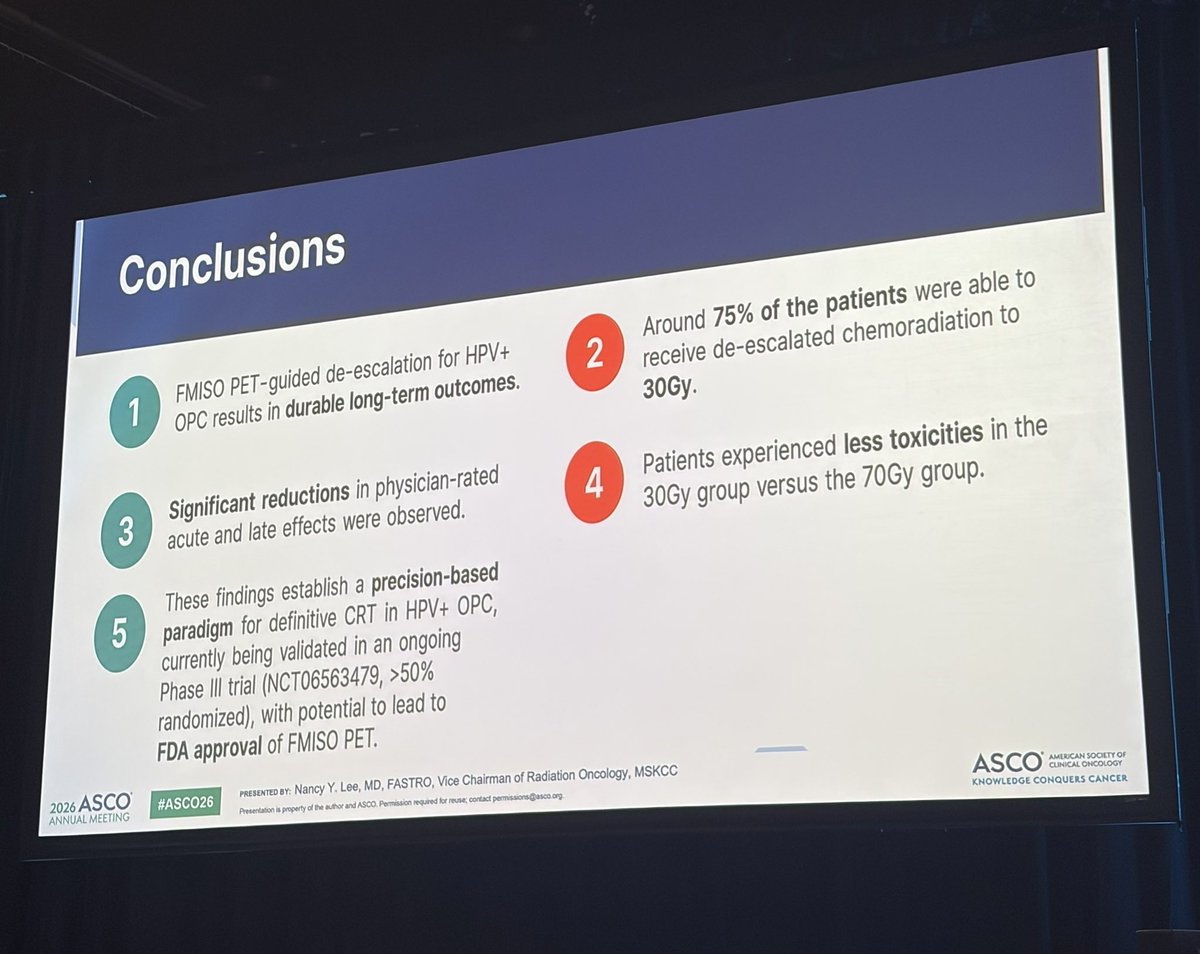
75% of patients received 30 Gy with FMISO PET based de-escalation for HPV-associated OPSCC. 30 Gy.
Need the randomized data but hard to believe this won’t be the way.
Incredible!
Today at #ASCO26: MSK radiation oncologist Dr. Nancy Lee (@imrtlee) shared long-term results showing that many patients with HPV-positive #oropharyngeal cancer were able to receive lower-dose radiation while maintaining durable outcomes and experiencing fewer side effects.
Such a critical point that applies to all disease sites comparing one radiotherapy modality with another.
Modern IMRT/VMAT is really, really good, not just because of the quality of the delivery but because we have a better understanding of key OARs and how to avoid them.
The challenge in improving on current outcomes is defining both the relevant dose metrics (beyond the "standard" for each disease site) and the relevant quality-of-life/bother endpoints that matter for patients in the long-run. I don't think that our current measures capture the entirety of the post-treatment patient experience, which is very difficult to quantify.
Agree - superb thread.
I would recommend one additional square: pay attention to the absolute benefit.
The HR is the standard metric for powering and evaluating clinical trials, but it also can hide a small absolute benefit that must be weighed against an often substantial absolute increase in adverse events for the arm with superior efficacy.
@PaulJiL@ASCO Very interesting preliminary result. KN-412 was actually pretty close but likely needed a few tweaks… What was the biomarker selection? Could the adjuvant pembro have made the difference given the CPS-positive population? Looking forward to the results!
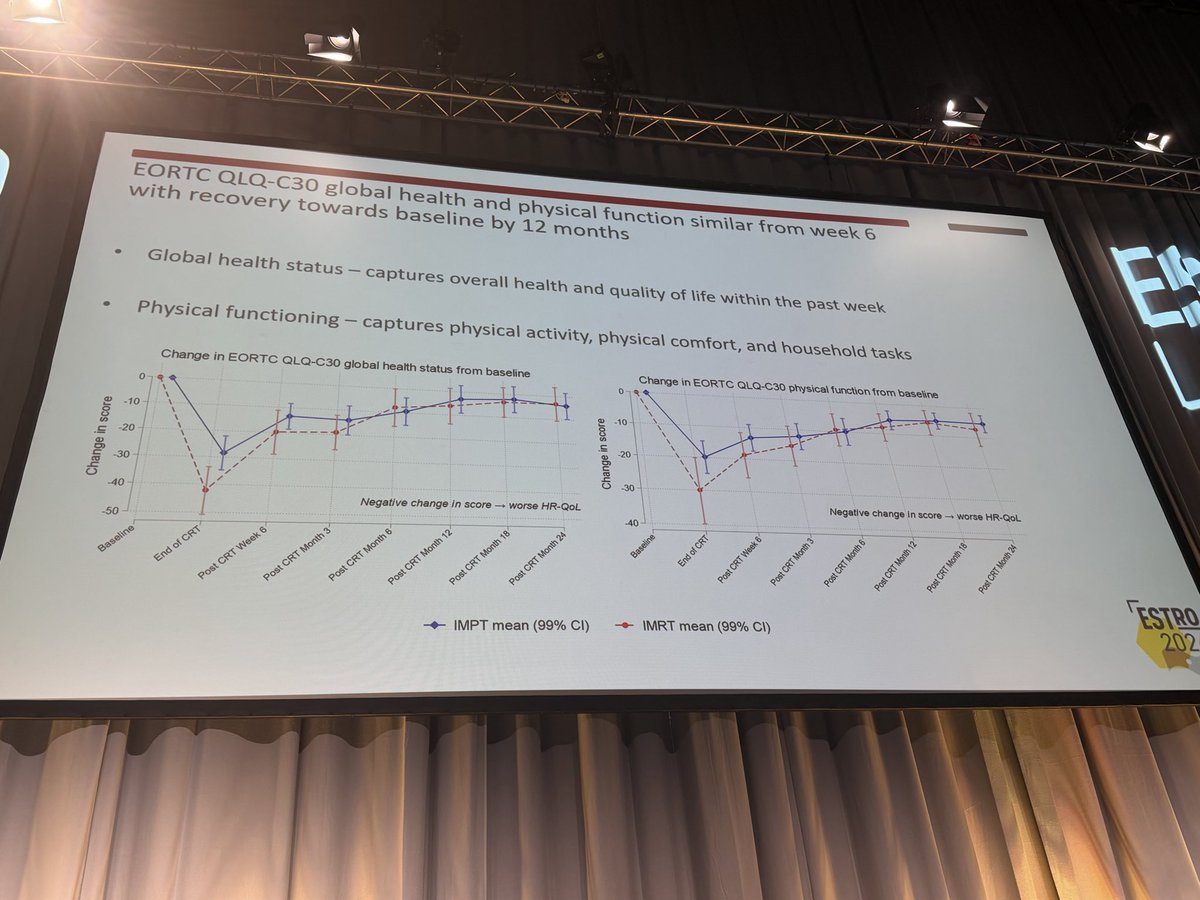
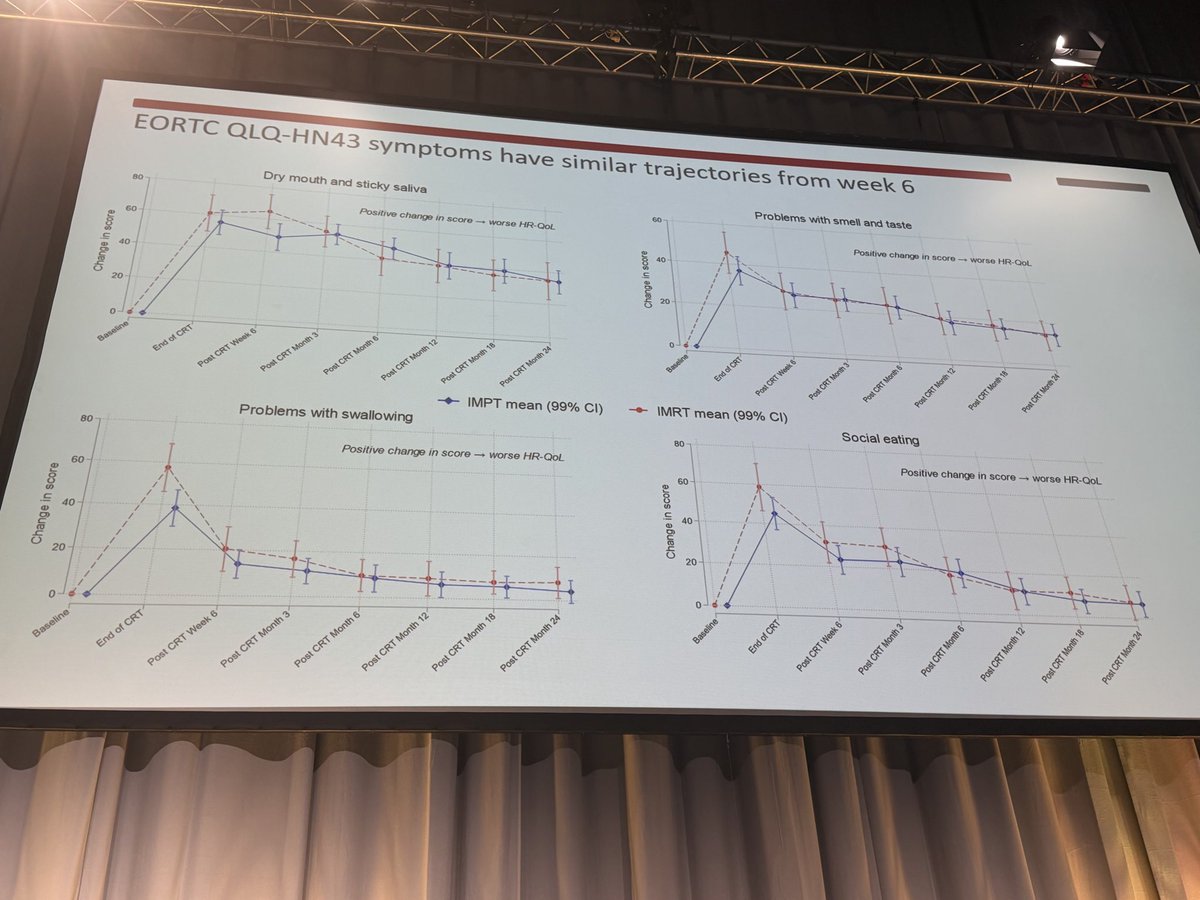
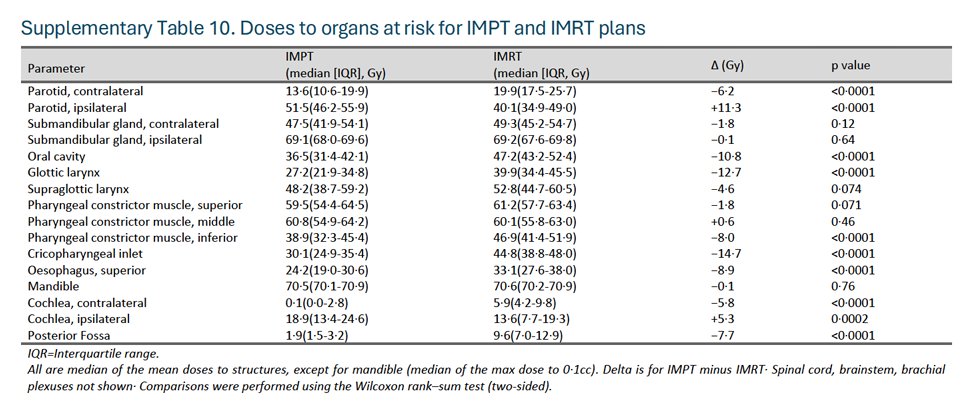
It was clear that the IMPT plans were better than IMRT. I think they could have been substantially better, but regardless, the improved dosimetry did not translate into long-term PRO gains. At all.
A critical question is understanding the determinants of PRO results in HNSCC patients. How much does expectation, mood, equilibrating to the new normal, genetics all play into these outcomes?
No QoL difference with IMPT vs IMRT in oropharyngeal cancer in the TORPEdO 🇬🇧 trial.
How to explain the differences w/ @SJFrankMD 🇺🇸 trial? Planning? Patients? Crossover in the 🇺🇸 trial? Real absence of difference?
Cc @EmmaHall71 @
It is an exciting paradigm, and our current phase II RCT (INVERT) is approximately 75% accrued. We are extremely grateful to the patients and families who have enrolled in these studies!
We are working on both an AI-free approach as well as automation of the entire workflow (i.e. auto-segmentation of the nodes and malignancy classification).
More to come over the next year on these endeavors.
We hope to finish accrual on INVERT over the next several months and, if successful, move this regimen to a multi-institutional randomized trial.
Absolutely terrific work by @DrSymYoung to report the long-term outcomes of our INRT experience from two prospective trials (INRT-AIR and DARTBOARD).
Short version: with long-term follow-up (median 5.2 years for INRT-AIR, 3 years for DARTBOARD), we've seen zero solitary elective nodal recurrences.
Longer version: ESTRO has highlighted novel approaches to managing the elective neck in HNSCC, and I believe the future will be very different than the present. Current ENI fields deliver the majority of the integral dose to patients and contribute substantially to critical structures (swallowing and xerostomia OARs). Minimizing ENI dose and volume may meaningfully improve the short- and especially long-term tolerance of radiotherapy.
A few more thoughts on our INRT paradigm below:
While ENI dose de-escalation is clearly better 50-56 Gy, it is not a substitute for INRT.
In INRT-AIR, we contoured standard ENI volumes to assess the delivered dose.
The median V40 to the ENI PTV was 50%, and the median V30 was 58%.
Absolutely incredible work by @_ShankarSiva and colleagues! Wow.
My question is how to engage our surgical and medical oncology trialist colleagues to test this paradigm versus primary surgery. @Raquib_Hannan
Is this going to end up like bladder cancer?
#ESTRO26 - 📣 FASTRACKII final results, median F/U of 5 years. Thank you patients, funders, investigators - #kidneycancer#kcsm
1) 100% Local Control: No local recurrences were observed at 36, 60, or 84 months.
2) 100% Cancer-Specific Survival
3) Grade 3 AEs remain at 10%
Great concept to actually nail down what's happening in these fractions.
So in the MRL-guided patients, it's just alignment and motion-management, so PTV margins are the same with and without daily adaptation? Dose/fraction?
Are you stratifying by MR/CT and by QD versus QOD?
Are patients blinded?
Phenomenal idea. Need more of these kinds of studies to resolve how the (expensive and time-intensive) technology is really helping!
There are tremendous opportunities to improve post-operative radiotherapy in HNSCC. The DIREKHT trial is an excellent example of such work, in which they spared the contralateral neck in a specified group of patients and/or reduced the primary CTV dose to 56 Gy.
The details are important, as over 60% of patients had contralateral (path-negative) neck dissections (from prior publication). Putting aside the controversy of sparing an un-dissected contralateral neck for an oropharynx (non-tonsil) or oral cavity cancer, there is still hesitance to spare a path-negative contralateral neck.
This paper helps assuage those fears. In the original publication, there were 3 contralateral-only LN recurrences, all in un-dissected necks. That means there were zero solitary nodal recurrences in 92 patients with a path-negative contralateral neck dissection, now with long-term follow-up.
If a contralateral neck has been adequately dissected and is negative, it's hard to justify additional treatment to that hemi-neck.
It's difficult to judge the 56 Gy outcomes by abstract alone, especially since the cohort mixed HPV-positive OPC and oral cavity.
Extremely informative trial!
Two of our faculty, Drs. @MonaArbabMD and Aurelie Garant, along with one of our fellows, Dr. @DrSymYoung, having a great time this weekend at #ESTRO26!
JCOG 1208 is a nice study of ENI dose (46 Gy/23 fx) and volume reduction, without any solitary elective neck failures; another trial that supports ENI de-intensification.
However, we cannot be satisfied with 79% locoregional PFS, especially for oropharyngeal cancer.
Even with T1-2 N0-1 disease, sometimes concurrent chemotherapy may be needed.













![OncoAlert's tweet photo. Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
De-intensification of postoperative radiotherapy in HNSCC by omitting contralateral elective neck irradiation– long term outcomes of the DIREKHT trial Presented by Charlotte Frei 🇩🇪
#RadOnc ☢️
The DIREKHT trial is a prospective multicentre phase II trial investigating de-intensified risk-adapted radiation in patients with newly diagnosed, non-metastatic HNSCC after surgery. A total of 140 patients were included in the analysis. After five years, overall locoregional recurrence rate was 6.0% (95% CI [1.9; 9.9]). Cumulative incidence of locoregional recurrence was 3.0% (95%-CI [0.1; 5.8]). Details on recurrence patterns and dysphagia rates are presented at ESTRO 2026.
@ESTRO_RT
@yasemin09896924
@LindaMrissa
@christian_roenn
@Valeriadionisi
@gerryhanna
@clchiang_hk
@mtugceyilmaz
@B_Tomasik
@gmpetrianni
@CiroFranzese1
@Atem84
@piet_ost
@brachyexpert
@BlanceS90
@The_PT_Explorer
@BarbaraJereczek
@Mat_Guc
@ZilliThomas
@AnnaKirby17
@PBlanchardMD
@achoud72
Pinging OA faculty
@MKnoll_MD
@_ShankarSiva
@Icro_Meattini
@seanmmcbride
@NiuSanford
@nataliagandur
@acampsmalea
@to_be_elizabeth](https://pbs.twimg.com/media/HIbrg-HWUAAvxYR.jpg)
![OncoAlert's tweet photo. Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
De-intensification of postoperative radiotherapy in HNSCC by omitting contralateral elective neck irradiation– long term outcomes of the DIREKHT trial Presented by Charlotte Frei 🇩🇪
#RadOnc ☢️
The DIREKHT trial is a prospective multicentre phase II trial investigating de-intensified risk-adapted radiation in patients with newly diagnosed, non-metastatic HNSCC after surgery. A total of 140 patients were included in the analysis. After five years, overall locoregional recurrence rate was 6.0% (95% CI [1.9; 9.9]). Cumulative incidence of locoregional recurrence was 3.0% (95%-CI [0.1; 5.8]). Details on recurrence patterns and dysphagia rates are presented at ESTRO 2026.
@ESTRO_RT
@yasemin09896924
@LindaMrissa
@christian_roenn
@Valeriadionisi
@gerryhanna
@clchiang_hk
@mtugceyilmaz
@B_Tomasik
@gmpetrianni
@CiroFranzese1
@Atem84
@piet_ost
@brachyexpert
@BlanceS90
@The_PT_Explorer
@BarbaraJereczek
@Mat_Guc
@ZilliThomas
@AnnaKirby17
@PBlanchardMD
@achoud72
Pinging OA faculty
@MKnoll_MD
@_ShankarSiva
@Icro_Meattini
@seanmmcbride
@NiuSanford
@nataliagandur
@acampsmalea
@to_be_elizabeth](https://pbs.twimg.com/media/HIbrg9GW4AEY1X2.jpg)
![OncoAlert's tweet photo. Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
De-intensification of postoperative radiotherapy in HNSCC by omitting contralateral elective neck irradiation– long term outcomes of the DIREKHT trial Presented by Charlotte Frei 🇩🇪
#RadOnc ☢️
The DIREKHT trial is a prospective multicentre phase II trial investigating de-intensified risk-adapted radiation in patients with newly diagnosed, non-metastatic HNSCC after surgery. A total of 140 patients were included in the analysis. After five years, overall locoregional recurrence rate was 6.0% (95% CI [1.9; 9.9]). Cumulative incidence of locoregional recurrence was 3.0% (95%-CI [0.1; 5.8]). Details on recurrence patterns and dysphagia rates are presented at ESTRO 2026.
@ESTRO_RT
@yasemin09896924
@LindaMrissa
@christian_roenn
@Valeriadionisi
@gerryhanna
@clchiang_hk
@mtugceyilmaz
@B_Tomasik
@gmpetrianni
@CiroFranzese1
@Atem84
@piet_ost
@brachyexpert
@BlanceS90
@The_PT_Explorer
@BarbaraJereczek
@Mat_Guc
@ZilliThomas
@AnnaKirby17
@PBlanchardMD
@achoud72
Pinging OA faculty
@MKnoll_MD
@_ShankarSiva
@Icro_Meattini
@seanmmcbride
@NiuSanford
@nataliagandur
@acampsmalea
@to_be_elizabeth](https://pbs.twimg.com/media/HIbrg71XcAAxgrj.jpg)
























![OncoAlert's tweet photo. Day TWO of #ESTRO26 Coverage by OncoAlert 🚨
De-intensification of postoperative radiotherapy in HNSCC by omitting contralateral elective neck irradiation– long term outcomes of the DIREKHT trial Presented by Charlotte Frei 🇩🇪
#RadOnc ☢️
The DIREKHT trial is a prospective multicentre phase II trial investigating de-intensified risk-adapted radiation in patients with newly diagnosed, non-metastatic HNSCC after surgery. A total of 140 patients were included in the analysis. After five years, overall locoregional recurrence rate was 6.0% (95% CI [1.9; 9.9]). Cumulative incidence of locoregional recurrence was 3.0% (95%-CI [0.1; 5.8]). Details on recurrence patterns and dysphagia rates are presented at ESTRO 2026.
@ESTRO_RT
@yasemin09896924
@LindaMrissa
@christian_roenn
@Valeriadionisi
@gerryhanna
@clchiang_hk
@mtugceyilmaz
@B_Tomasik
@gmpetrianni
@CiroFranzese1
@Atem84
@piet_ost
@brachyexpert
@BlanceS90
@The_PT_Explorer
@BarbaraJereczek
@Mat_Guc
@ZilliThomas
@AnnaKirby17
@PBlanchardMD
@achoud72
Pinging OA faculty
@MKnoll_MD
@_ShankarSiva
@Icro_Meattini
@seanmmcbride
@NiuSanford
@nataliagandur
@acampsmalea
@to_be_elizabeth](https://pbs.twimg.com/media/HIbrg-lWkAAK1bp.jpg)






















