🥳🎆 Kicking of 2026 with our work showing intra-tumoral bacteria 🦠 affect outcomes of Radiotherapy + anti-PD-L1 now out in @NatureCancer with sister paper by @nataliesilvermd! Even when trials "fail" – we can learn from them! https://t.co/0iE2v2sOKZ. -- w/ @GeneCollector, @imrtlee, @TylerAlban1, @DrHaddadRobert, the Pfizer team and more! (1/N)
🧬 Can tumor genomics be used to personalize radiation dose?
Grateful to present results from our phase II trial on dose de-escalated radiation therapy for ATM altered tumors at #ASCO2026
Great to see ☢️ #Radiation in the early-phase #PrecisionOncology space!
75% of patients received 30 Gy with FMISO PET based de-escalation for HPV-associated OPSCC. 30 Gy.
Need the randomized data but hard to believe this won’t be the way.
Incredible!
Thrilled to share our new paper out today in @NatureCancer:
Tumor irradiation promotes antigen dressing of dendritic cells to enhance CAR T cell persistence and efficacy in lung metastases.
A single dose of radiotherapy makes CAR T cells work against extensive metastatic lung cancer — even when the target antigen is also on normal tissues.
https://t.co/4xHTzjNOc8
🧵 (1/14)
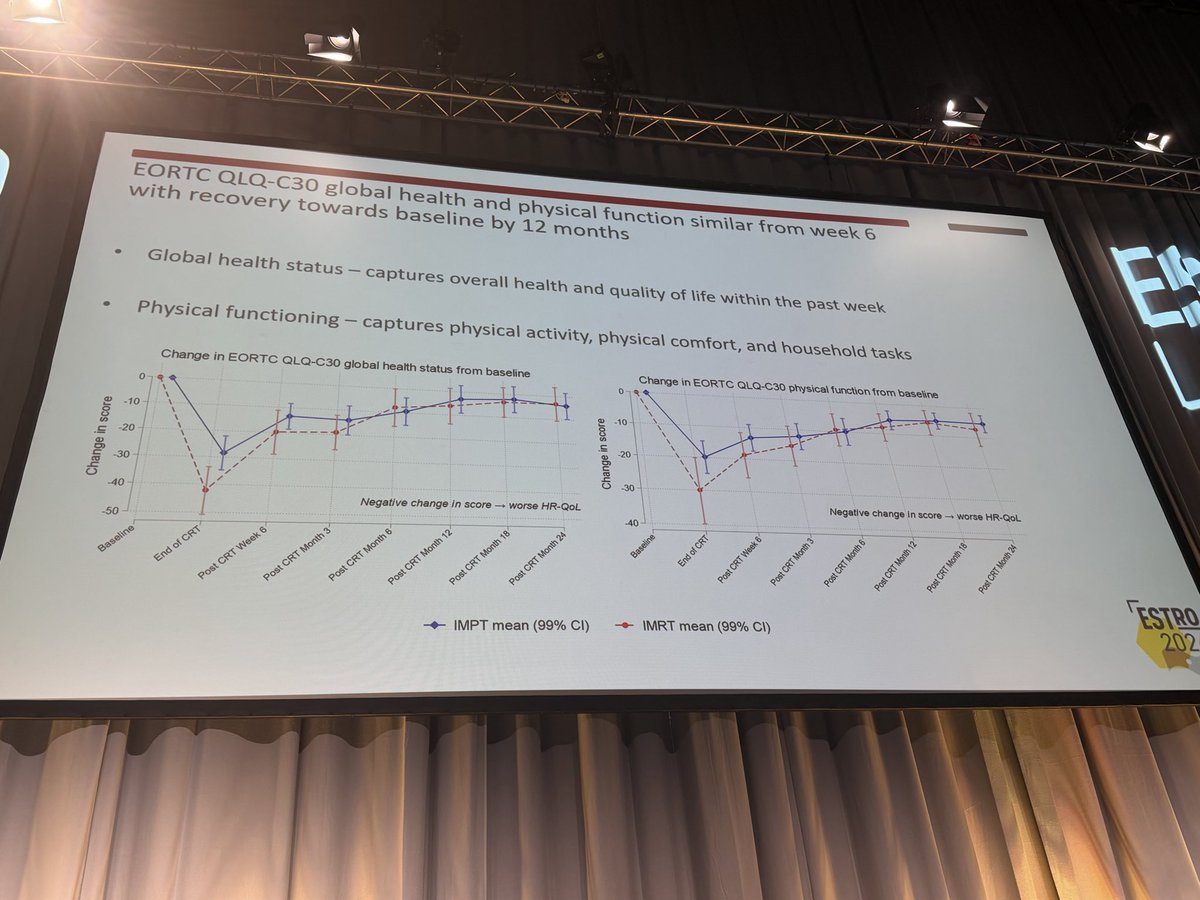
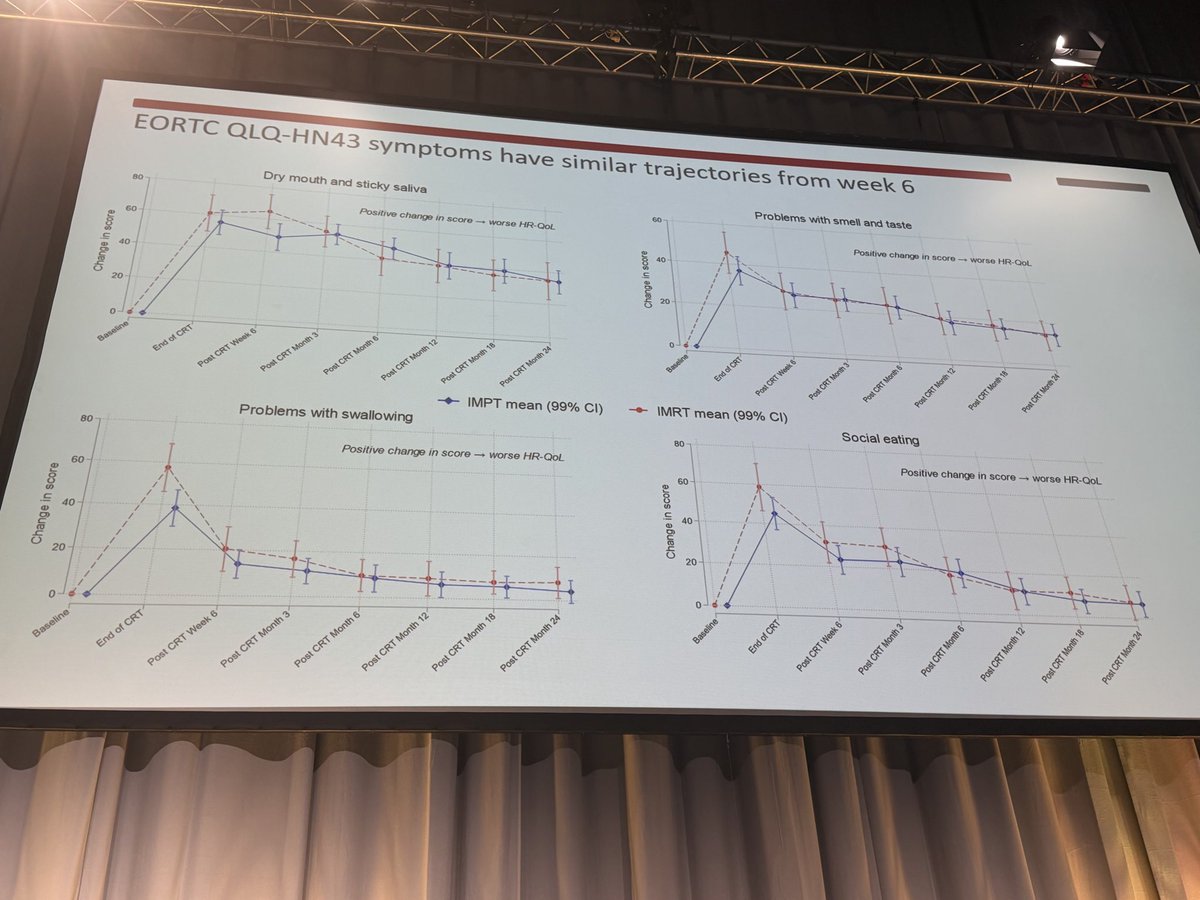
No QoL difference with IMPT vs IMRT in oropharyngeal cancer in the TORPEdO 🇬🇧 trial.
How to explain the differences w/ @SJFrankMD 🇺🇸 trial? Planning? Patients? Crossover in the 🇺🇸 trial? Real absence of difference?
Cc @EmmaHall71 @
Absolutely terrific work by @DrSymYoung to report the long-term outcomes of our INRT experience from two prospective trials (INRT-AIR and DARTBOARD).
Short version: with long-term follow-up (median 5.2 years for INRT-AIR, 3 years for DARTBOARD), we've seen zero solitary elective nodal recurrences.
Longer version: ESTRO has highlighted novel approaches to managing the elective neck in HNSCC, and I believe the future will be very different than the present. Current ENI fields deliver the majority of the integral dose to patients and contribute substantially to critical structures (swallowing and xerostomia OARs). Minimizing ENI dose and volume may meaningfully improve the short- and especially long-term tolerance of radiotherapy.
A few more thoughts on our INRT paradigm below:
This is the crux of it. They do have acute toxicity benefits in OPC, but is that enough? Protons have a place in reirradiation, skull base, and very young H&N patients. They have unique dosimetry beyond the Bragg peak, LET peculiarities at the distal edge we've barely begun to exploit. It's incumbent on young investigators to push forward and think creatively about how those dosimetric advantages can actually benefit patients. Our initial attempts, as you've described, have largely been disappointing and the worst thing for the field is to assume the @SJFrankMD OS data is going to hold up, when it's highly likely the long-term UK data ends up contradicting it, as may the other European trials starting up. We need new strategies, not doubling down on paths that look like dead ends.
Great letter by @SeanMcbride laying out real concerns with the OS claim in @SJFrankMD's proton vs. photon oropharynx trial. Compelling enough that Yingzhi Wu and @EChrisDee pulled our own data. We see no OS difference between protons and photons. Together with UK TORPEdO RCT, this adds to the concern that the randomized trial’s OS finding may be hypothesis-generating rather than causal.
Our letter to the editor in The Lancet critiquing the MD Anderson-led trial of protons v photons for OPC. Appreciate @SJFrankMD's well thought out response.
I think we can all agree on two points:
1) Steve deserves major kudos for bringing level 1 evidence to the debate on protons v photons for OPC. These trials are extraordinarily difficult to run, and Steve, et al pulled it off. Well done!
2) Longer term follow-up from TORPEdO will help tease out the extent to which protons improves OS in OPC.
@CJTsaiMDPhD@drlorenmell@xrtGenomics@DavidSherMD #radonc #hncsm
https://t.co/STvm2x8ape
Stay tuned! Informally we see some differences in acute toxicity (mainly dysgusia) that attenuate over time. The controversey isn't on this though (UK & MDA data are consistent here) -- its on the OS data without a PFS benefit, with a lot of obivous statistical confounding issues.
Of course @SJFrankMD and the trial invesitgators should be commended for putting together this seminal study -- much of the other data will be very important for the field. I just wish the discussion around the OS effect had been more realistic. We are preparing the unpublished data above for publication with full details (stay tuned).
Really exciting work by @HeadNeckMD and @jdschoenfeld1 -- The way to de-escalate HPV-related cancers, even advanced tumors is monitoring treatment response and selecting those that respond! Nice proof of concept this can be done with ctDNA --- Looking forward to seeing this space develop @CJTsaiMDPhD@imrtlee@sueyom@seanmmcbride@BillDiplas
Sharing the results of ReACT 1.0 in @NatureComms -- the first study to use HPV ctDNA to guide CRT de-escalation in higher risk HPV+ OPC. ctDNA metrics may improve risk stratification. Grateful to our coauthors. @Naveris_inc@DanaFarberNews@jdschoenfeld1
https://t.co/53tHQtj8pl
The future is here!!!
First ever plasma liquid biopsy capable of profiling the tumor microenvironment with spatial transcriptomic insight.
Out today in @Nature!
Very thoughtful editorial on some possible missteps in science communication during Covid. Clearly we need new and more better strategies of public communication in an era of declining trust l.
I wrote this piece to promote thoughtful, respectful, and rational engagement with controversial science topics. I hope it fosters constructive dialogue in the scientific community—thank you for reading and sharing 🙏🏼 @NatRevImmunol
https://t.co/iSdbikwy9p
📣 We are excited and thrilled to announce APOLLO, a healthcare system-scale multimodal temporal foundation model for virtual patient representations.
Trained on 25 billion clinical events from 7.2 million patients across 33 years and 28 modalities, APOLLO learns a unified atlas of medicine. Turning labs, notes, pathology images, medications, and diagnoses into coherent, computable longitudinal trajectories. APOLLO is disease-agnostic by design, a single model that learns the shared structure underlying human health and disease across every specialty, modality, and stage of care.
The possibilities are enormous: earlier risk prediction, treatment response modeling, clinical trial matching, biomarker discovery, and a new generation of agentic systems built on rich patient representations.
Read the pre-print: https://t.co/IUaWyodcrS
Read our blog post about the work: https://t.co/QOeUHYsrYN
👏 🎉Huge congratulations to Andrew Zhang , @TongDing99, Sophia J. Wagner, and the rest of the team.
Striking new @Nature paper on NPC: the 20.5% of southern Chinese who carry both high-risk EBV 85841G and a susceptible HLA-A background (A*11:01− or A*02:07+) account for ~47% of cases. Host–virus interaction, not host or virus alone, drives NPC risk. #hncsm
1/n
Setidegrasib the first-in-human, first-in-class, KRAS G12D-targeted protein degrader #TPD
Our KRAS G12D degrader study is now published in the New England Journal of Medicine @NEJM
https://t.co/8Juil6VN42
A new way to target KRAS G12D - one of the most common oncogenic drivers across cancers.