What's your diagnosis:
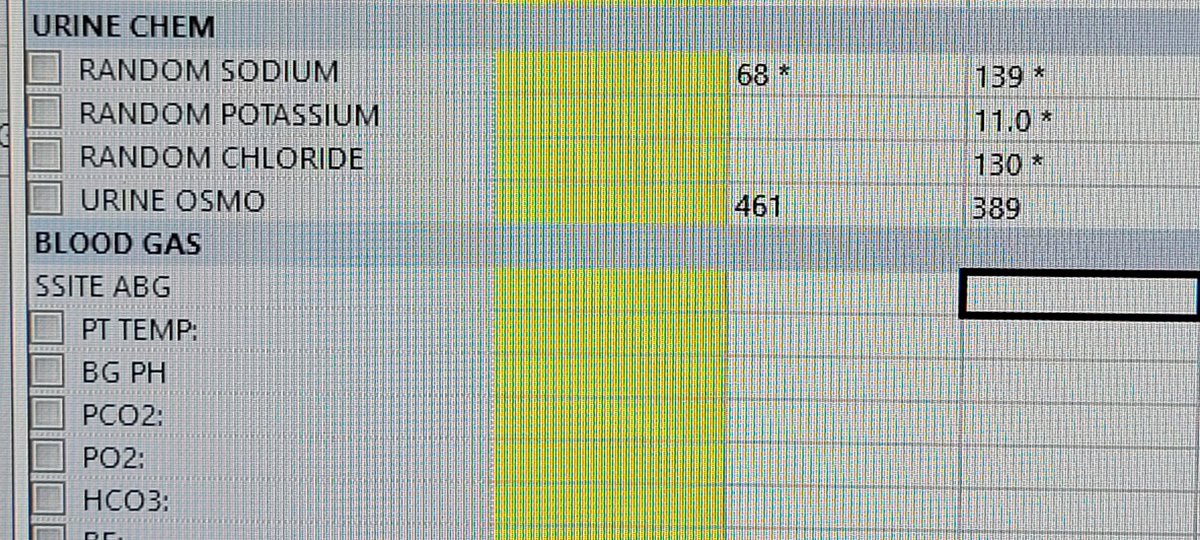
40/f consult for polyuria, adm for pancreatitis sp lap chole, on TPN, Saline 125/hr
Output 6.4 litres
Sodium 132, bun 10, serum Osm 310
TG 1006, glucose 250
Urine studies attached
@JohnRMontford It's a policy in most units here. Burden, sure.
I couldn't find direct data.
We know incidence of hyperkalemia is 2.0 to 2.4 times after long interdialytic interval. Dialysis units don't ve tele...for discuss, what would be YOUR threshold of missed treatments for sending to ER?
Update:
Biopsied. 80 glomeruli, beautiful smaple. Hypertensive nephropathy. 30% glo-sclerosis,20%IFTA. No necrosis.
Surprisingly no AIN or ANCA vasculitis or interstitial nephritis
#askrenal#nephropath#anca#mpa
Part 1: 87 yo female with no recent med changes but prolonged PPI usage. Wors ring gfr last few months. Progressive eosinophilia from 6% to 9% (aec 202 to 470) , gfr 31.
No precious UA from pcp....
PPI changed to h2 on first consult
Part2:
Workup p-anca 1:40
Mpo 53 (strongly positive)
UA 10-20 wbc, no rbc
24 hr urine protein 92 mg
Gfr stable...
Abs eos down 323
1. Can you see high MPO in ac interstitial nephritis
2. Would you biopsy / approach
#askrenal#nephrocase
Part 1
48/M with Diabetes w/ retinopathy. Cr 1.8. proteinuria 2.5 gram per gram. UA no micro hematuria. Albumin 4. LDL 78 (on statin at consult)
UPEP 89% albumin. Repeat UPEP 86% albumin. Kidney bx Nodular diabetic Glomerulosclerosis. Thicked BM as expected
@bottomleymatt No extra renal manifestations..Tiredness and fatigue (multifactorial).
Noted some cases of anca presenting interstitial nephritis in literature....
No microhematuria seems unusual if active lesions...
No asthma /respiratory history
@MeloneyOliveira@TWhittier_RUSH@Rush_Nephrology@RushDOIM Was this patient kept NPO between labs 1 day ago and subsequent 6 am? Starvation ketosis ? Especially if non-oliguric that can give the associated gap and non gap acidosis. Hypoglycemia also concerning for same.urinalysis with ketones? Will check Beta hydroxy butyrate
@NephroGuy @GlassockJ@askrenal Correct
No large efficacy trials of spironolatone in dkd for hard renal outcomes. Finerinone has composite renal outcome data.
#askrenal#hyperaldosteronism#diabeticnephropathy#angiotensin
Would ace inhibitors/arb be still as efficacious for diabetic nephropathy in a patient with concomicant primary hyperaldosteronism given that renin/ angiotensin pathway is significantly suppressed anyway ?
@RenalFellowNtwk Quite a common scenario unfortunately in a lot of hospitals. When nephrologists are consulted, we can be effective gatekeepers. Establishing PICC team protocols with a reflex nephrology communication for any PICC in eGFR<45 can be helpful...