Clinical Quiz
🔸45 year old man presented with muscle weakness and pain for 6 months. He had difficulty in getting up from squatting position, climbing up stairs and while reaching for objects above shoulder height.
🔸On examination, he had enlarged tongue (macroglossia) and hypertrophied calf muscles (see the image below).
🔸Serum CPK was 9600 U/L (normal range: 85-170). EMG was myopathic.
What is the most likely diagnosis?
If you have fatty liver (MASLD/MAFLD), you’ve probably been told that Just do BRISK WALKING
But most people don’t know what “brisk” actually means physiologically.
A short thread 🧵
62♂.
No significant PMH.
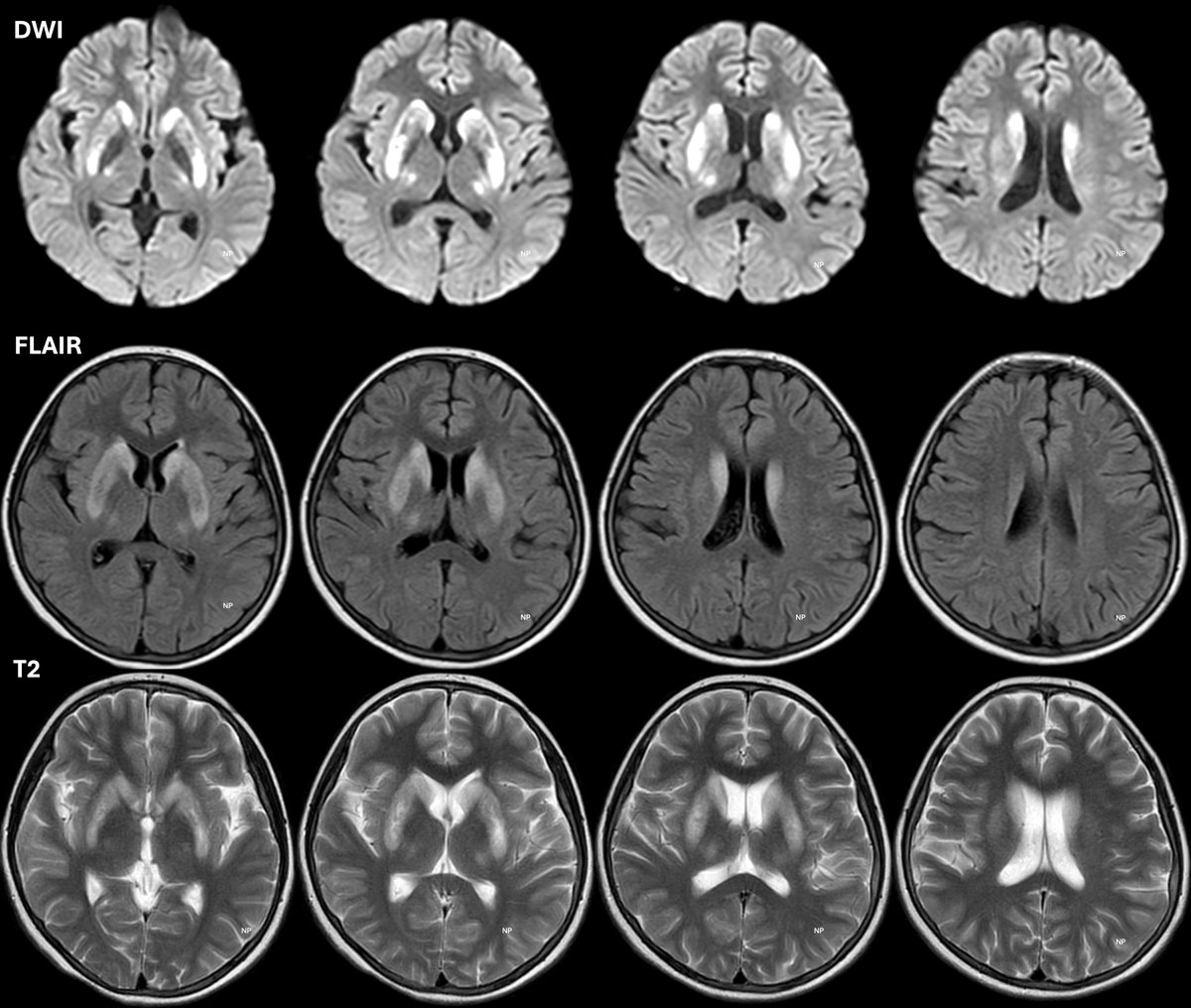
~18 months h/o progressive decline in language abilities: speech, comprehension & recently writing.
We neurologists should know where to look👀
T2 MRI 👇
A 62-year-old man presented with progressive limb weakness and involuntary movements. Take the Clinical Challenge.
What is your diagnosis?
https://t.co/kAcekr61dM
A 36-year-old male presents with intermittent dull right-sided abdominal pain for 2 months, associated with progressive abdominal distension and gradual vision impairment. There is no fever, vomiting, or urinary symptoms.
A positive family history reveals similar illness in multiple siblings.
Examination Findings
BP: 160/95 mm Hg
Hepatosplenomegaly
Ophthalmology: Peripheral corneal opacities
Laboratory Clues
↑ Serum creatinine
Normocytic anemia
↑ Total cholesterol & triglycerides
Very low HDL-C
🧠 Most Likely Diagnosis
Lecithin–Cholesterol Acyltransferase (LCAT) Deficiency
What is the mode of inheritance of this disorder?
✅ Autosomal recessive
🔍 Clinical Reasoning
Multisystem involvement (eye, liver, kidney, lipids) suggests a metabolic enzyme defect
Corneal opacities + low HDL + renal dysfunction are classic for LCAT deficiency
Affected siblings with unaffected parents strongly indicate autosomal recessive inheritance
📌 Clinical Pearl
Think LCAT deficiency in young adults with corneal clouding, hepatosplenomegaly, renal dysfunction, and very low HDL, especially with sibling involvement.
🩺 Management Snapshot
Supportive care & CV risk reduction
BP and lipid control
Monitor for progressive renal disease
Future directions: enzyme / gene replacement therapies
🔹 CME INDIA | Rare Dyslipidemia Awareness | Genetics in Clinical Practice
New joint pain + clubbing = search for cancer.
Why ..let’s decode👮🏾🕵🏽♀️
A 60-year-old man came with history of 8 weeks of joint pain.
Also mentions breathlessness + dry cough. Hands show clubbing.
X-ray shows periosteal new bone formation and tram-line sign.
But CT chest changes everything...
👉 Diagnosis is easy : Hypertrophic osteoarthropathy (HOA)
How do you diagnose HOA? 🦴🫁
🔹 Arthralgia/synovitis
🔹 Bone pain (tibia & femur classic)
🔹 Digital clubbing
🔹 X-ray: periostitis / tram lines
🔹 Always image the chest
Till here it’s easy twist is…
Why we did chest xray and ct thorax …
⚠️ New-onset HOA = think malignancy until proven otherwise
Key pearl 💡
📊 new onset means secondary HOA can be due to an underlying malignancy
📍 Most commonly lung cancer (NSCLC)..
Take-home
Rarely Joint pain may be the first sign of cancer.
Always 👀 beyond joints…
Older Child, preadolescent, unable to even walk in the house, so severely cyanotic....
...so sad to see these kids in OPD day after day ...
...yes we are able to help out.
But they should have been detected and made to undergo surgery long time ago....
What do u think is the diagnosis. Even the ecg is classic.
@DrRajeshG1@nihar_nayak2
2025 was a landmark year for stroke neurology.
From the MeVO trials to news of AI-driven systems of care and Factor XIa inhibitors on the horizon, the landscape of vascular neurology has shifted.
Here's a month-by-month recap of the year! 🧵
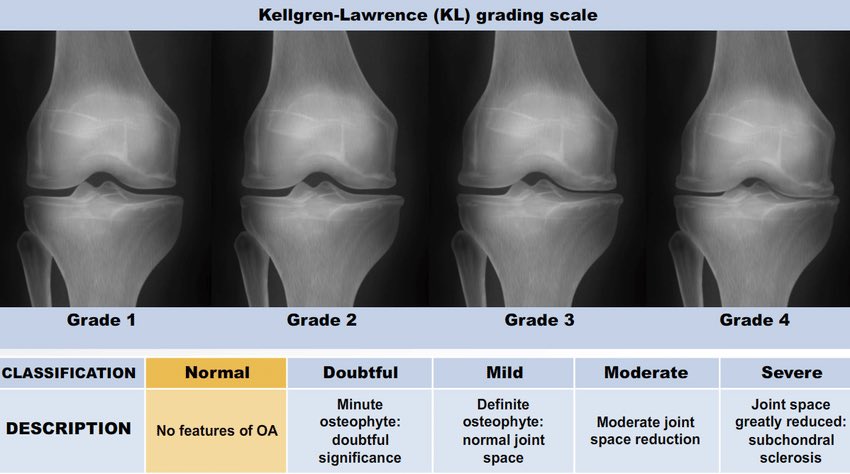
🦴📸 Kellgren–Lawrence Scale: OA at a Glance
Grading Osteoarthritis on X-ray (0–4)
Grade 0 – Normal 🦴✨
•Normal joint
•No OA changes
Grade 1 – Doubtful OA ❓🦴
•Possible tiny osteophytes
•Doubtful joint space narrowing
Grade 2 – Mild OA 🌱🦴
•Definite osteophytes
•Possible joint space narrowing
Grade 3 – Moderate OA ⚠️🦴
•Multiple osteophytes
•Definite joint space narrowing
•Subchondral sclerosis
•Possible bony deformity
Grade 4 – Severe OA 🔥🦴
•Large osteophytes
•Marked joint space narrowing
•Severe subchondral sclerosis
•Definite bony deformity
Key points
•Based only on radiographs (not symptoms)
•Widely used in clinical practice, trials, and epidemiology
•Pain severity may not correlate with KL grade
#RheumattDoc #MedTwitter #RheumTwitter #rheumatology @DrAkhilX @IhabFathiSulima@CelestinoGutirr@DurgaPrasannaM1
Palindromic rheumatism is fascinating—best viewed as a two-axis overlap (autoimmunity + autoinflammatory ‘attack’ biology).
Ref: doi:10.1038/s41584-019-0308-5
How often do you encounter this autoinflammatory-leaning presentations ? @DurgaPrasannaM1@sarath_rheum@IlliasulK@Rheumat_Aravind