Why can Hepatocellular Carcinoma (HCC) often be diagnosed without a biopsy, while most other cancers cannot?
The answer lies in its unique vascular transformation.
As HCC develops, it switches from portal venous to arterial blood supply, producing the classic imaging pattern:
🩸 Arterial Phase Hyperenhancement (APHE) → 🌑 Portal/Delayed Washout ± Capsule.
In a patient with cirrhosis or chronic HBV, this pattern is so specific that LI-RADS LR-5 allows a confident diagnosis without tissue confirmation in many cases.
Most other solid tumors lack such a unique imaging signature, making histopathology and molecular profiling essential before treatment.
A fundamental concept every oncology trainee should master.
#HCC #HepatocellularCarcinoma #LiverCancer #Oncology #MedicalOncology #Radiology #LIRADS #CancerEducation #FOAMed #MedEd #DrNB #DMOncology #CancerConceptsExplained #OncoTwitter #MedTwitter
I use Olanzapine heavily in my clinical practice across multiple tumor types. 👇👇 Phase III: Netupitant/Palonosetron + olanzapine +/- DEX was noninferior to standard 4-day DEX for CINV in highly emetogenic chemo. ⬇️ steroid toxicities.
#OncTwitter#bcsm#gusm@JCO_ASCO
Honoured to present our #NeoLOCUSRetro study at #ASCOBT26.
Discussed how Carbo-Pacli+ Low-Dose Immuno + Oral Metronomic Therapy can downstage locally advanced HNSCC, enabling radical-intent treatment and improving outcomes.
Grateful to @todrashish, @drmpk91 & @OffCMCVellore.
Most oncologists can name KEYNOTE, CheckMate, or EMPOWER.
But one PD-1 program has quietly stacked positive phase III trials across lung, esophageal, and gastric cancers.
The ASTRUM program 👇
🫁 ASTRUM-005 | ES-SCLC
Serplulimab + EP vs Placebo + EP
OS: 15.4 vs 10.9 mo
HR 0.63
🫁 ASTRUM-004 | Squamous NSCLC
Serplulimab + nab-paclitaxel/carboplatin vs chemo
PFS HR 0.53
OS HR 0.73
🍽️ ASTRUM-007 | ESCC
Serplulimab + FP vs Placebo + FP
OS: 15.3 vs 11.8 mo
HR 0.68
🍽️ ASTRUM-006 | Resectable PD-L1+ Gastric/GEJ
Peri-op Serplulimab + SOX → Adjuvant Serplulimab
vs
Peri-op SOX → Adjuvant SOX
EFS: HR 0.73
pCR: 21.6% vs 6.4%
4 cancers.
4 phase III wins.
While the oncology world focused on Western PD-1s, serplulimab quietly built one of the most successful immunotherapy development programs in cancer medicine.
Is ASTRUM the most underrated trial program in oncology?
@oncoalert@ASCO@myESMO
#Oncology #Immunotherapy #LungCancer #GastricCancer
ADCs are no longer a niche therapy in gynecologic oncology.
Today, three ADCs have FDA approvals across ovarian, endometrial, and cervical cancers, and dozens more are in development.
🔹 Mirvetuximab soravtansine: FRα-positive platinum-resistant ovarian cancer
🔹 Trastuzumab deruxtecan: HER2-positive gynecologic tumors
🔹 Tisotumab vedotin: Recurrent/metastatic cervical cancer
The next challenge isn’t finding more ADCs.
It’s learning how to use them.
🧬 Which biomarker best predicts benefit?
🔄 Can patients receive sequential ADCs?
🎯 Should we switch targets or payloads after progression?
⚠️ How do we optimize management of ocular toxicity, neuropathy, and ILD?
The future of gynecologic oncology may not be chemotherapy vs targeted therapy.
It may be ADC vs ADC.
Excellent review of where the field stands today and where it’s heading next.
#GynOnc #Oncology #ADC #MedTwitter
@OncoAlert@myESMO@JCOPO_ASCO
【The 2025 Journal Impact Factors have been released】
📊 I visualized the top 50 journals in Oncology and Respiratory Medicine as bar graphs.
Of course, JIF is only one metric, but seeing the journals side by side makes the overall landscape quite interesting 👀
#LCSM
🧠 High-yield: KEYNOTE-689 vs NIVOPOSTOP
These two trials are redefining standards for resectable LA-HNSCC.
1/ KEYNOTE-689 (NEJM 2025)
Perioperative pembro → significant EFS benefit
First positive perioperative IO trial in >2 decades
2/ NIVOPOSTOP (ASCO 2025)
Post-op nivo + CRT in high-risk → significant DFS benefit
First superiority over SOC CRT in >20 years
Full comparison + practical scenarios + exam points in the image below 👇
Thread continues in comments / save for later.
What’s your current approach?
#HNSCC #KEYNOTE689 #NIVOPOSTOP
Excellent slides about definition of endocrine resistance and sequencing of endocrine therapy in 2026. From the talk by @AlexEniu@asco#asco26 🙂👍. Money 💰 Slides .
Desmoid Fibromatosis (Aggressive Fibromatosis) – Management Algorithm
The treatment landscape has changed.
Active surveillance is now the preferred first step for most patients.
Surgery is no longer routine first-line.
Nirogacestat (gamma-secretase inhibitor) has become the preferred systemic therapy for progressive disease based on the DeFi trial.
This high-yield infographic covers: • What it is & key mutations (CTNNB1 / APC) • Initial workup (biopsy, imaging, molecular) • When to treat (clear indications) • Limited role of surgery & radiotherapy today • Systemic options: Nirogacestat (preferred), TKIs, chemotherapy • Hormonal/NSAIDs – why they’re no longer routine • FAP-associated desmoid management • Practical exam algorithm + viva pearls
Perfect for residents, fellows & exam prep (DrNB/Medical Oncology).
Save it for quick reference. Share with your team.
What’s your current approach for a progressive mesenteric desmoid in a young patient?
#Desmoid #DesmoidTumor #AggressiveFibromatosis #Sarcoma #Oncology #MedicalOncology #CancerEducation #MedEd #ClinicalPearls
CHEMO-IO VS IO ALONE IN PD-L1 ≥50% NSCLC
• IPD network meta-analysis of 24 phase III trials (n=5,546)
• OS: 29.2 vs 19.8 months (+9.4 months)
• PFS: 11.3 vs 6.8 months (+4.5 months)
• Fewer early progressors with chemo-IO
• Greater toxicity with combination therapy
• Not a head-to-head randomized comparison
PD-L1 ≥50% may not be enough reason to omit chemotherapy.
Di Federico et al. • JAMA Oncology 2026
#NSCLC #LungCancer #Immunotherapy #MVOnco
What did ASCO 2026 change?
Some standards of care have now moved by years.
That almost never happens.
BRAF colorectal, pancreatic KRAS, and DDLPS sarcoma
are three of oncology's hardest diseases
SOC moved by > 1yr:
▫️BRAF mCRC: 15.1 → 30.3 months OS
▪️Pancreatic KRAS: 6.7 → 13.2 months OS 🏆
▪️DDLPS sarcoma: 1.5 → 9.7 months PFS ⭐️
(sarcoma went from "nothing" to a win).
Myeloma, GIST, HR+/HER2- breast, uveal melanoma, bladder, prostate, and RET+ lung cancer moved too.
This is what decades of funded science look like when it compounds.
- - - - -
Source: Jori (@jori_health)
𝘗𝘭𝘰𝘵 𝘱𝘦𝘦𝘳-𝘳𝘦𝘷𝘪𝘦𝘸𝘦���� 𝘣𝘺 𝘦𝘪𝘨𝘩𝘵 𝘰𝘯𝘤𝘰𝘭𝘰𝘨𝘺 𝘦𝘹𝘱𝘦𝘳��𝘴. 𝘛𝘩𝘢𝘯𝘬 𝘺𝘰𝘶 <3
- - - - -
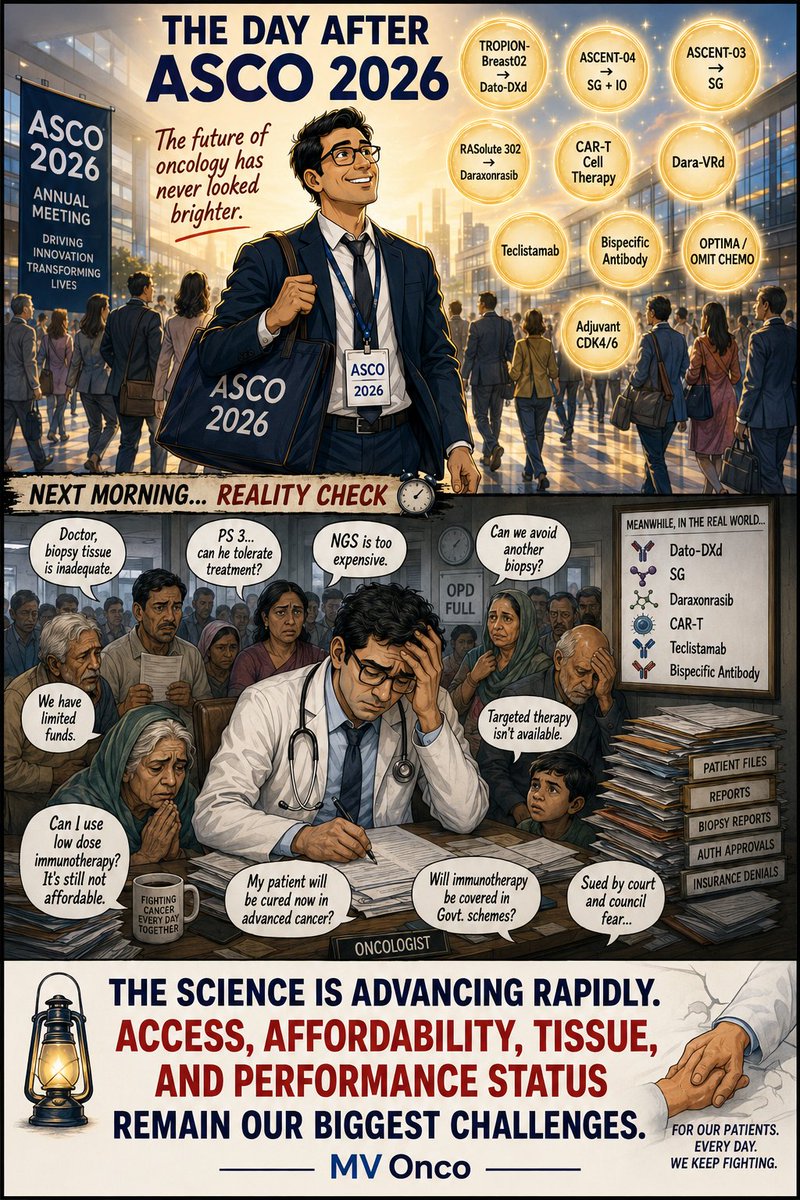
ASCO 2026 gave us Dato-DXd, SG, Daraxonrasib, CAR-T, bispecific antibodies, and many reasons for optimism.
The next morning in clinic, the questions are often different:
• Is the biopsy adequate?
• Can the patient tolerate treatment?
• Can they afford NGS?
• Will immunotherapy be covered?
• Is the drug even available?
Science is moving faster than ever.
Access, affordability, tissue adequacy, and performance status remain some of the biggest challenges in oncology.
#ASCO2026 #Oncology #CancerCare #MVOnco