How the ECG Tells You Where VT Is Coming From
1️⃣ When a rhythm comes from the ventricles, it travels slowly across muscle instead of racing through the Purkinje system. That’s why VT is wide, fast, and regular.
#CardioNuggets
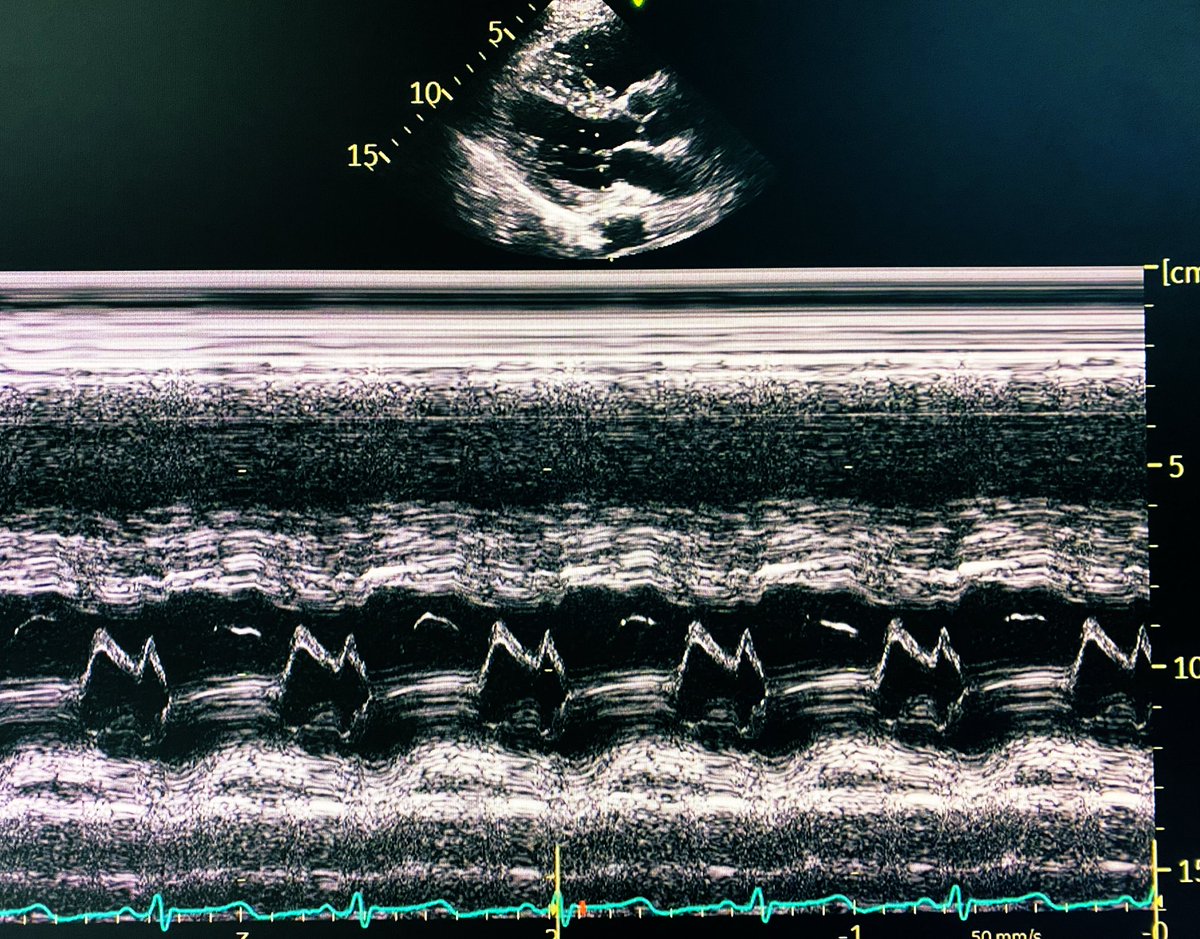
“Teardrop Heart” in Congenital Absence of Pericardium
🫀 Why the “teardrop” shape?
• No pericardial restraint → heart is unusually mobile in the chest
• Leftward displacement → heart shifts toward the left hemithorax
• RV can appear abnormally prominent and findings may mimic those of ASD
✨ Result:
• The LV elongates and stretches downward
• Cardiac silhouette appears narrow superiorly + bulbous inferiorly
#CardioNuggets #MedEd #CardioMed
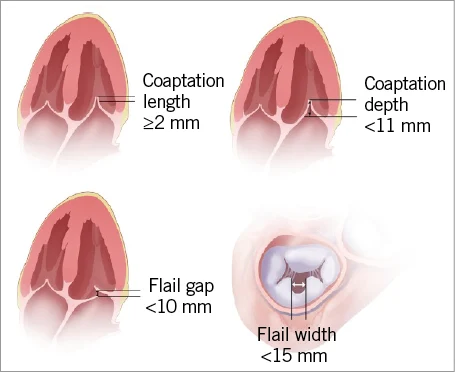
🫀 #CardioNugget: Flail Gap vs Flail Width in MR
📍 Flail Gap
➡️ Distance between the flail leaflet tip and the coaptation line
➡️ Think: “How far is the leaflet flying into the LA?”
🔴 Larger gap = more severe MR
✅ MitraClip-friendly: <10 mm
📍 Flail Width
➡️ Medial–lateral extent of the flail segment
➡️ Think: “How wide is the damaged portion?”
🔴 Wider segment = more complex repair
✅ MitraClip-friendly: <15 mm
🎯 Why it matters?
Both help determine severity + feasibility of transcatheter repair (e.g., MitraClip)
#CardioNuggets #MedEd #TEE #MitraClip
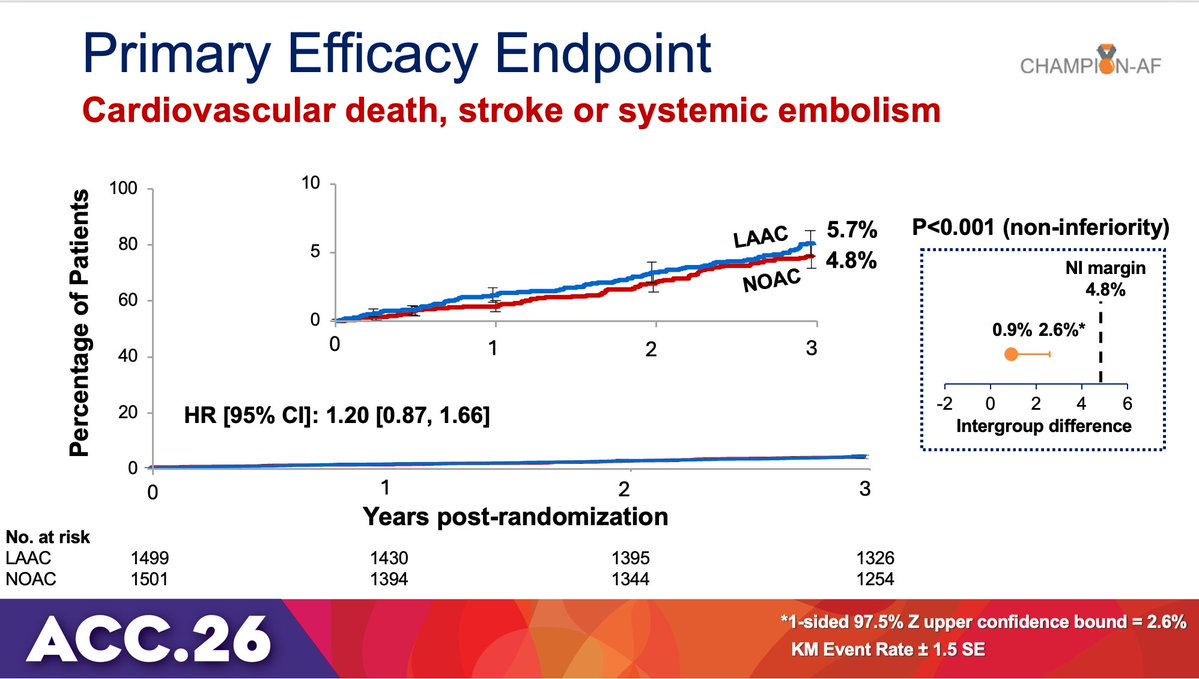
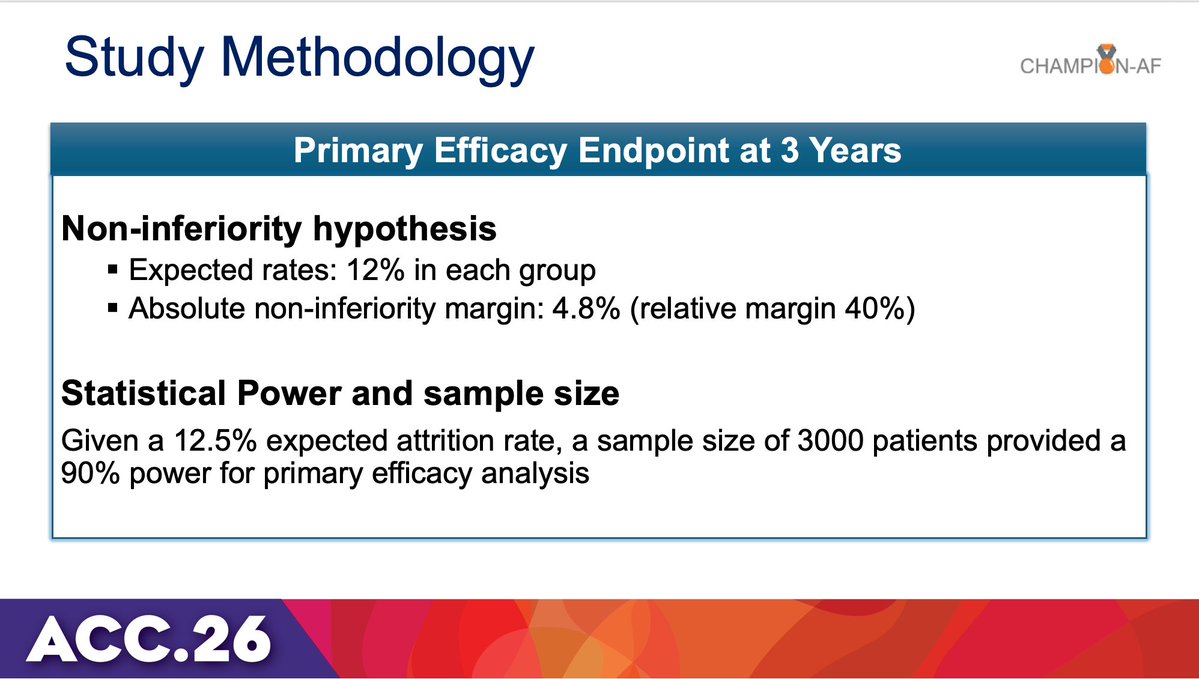
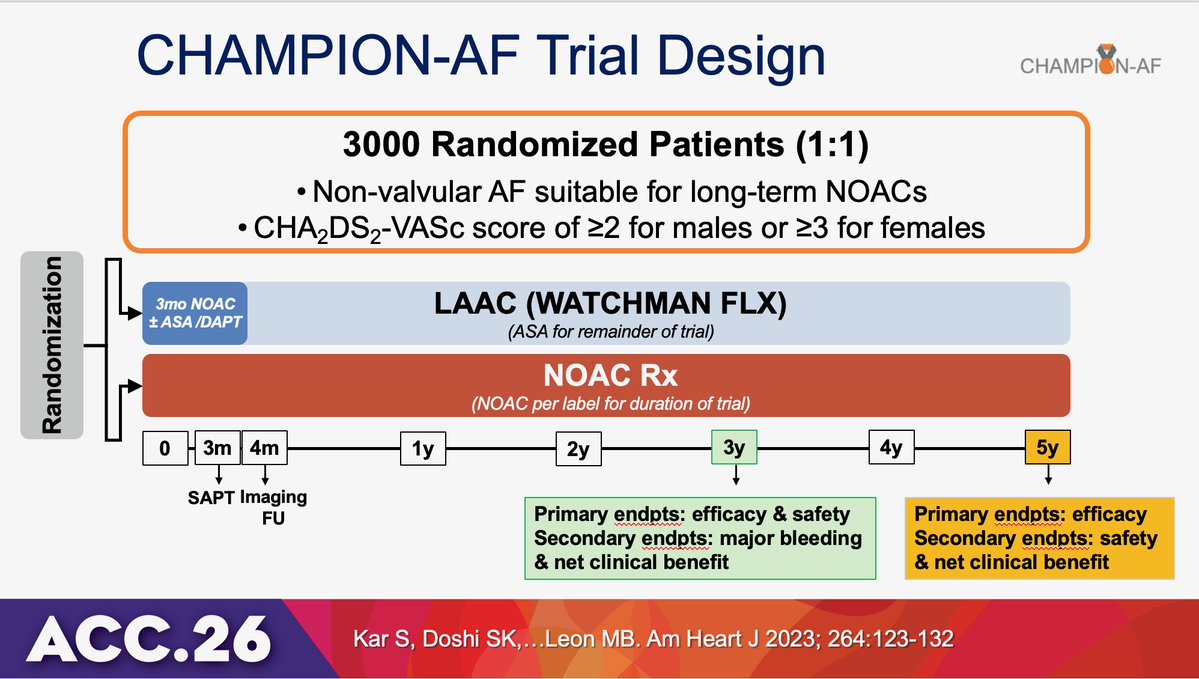
🌟#CHAMPION-AF at #ACC26
📍n=3000 NVAF
📍WATCHMAN FLX LAAC vs NOAC
✅LAAC met NI for 3y CV ☠️, stroke, or systemic emb
✅🩸 lower w LAAC
⚠️Important caveat: the NI margin was 4.8%, as large as the overall event rate.
Large NI margin only non-proc bleeds included
Presented at #ACC26:
Among patients with a preserved ejection fraction at least 1 year after myocardial infarction, stopping beta-blockers was noninferior to continuing therapy with respect to major clinical outcomes. Full SMART-DECISION trial results: https://t.co/dZS03RaTcA
@ACCinTouch
Great presentation on prevention medications. One thing I noticed- a lot of us still hesitant to prescribe GLP-1’s to our patients when indicated. Was great to have some more insights on GLP1 in cardiology practice. @ACCinTouch#ACC26#GLP1
Digoxin in Rheumatic Heart Disease (DIG-RHD)
RCT evaluating digoxin in patients with HF with rheumatic heart disease
❤️ A long-standing therapy now undergoing rigorous evaluation in a contemporary population needed
Key results
💊4% relative risk ⤵️ of primary endpoint driven in those tx with digoxin by ⤵️ worsening HF
💊 Hospitalization for HF was very infrequent (2.8 vs. a mortality rate of 4.9 per 100 patient-years)
💊 1st trial evidence for digoxin as a safe treatment for reducing HF worsening in RHD
#ACC26 #GlobalCardiology #ValvularHeartDisease #LBCT #rheumaticheart
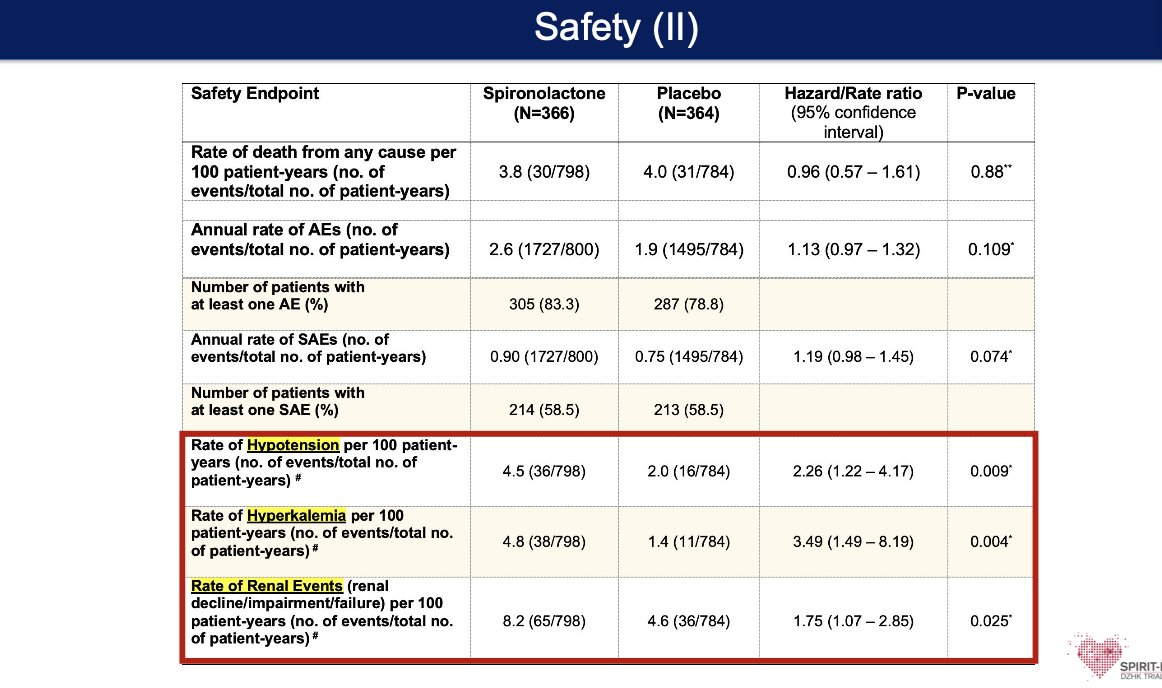
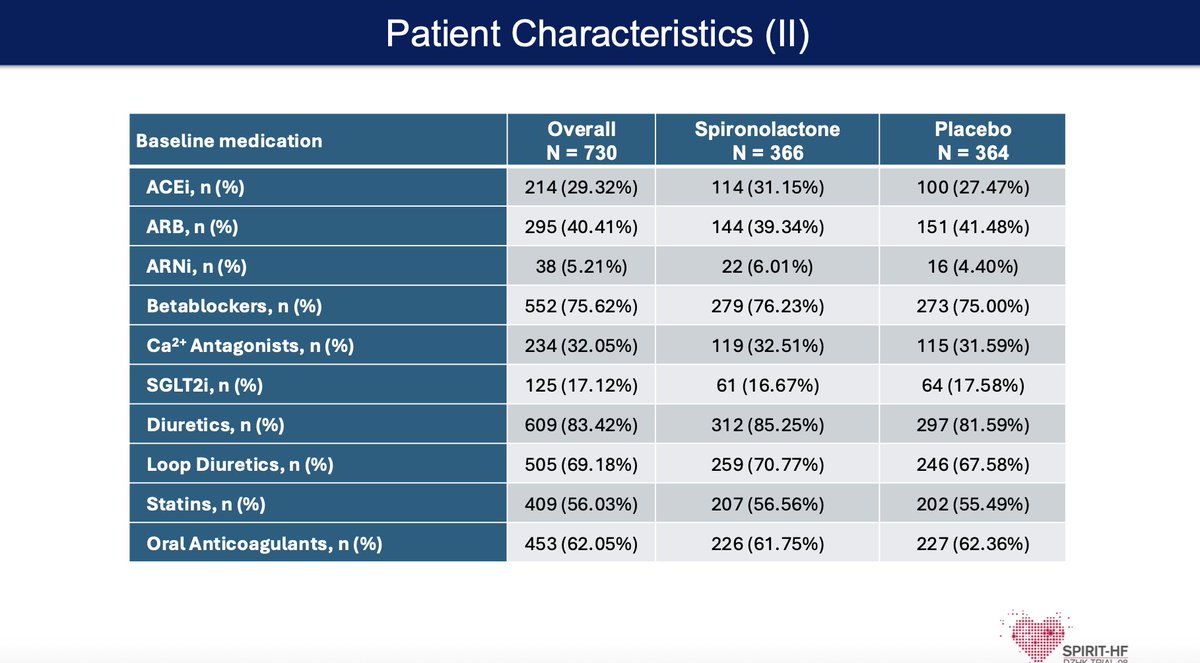
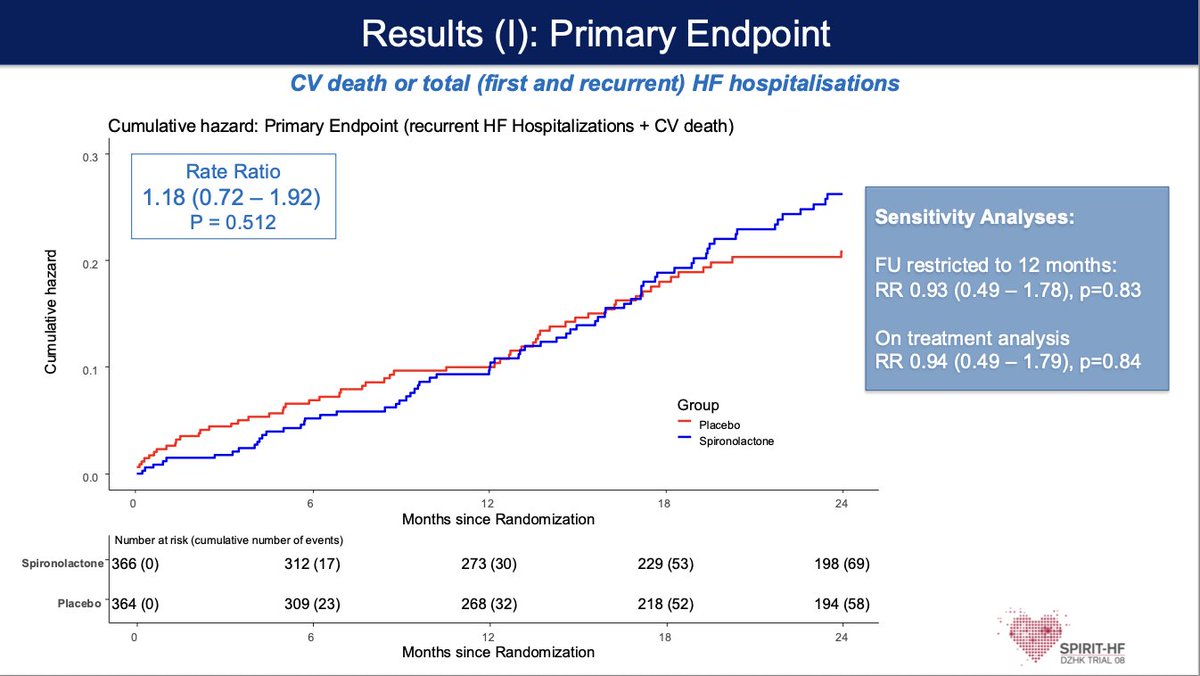
#SPIRIT-HF #ACC26
🧑⚕️ HF with preserved or mildly reduced EF (HFpEF/HFmrEF)—a large, underserved group with limited therapies
🧠 Does Spironolactone reduce CV death and HF hospitalizations, building on signals from prior trials like TOPCAT
📊 Trial was underpowered (COVID impact, lower enrollment, high drug discontinuation) → unable to definitively test hypothesis
⚠️ No clear primary outcome benefit; side effects and drug withdrawal were common, potentially blunting efficacy
💡 Takeaway:
Signal for benefit may still exist—but tolerability + adherence remain the real barriers in HFpEF therapy
Great Discussion by @dranulala 👏👏
#ACC26#LBCTSession1️⃣
🔑 HI-PEITHO : catheteter directed fibrinolysis + AC is comparable w AC alone for intermed. risk PE
🔑 CHAMPION-AF: LAAO is non-inf to NOAC for AF pts eligible for AC
🔑 STEMI-DTU: No benefit of Impella +DTU of 30 min over immediate PCI for MI w/out CS
Want to join the @CardioNerds family?
Application for next year’s Academy class is live!
📣 Looking for residents & fellows interested in cardiovascular medical education
🔗 https://t.co/qK0ZSfAgtu
⏰ Due May 11th
Come meet us at #ACC26
https://t.co/me26TJ28NT
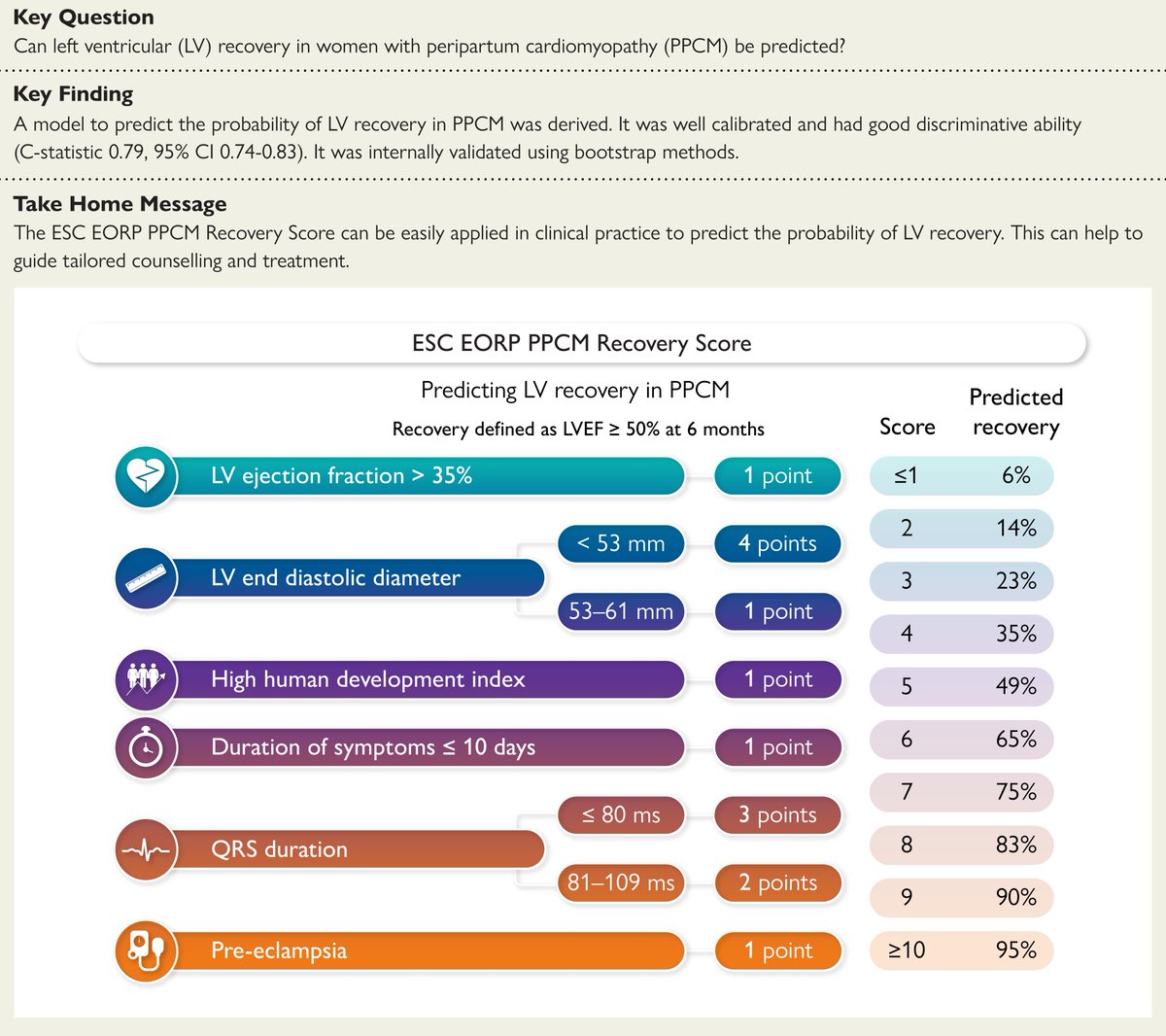
In a new Review Article, Dr. Zoltan Arany (@AranyLab) discusses the epidemiology and clinical presentation of peripartum cardiomyopathy, as well as the mechanistic basis for potential therapeutics. Read the full article: https://t.co/C7N3RGjIJY
Important advice from Prof. @JBauersachsMD to help you recognise and diagnose peripartum cardiomyopathy.
Watch the 4-minute discussion on #ESCTVToday – free online, on demand. https://t.co/uKrHbP8Lpw
Sign up so you get every #ESCTVToday episode https://t.co/kXj70s9OC9
Peripartum cardiomyopathy is now the leading cause of maternal death in many parts of the world.
A new Seminar summarises current knowledge of peripartum cardiomyopathy genetics, pathophysiology, diagnostic approaches, medical management, and outcome: https://t.co/Gn5lciA0Qb
#ESCCongress
Peripartum cardiomyopathy updates from the 2025 ESC Guidelines on cardiovascular disease and pregnancy (based on the slide) 🌸🫀✨:
1️⃣ Modified WHO 2.0 Classification
🟢 More granular risk stratification for maternal CV risk:
Mild LV impairment (EF >45%) 🟢
Moderate LV impairment (EF 30–45%) 🟡
Severe LV impairment (EF <30% or NYHA III/IV) 🔴
2️⃣ Peripartum Cardiomyopathy (PPCM) Highlighted 💡
⚡ History of PPCM is now integrated into risk categories:
•Previous PPCM with only mild residual LV impairment ➡️ mWHO 2.0 III 🟡
•Previous PPCM with >mild residual impairment ➡️ mWHO 2.0 IV 🔴
3️⃣ New Recommendation: Genetic Counseling 🧬
🌟 Genetic counselling & testing should be considered in women with PPCM.
🔖 Class IIa, Level C ➡️ highlights the importance of precision medicine and family risk evaluation.
4️⃣ Extended Heart Failure Therapy ⏳
💊 Even after LV recovery, HF treatment should continue for ≥12 months to ensure stability.
📝 Based on EF and LV volume normalization.
🔖 Class IIa, Level C.
5️⃣ Clearer Long-Term Risk Communication 🗣️
🔴 Severe LV impairment or prior PPCM with persistent dysfunction is now a contraindication to pregnancy.
#ESCCongress @escardio