I’m so excited. My secret (not so secret) observational experiment is about to begin.
This is a once in a lifetime opportunity for wastewater surveillance.
FIFA World cup.
1/
@SecureBio
https://t.co/3Yi9LFwNz2
Hiroshima University studied 6.2 million matched people in Japan.
COVID was linked to 4.14 times higher TB treatment risk, rising to 14.7 with prior TB.
This points to possible reactivation, not proof of cause.
https://t.co/xF2Vh3rZGk
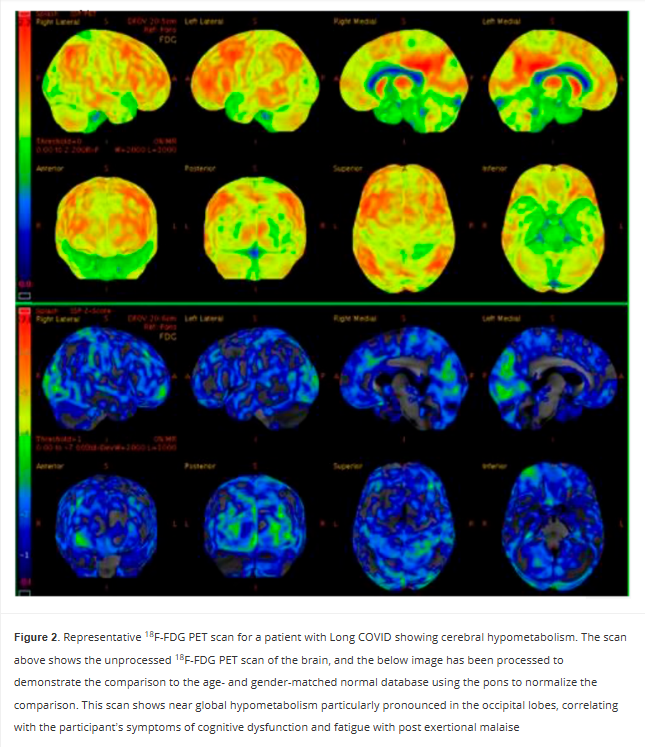
Persistent Cerebral 18-FDG PET Changes in Patients With Long COVID Presenting With Fatigue and Post Exertional Malaise
🚨We already knew Long COVID brain damage could last 6 months.
Now this new PET scan study proves it’s still there at 2 YEARS and counting.
Hypometabolism hits the left sensorimotor cortex (movement + body sense), left superior parietal (spatial awareness + attention), and bilateral visual cortex (raw sight processing).
This is NOT just “tired.”
This is a broken sensory-motor command center.
Is this the start of a lifelong neurological disease?
➡️Mayo Clinic observational cohort study of 40 Long COVID patients (70% female, median age 53) from a specialized clinic who underwent brain 18F-FDG PET-CT scans 17–149 weeks (median 62 weeks) after SarsCoV2 infection,
➡️73% had predominant fatigue with post-exertional malaise (PEM),
➡️This group showed statistically significant cerebral hypometabolism vs. non-PEM patients in the left sensorimotor cortex (p=0.0253), left superior parietal cortex (p=0.0276), and bilateral primary visual cortex (p=0.0096 and 0.0016),
➡️Abnormalities persisted already up to ~2 years post-infection,
➡️Scans used pons-normalized Z-scores against age/gender-matched controls with common comorbidities included psychiatric, GI, and cardiovascular conditions,
➡️Caveat: No references to vaccination status and/or reinfections,
➡️Authors propose 18F-FDG PET-CT as a potential diagnostic and therapeutic biomarker for the fatigue/PEM phenotype of Long COVID.
‼️So, AGAIN, Long COVID fatigue and PEM have a demonstrable, persistent neurological signature! Cerebral hypometabolism, still detectable on PET scans up to two years later and hits the left sensorimotor cortex (movement + body sense), left superior parietal cortex (spatial awareness + attention), and bilateral primary visual cortex (raw sight processing).
This isn’t just “tired.”
It’s a broken sensory-motor command center.
😡Study proves LC is biologically real, not psychosomatic or any other stupid FND diagnosis.
Without urgent validation of this biomarker and targeted therapies, patients will continue to be dismissed despite objective brain damage!
#AvoidSars2 #AvoidReinfections #BrainDamage
https://t.co/OfoOlgDyt0
🧵"What we know (and don't) about Covid-19's effect on the immune system."
1. Lasting impact
2. This looks like...
3. 5-20%
Source: https://t.co/2Y48VsLvWR
Beyond brain fog: viral proteins as convergent drivers of neuroinflammation and proteinopathy
🚨“COVID-19 never really leaves your brain.”
New science review proposes SARSCoV2 viral proteins stay behind as long-lived toxins, triggering chronic neuroinflammation and planting the seeds of Alzheimer’s and Parkinson’s, even after mild infection.
This very interesting and eye-catching GERMAN review reframes post-viral neurological syndromes( L0ngC0vid) as driven by persistent viral proteins acting as long-term toxins ("protein-as-pathogen" model), not just the active infection!
➡️Core mechanisms:
- SARSCoV2 Spike and OTHER viral proteins activate glial TLR4/TLR2 receptors, triggering chronic neuroinflammatory cascades via NLRP3 inflammasome,
- They also disrupt autophagy, allowing toxic protein aggregates (tau, amyloid-beta, α-synuclein) to accumulate and seed neurodegeneration,
➡️SARSCoV2 specific evidence:
- Animal studies show Spike protein alone (without live virus) induces TLR4-mediated cognitive deficits, memory impairment, synaptic loss, and sustained neuroinflammation, recapitulating post-COVID syndrome,
- Spike binds α-synuclein, accelerating Parkinson-like clumps,
➡️Human data evidence:
- Millions experience "brain fog,"
- Post-COVID patients exhibit measurable brain damage: cortical thinning, hippocampal iron accumulation, and biomarkers of ongoing neuronal injury,
➡️Broader risks:
- Even mild infections leave lingering proteins that promote Alzheimer’s and Parkinson’s-like pathology via shared pathways,
- Same pathways seen in influenza, dengue, West Nile etc,
- Mild infection = no protection,
‼️So, according to this review, the “protein-as-pathogen” model makes it crystal clear: every new SARSCoV2 infection (even mild or asymptomatic) deposits more of these long-lived toxic viral proteins into the brain. They don’t fully clear. They accumulate.
Each reinfection reloads the TLR4/TLR2 → NLRP3 inflammasome trigger and further collapses autophagy, speeding up the tau/amyloid/α-synuclein proteinopathy and neurodegeneration.
SARS-CoV-2 does not just infect.
It weaponizes its own proteins as long-lived intracellular saboteurs.
Millions are probably already carrying this hidden payload.
This is not brain fog.
This is a silent, population-scale reprogramming of human brains toward dementia-like decline.
The long-term neurological cost will probably dwarf the acute pandemic itself!
#AvoidSars2 #AvoidReinfections
https://t.co/x0oxacaNwl
Rates of infection with other pathogens after a +ve #COVID test versus a neg test - more brilliant work from @zalaly and team. COVID causes immune dysregulation and ⬆️risk of other infections. https://t.co/yIZ9LvD2NF
Pediatric Post-Acute Sequelae of SARS-CoV-2 Infection in Taiwan: Insights from the DISCOVER Cohort
🚨We’ve called for caution and we’ll do it again!! #OurChildren#Omicron
Even MILD paediatric COVID isn’t harmless.
➡️INTERESTING new Taiwan DISCOVER cohort (n≈500 kids, mean age7.6ys, post-2022 Omicron):
1. High burden of persistent multisystem symptoms:
- Even though acute COVID-19 was predominantly mild, a substantial proportion of children developed post-acute sequelae of SARSCoV2 (PASC/long COVID) lasting >4 weeks,
- The most common symptoms were fatigue, cough, chest pain, and other somatic complaints,
- Neuropsychiatric issues (sleep disturbances, brain fog, anxiety/depression) affected 5–15% of cases, particularly adolescents, and correlated with reduced quality of life,
2. Subclinical organ dysfunction frequently missed by routine tests:
- Impulse oscillometry detected abnormalities in 74.6% of assessed children (mainly small-airway dysfunction in 62.9%), strongly linked to respiratory symptoms,
- ‼️Conventional spirometry was often normal,
- ‼️AI-enhanced echocardiography (ResNet-50 model, 96.6% accuracy) unmasked subtle cardiac changes not visible on standard echo,
3. Immune-driven mechanism:
- Symptom severity tracked with elevated anti-nucleocapsid IgG titers and a low-grade “cytokine simmer” (elevated IL-2, IL-21, MIP-1α) plus T-cell exhaustion markers (PD-1/PD-L1 correlation),
- No evidence for viral persistence,
4. Vaccination modifies disease course:
- ‼️Fully vaccinated children had significantly lower odds of gastrointestinal sequelae (abdominal pain AOR 0.49; diarrhoea AOR 0.37) and better-preserved pulmonary function (improved impulse-oscillometry parameters),
5. Vitamin D supplementation may show early promise:
- A small single-center RCT (n=33) found 2,000 IU/day for 6 months significantly reduced overall symptom burden (CSSI-24 score), lowered pro-inflammatory cytokines, and favourably altered immune checkpoints and the microbiome, especially in children with vitamin D deficiency plus VDR risk genotypes,
6. Additional risks identified:
-Older age and greater acute-infection severity predicted worse PASC,
- ‼️The cohort also showed an elevated hazard of new-onset allergic diseases (asthma, rhinitis, dermatitis) post-infection.
‼️So, AGAIN, even mild pediatric SARS-CoV-2 infections can trigger long-lasting multisystem damage and impaired quality of life. Persistent symptoms in children must never be dismissed as “just recovery/getting over it” but need prompt specialist evaluation and intervention!
Dammm it….protect our children and don’t relax after at first sight “normal” tests!
#CleanAir #AvoidSars2 #AvoidReinfections
https://t.co/pqKmZr3yc5
IKEA sells a $30 air quality monitor now. Amazon has an affordable monitor too. Sensors are shrinking fast.
Issue 02 of The Air Quality Index looks at what's driving air quality monitoring into the mainstream. New devices from big-name brands, miniaturisation (including the Bosch BMV080, a PM sensor roughly the size of a fingernail), and smarter ways to visualise pollution data.
https://t.co/rfxuHHT4F8
Incredible speech delivered by Baroness Linforth in the House of Lords today calling for clean indoor air in schools.
“It would cost less than a tenner per child per year to provide pupils and staff with clean air - about the same cost as a coffee and a cake.”
☕️🧁
People who tested positive for #COVID have a higher risk of being diagnosed with other infections in the following months. This has been shown for years and hundreds of publications in the topic. Covid has an impact on the immune system we still don't fully understand.
A New Phase of SARS-CoV-2 Evolution?
The evolution of SARS-CoV-2 has followed a familiar pattern: new variants emerged, spread rapidly across the globe, and replaced their predecessors - triggering successive waves of infection.
This pattern may now be changing - see our manuscript below. Here is the evidence - and what it suggests.
BA.3.2 is different
Instead of being replaced, variants that were dominant in the second half of 2025 continue to circulate. At the same time, a new saltation variant - BA.3.2 (“Cicada”) - is spreading globally but more slowly and unevenly across regions.
👉 It can spread alongside other variants
👉 It dominates in some regions, but not others
👉 Its global spread is gradual, not explosive
BA.3.2 preferentially targets children
BA.3.2, unlike other variants, preferentially targets children and its spread can be associated with rising case numbers among children.
What does this mean?
One might speculate that:
➡️No single variant may dominate worldwide in the future.
➡️The time of pandemic waves of infection may come to an end. Instead, COVID-19 may become a more regionally variable, endemic disease.
Which questions remain open?
Why does BA.3.2 preferentially target children? The particular antibody profile in this age group is my best guess, but other possibilities exist and have been discussed on this platform.
Is BA.3.2 more pathogenic in children than other variants?
Does the deletion of accessory ORFs in BA.3.2 result in preferential infection of the upper respiratory tract, where the interferon system is likely less potent relative to the lower respiratory tract?
Do we need a bi- or even multivalent vaccine for the next COVID-19 season, covering BA.3.2 and other variants?
Will BA.3.2 acquire mutations that increase transmissibility?
Reference
Does BA.3.2 epidemiology imply a change in SARS-CoV-2 evolution? - The Lancet Infectious Diseases https://t.co/2ISgELZnsF
@1goodtern Unfortunately we've had a breakbreakdown in our protocols, either my earloop mask didn't cut it in what didn't appear to be a high risk environment or I caught it talking to someone outside. Very annoying since if wasn't a cold, flu or rsv that I caught but covid-19.
We’re in year 7 of COVID, and a lot has changed. We now understand far more about its long-term impact on the body and how infections can build over time. If you’ve been rethinking your approach to protection, you’re not alone, and it’s not too late to start again.
Read more and explore practical, science-based guidance here: https://t.co/FCYlUnf4XN
#COVID19 #COVID #SARSCOV2 #LongCOVID #CovidIsNotOver #COVIDAwareness #LongCOVIDAwareness
Holy shit, after 5 years Health Canada finally put out engineering guidelines recommending people wear N95s, clean indoor air to reduce viral load, and admitted COVID is airborne. Based
https://t.co/TjWPnP2MPX
For anyone wanting a deep-dive into the regulation of indoor air quality in Australia, the recent NSW Parliament enquiry into Clean Indoor Air offers a treasure-trove of great information about the present sorry situation and possible ways forward.
A recurrent theme of the inquiry has been that there is little we can do about poorly ventilated public buildings because there are no standards to enforce.
It’s true that the absence of specific standards for indoor air quality has long been used as an excuse for the indifference to effective ventilation. But I believe that new regulatory frameworks and codes of practice make it clear that even without unambiguous standards, safe indoor air is a non-negotiable legal obligation and the consequences for non-compliance reach all the way to individual principals, executives, and clinicians. Full details here: https://t.co/YN0cE4BQrJ
Harvard researchers put 24 office workers in the same room for 6 days.
They changed one thing about the air. The workers didn't know.
Then they tested their brains.
Cognitive scores doubled.
Here's what the air you're breathing right now is doing to your brain:
For Aussie Christians concerned with the air they breathe in Churches and groups, I have a Facebook group or we can talk here. A challenge for Christian communities https://t.co/ODkTEBOEED #christian#australia#longcovid#me#cleanair#saferair