(1/x) Those of us who love #pocus often use it to rule out pneumothorax.
But how reliable is this approach? So-so.
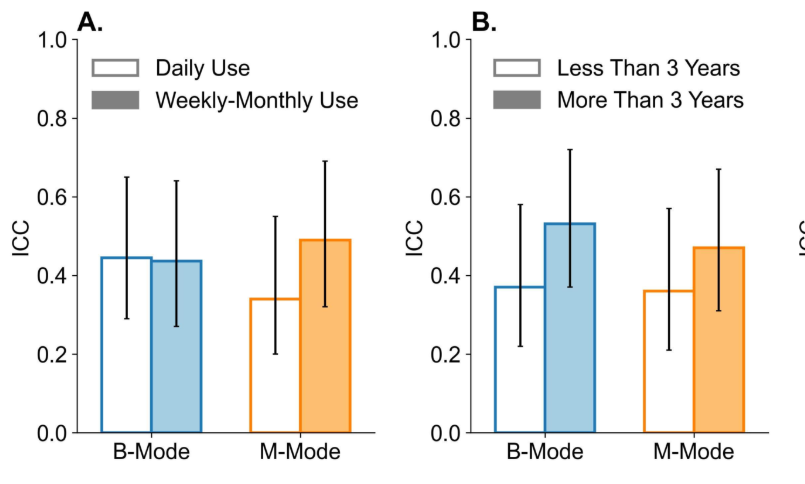
We found only moderate interrater reliability to detect lung sliding among clinicians.
Want to perform high quality clinical research? The best piece of advice I've received is to focus 10x more on creating an unimpeachable research protocol.
This is how I do it step-by-step:
1) I start with a manuscript template for the study design I am using (linked below 👇)
2) Fill out the template / design the study in as much detail as possible. This includes writing the entire introduction, methods.
3) For the results, create the actual data tables you will want to publish for your paper (this will make sure you are collecting all the data)
4) Think about what figures you will want to generate --> pencil these in
5) Write 3-4 discussion points you intend to make if your hypothesis holds true (you aren't bound to these).
6) Next, check your manuscript protocol against @EQUATORNetwork checklists for reporting completeness --> are there any methodological things you haven't considered?
7) Next, send your protocol to all your co-investigators for review --> this is the time to decide whether the study should be done as is or should be reworked. You don't want to finish your study and have everyone say "why did we do it this way?" . After the study is done its too late!!!!
8) Publish your protocol on OSF (or another online protocol registry) for transparent open science.
I know this seems like a lot of work, but it takes about 1/10th the time to do it right the first time than to start a study, realize there is a fundamental flaw, and pivot/redesign (from personal experience).
Hope this help, templates below 👇
For new #ICU fellows the learning curve is STEEP.
On reflection, the best fellows seem to master core groups of skills in a somewhat predictable order.
Here is my take on the "Maslow's Hierarchy of Needs" equivalent for ICU skills.
1st: Resuscitative Skills --> without competence in resuscitative skills, general ICU care suffers. For example, if you aren't confident in your intubation skills, you won't make the best decisions about EXtubation.
2nd: Core ICU Management Skills --> Some doctors can be excellent at resuscitation, yet lack in the ability to provide excellent ongoing ICU care. The truth that some trainees realize too late imho is that resuscitation is only part of critical care --> the bread and butter is managing complex medical patients on ventilators.
3rd: Family Communication Skills --> Once excellent patient care in the ICU is being mastered (or in parallel with this), excellent fellows master communication with families. A different yet crucial skill set.
4th: Team Management Skills --> Part of being an excellent intensivist is coordinating a multi-disciplinary team. This takes time and practice, and involves the team trusting you to make solid clinical decisions.
Last: Resource management --> The final piece to master for many trainees is resource management. This can be at a unit, hospital, or regional level.
Of course, no one ever truly masters any of these and we always have so much to learn, but just a pattern i've observed in our best ICU fellows.
(4/x) Thus, if the IVC can only tell us a couple pieces of information of left sided congestion AND we are trying to understand a patient complex hemodynamics, why even assess it?
Good use cases for IVC:
1. A collapsible IVC indicates low mean systemic filling pressure --> this can be 1) normal 2) hypovolemia 3) vasodilation. In a patient with shock, this helps rule out cardiogenic or obstructive shock.
2. In a patient with AKI where the question of right sided congestion is raised, a totally collapsible IVC argues against right sided congestion coming from the heart causing the renal failure.
(1/x) Venous congestion is not just about volume overload.
A 🧵 on diagnosing and treating individual sub-types of congestion based on their underlying cause.
#foamed#medtwitter
Interested in coming to Canada and doing a critical care ultrasound fellowship @westernsono ? We would love to have you.
Shoot me a DM and we can chat more!
Highlights:
- 6 months - 1 year (preferred 1 yr)
- any training background invited to apply
- supervised by @arntfield@john_basmaji and myself
- tons of resus / critical care TEE exposure
- ++ research opportunities (including the ability to focus this as a research fellowship) --> we are running observational + RCTs in ultrasound
I completed this fellowship a while ago and can attest first hand how great it is (over 25 graduated fellows over the past decade). We would love to have you.
Pinging some previous fellows too in case they want to highlight their experience: @KiranRikhraj@katiewiskar@HansClausdorff@DCBrotherston@LintnerRivera@msattin4
#medtwitter #foamed #pocus
(1/x) Here's our paper on the medico-legal risks of #pocus 🧑⚖️
A better title: How not to get sued performing POCUS. A 🧵
Teaser: You can be sued performing #pocus...
Please share to help spread best #pocus practices 🙏
https://t.co/MTialTQixQ
@arntfield@derwuk@NephroP@ArgaizR
#medtwitter #foamed #foamus #meded
As an AI solutions provider in a specialized area of lung ultrasound, it can be a challenge to convey the scale and reach of the problems our team is solving. Our latest video invites you to better understand how we are transforming respiratory imaging! #medtech#ai#ultrasound
Excited to announce the launch of https://t.co/gAex5B5veg a free online platform to help clinicians and researchers perform high quality, efficient, and impactful research (simply!) Have a look at our early features, blogs, and resources and share the news! #medtwitter#foamed
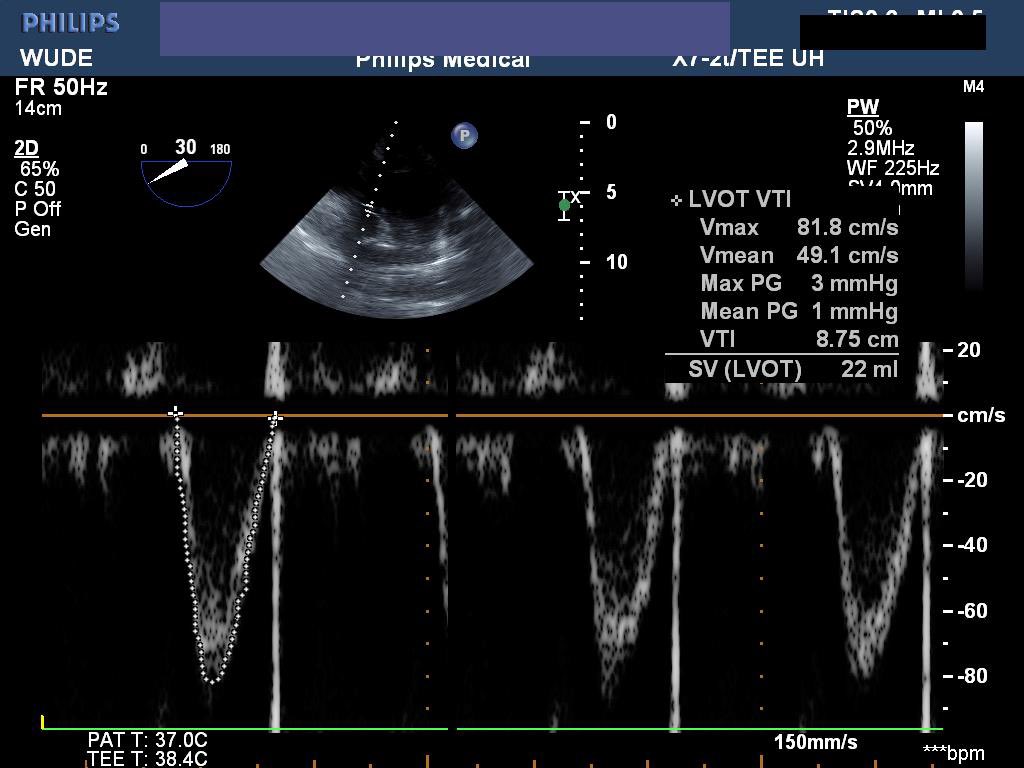
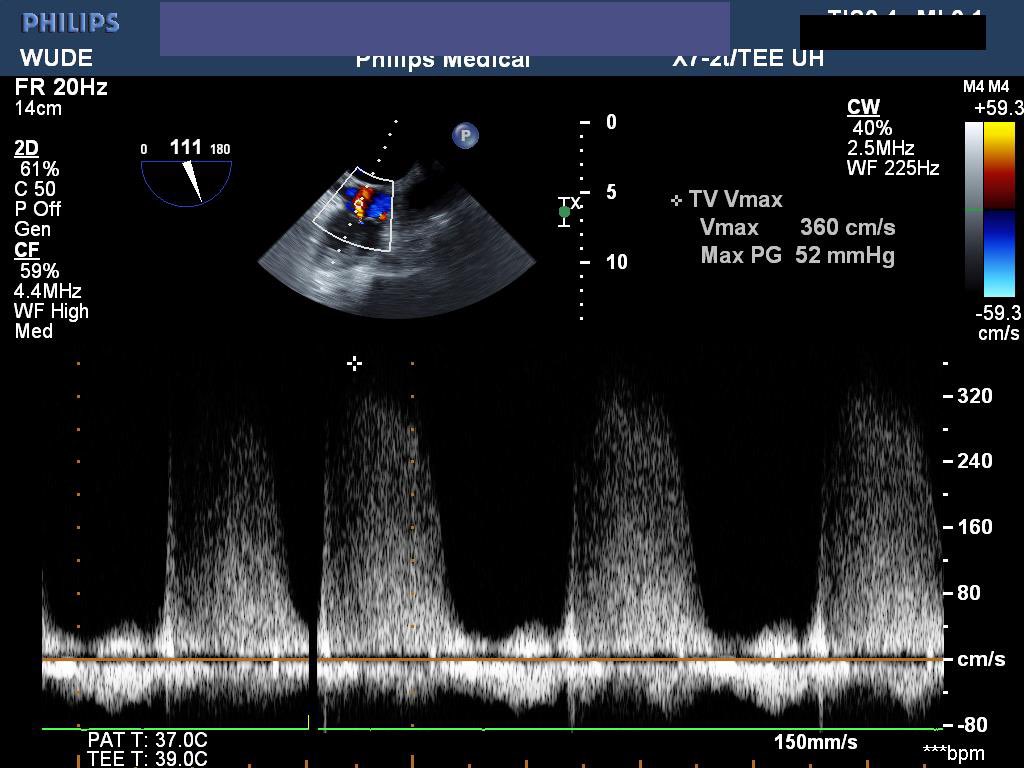
(1/X) Challenging case of LVOT obstruction. Post IR procedure for intrabdominal bleeding. Rapidly rising vasopressor requirements (yet no drain blood from drain). Initial POCUS shows:
@hraza222@westernsono Thanks man! Case still running its course with a new team now. Still high doses of pressors/inotropes and on CRRT for refractory pulmonary edema. POCUS helped us create a roadmap for her, hopefully can pull through
Great #hemodynamic#pocus#tee case on last ICU shift for a while 💔 50sF from periphery w/ spont occipital bleed, SDH, PEA arrest ⬇️⏱️6 min, anterolateral ST⬆️ & ⬆️ trops. Arrived on Levo 30, vaso 2.4, milrinone 0.125 @westernsono@hraza222