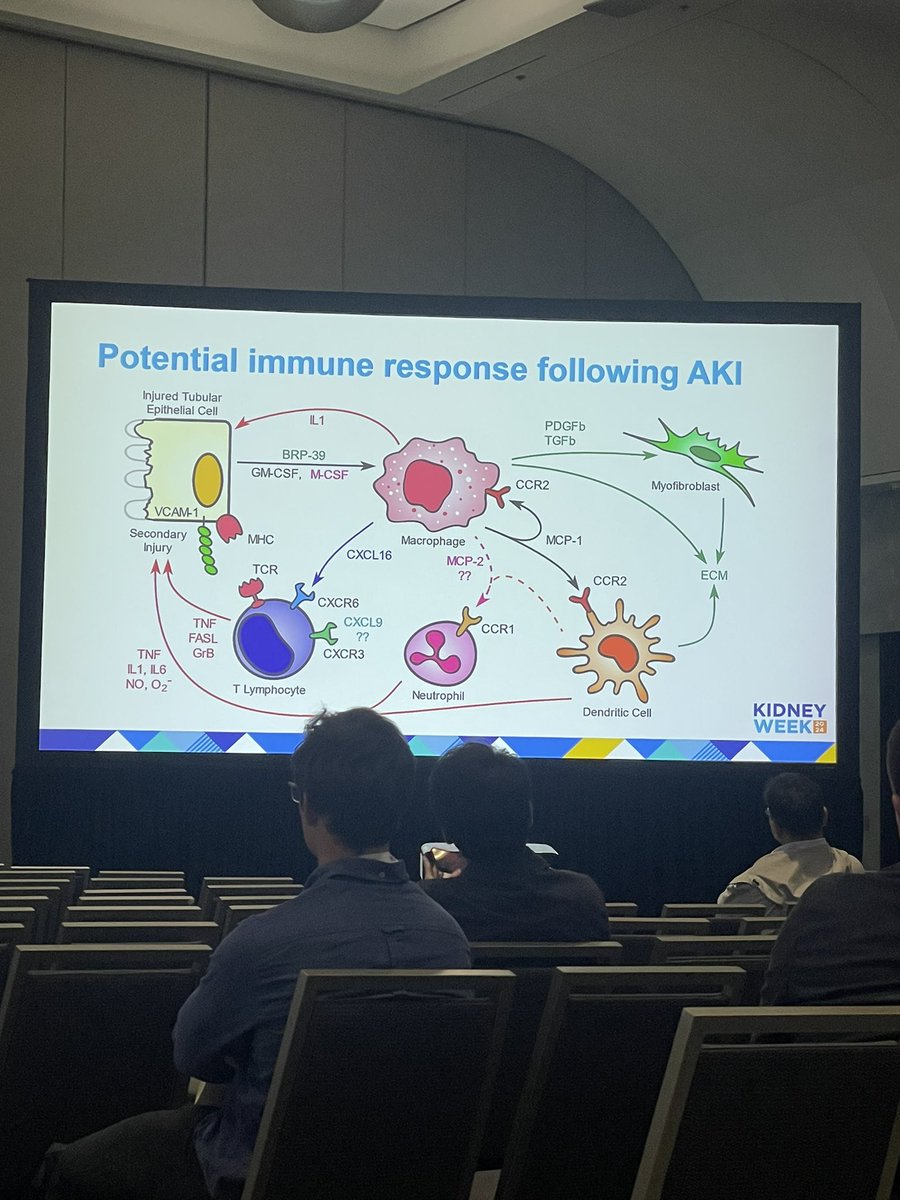
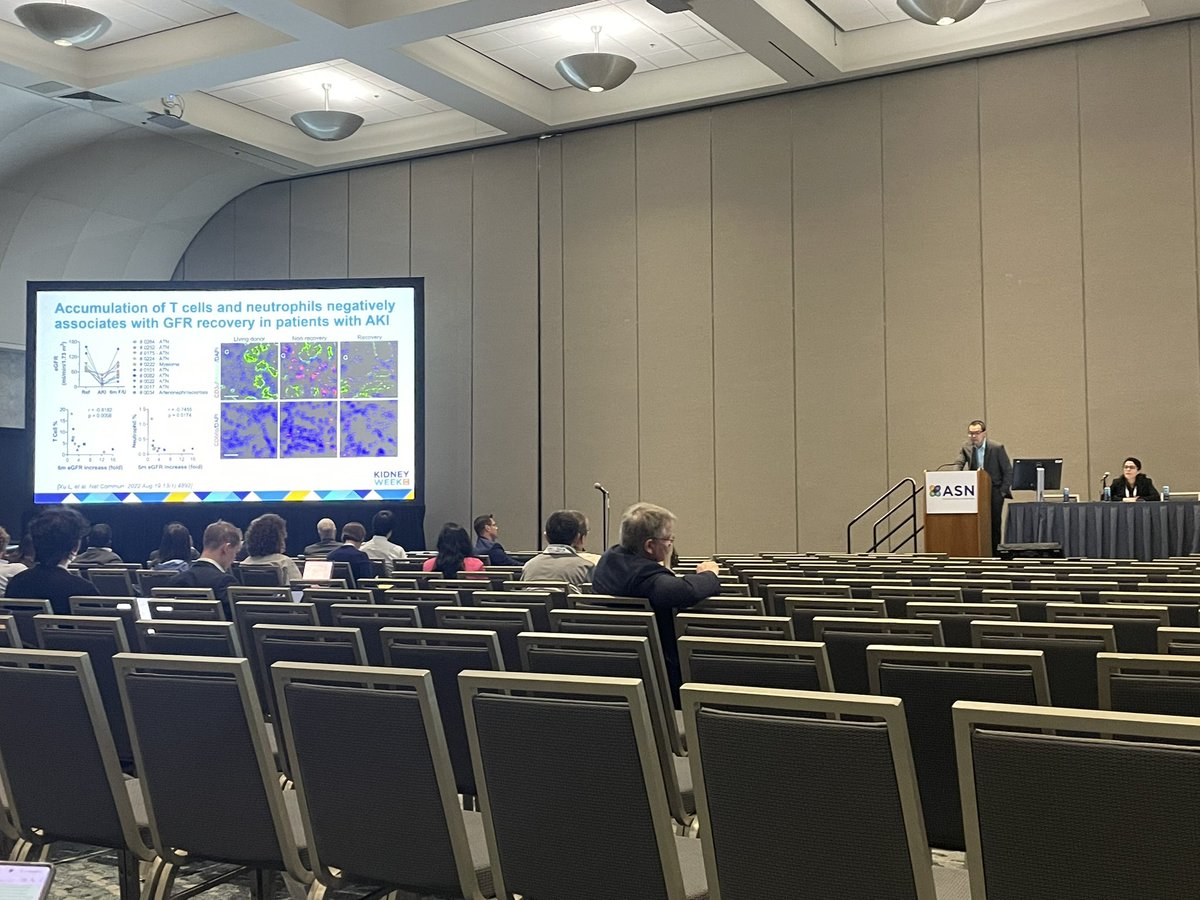
1 in 5 patients develops acute kidney injury (AKI) within the first year of starting cancer immunotherapy.
Researchers are investigating whether checkpoint inhibitors are causing acute interstitial nephritis.
Read more in the Q&A with @dmoledina.
https://t.co/GZPaG8t1Ir
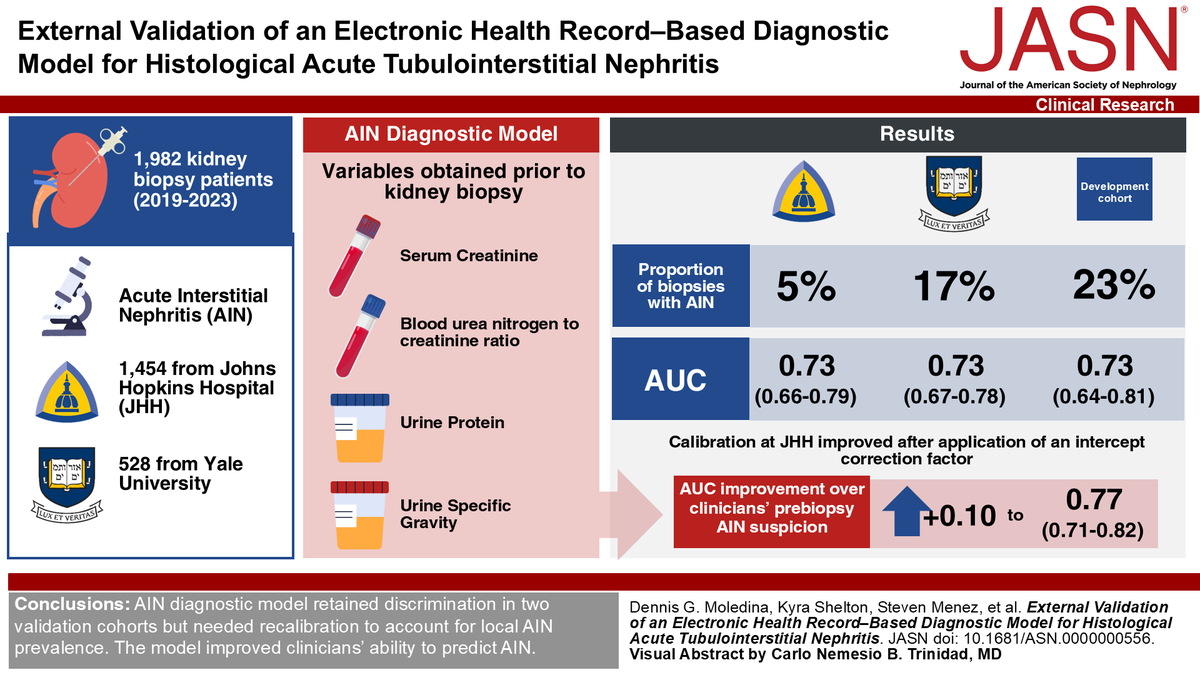
New @hopkinsneph study uses new electronic diagnostic model as an alternative to kidney biopsies to predict AIN. @KidneydrChirag
https://t.co/dDLDboUpUg
I hope people will use the AIN calculator to differentiate AIN from ATN on AKI consults. Let us know if you have questions or additional suggestions. @dmoledina
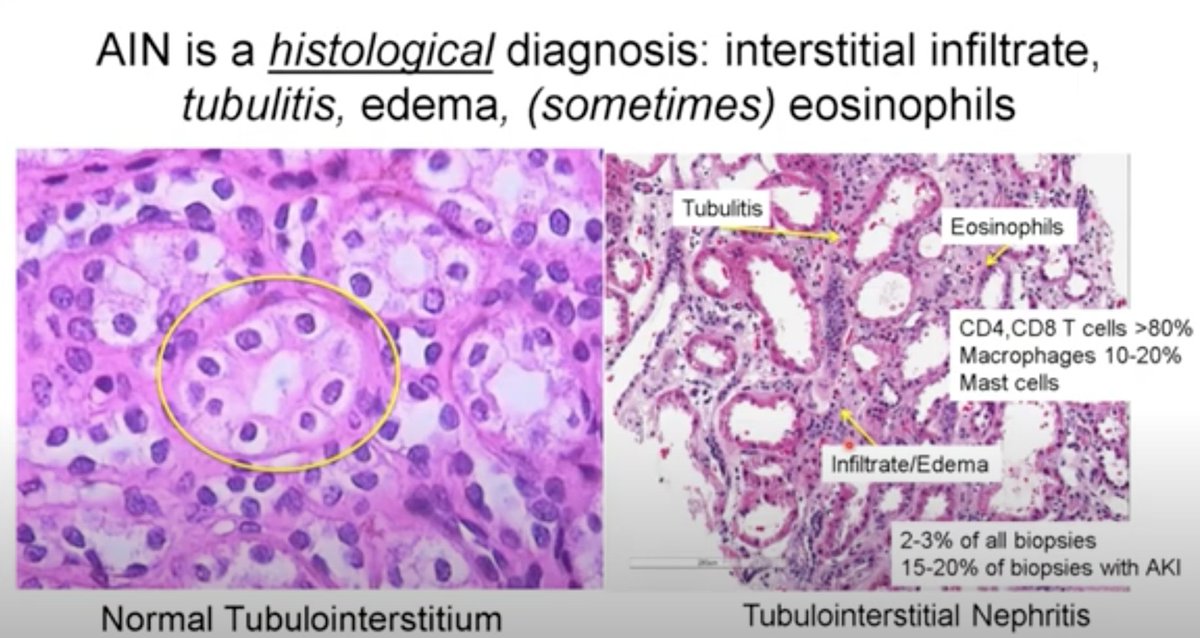
Accurate diagnosis of acute tubulointerstitial nephritis (AIN) often requires a kidney biopsy. This study found that an AIN diagnostic model retained discrimination in two validation cohorts but needed recalibration to account for local AIN prevalence. https://t.co/GyqeGwIf62
@dmoledina@fperrywilson@kidneydrchirag@Nephronette@oconnkyle@StevenMenez
A new #clinicaltrial led by @YaleIMed's @dmoledina seeks to use biomarkers to detect when kidney injury results from #immunotherapy complications, reducing treatment interruptions for patients with #cancer. Learn more in a YSM Q&A: https://t.co/yGKezi6RWj
@hswapnil @NephroGuy @rmohty@onconephsociety We had urine PDL1 (not PD1) in our olink proteomics data. 1.7 fold higher in AIN (pval=0.007, qval=0.03). CXCL9 was 7.6-fold higher in AIN.
@hswapnil @NephroGuy @rmohty@onconephsociety very cool study - urine sPD1 could be a biomarker of ICI-AIN vs. other AIN (2.7 fold higher). i can't figure out if there is any difference in non-ICI-AIN vs. ATN. We didn't measure this so can't really tell which one performs better (CXCL9 vs. PD1).
@hswapnil@NephroSeeker@NephJC This is the really good study looking at PPI-AIN /PPI-AKI. 2-3 fold higher hazard of both but low incidence of bx-proven AIN (though certainly some could’ve been missed). https://t.co/QeS47Pdft7