The term "VIP patient" further perpetuates existing disparities in healthcare. Let's work to treat all of our patients like the very important people that they are. 🤝🏾👩🏻⚕️⚕️⚖️🩺🏥
#HealthForAll#HealthEquity#HealthIsWealth
7yr CROWN update of 1L lorlatinib
55% progression-free at 7 YEARS.
Median PFS STILL not reached.
In metastatic solid tumors, this is essentially unheard of. Let that sink in.
And hopefully, one day, this becomes the standard (or even better) for ALL metastatic cancers.#ASCO26
a standing ovation for daraxonrasib at asco. over 40k oncologists, entrepreneurs, investors, and patient advocates together celebrating revmed's breakthru in the fight against pancreatic cancer. u never forget these moments. it's what innovation is all about.
🏛️ Presented today at the EAS 2026 Congress in Athens.
🤩 A fascinating case of double-hit genetic dyslipidemia, combining severe lifelong exposure to apoB-containing lipoproteins and extremely elevated Lp(a), resulting in diffuse polyvascular atherosclerotic disease.
🔹 LDL-C: 272 mg/dL (untreated)
🔹 ApoB: 198 mg/dL
🔹 Lp(a): 766 nmol/L
🔹 Coronary, carotid, subclavian, peripheral, and calcific aortic valve disease
This case highlights a key concept:
➡️ Atherosclerotic risk is not only about current LDL-C levels—it is the consequence of cumulative lifelong exposure to atherogenic lipoproteins.
☝️ As we await dedicated Lp(a)-lowering therapies, early detection, cascade screening, and aggressive apoB reduction remain essential.
👉 The case raises several important questions:
🔎 Diagnostic Challenges
• How much of the phenotype is driven by familial hypercholesterolemia versus extreme Lp(a)?
• Is severe calcific aortic stenosis simply another manifestation of lifelong lipid exposure, or does it represent a distinct disease process?
• How should we quantify cumulative apoB burden in routine clinical practice?
💊 Therapeutic Challenges
• LDL-C remains above guideline targets despite intensive lipid-lowering therapy.
• PCSK9-targeted therapies are not universally accessible.
• No approved Lp(a)-specific therapies are currently available.
• Lipoprotein apheresis is often unavailable or impractical.
👨👩👧👦 Management Challenges
• What is the optimal antithrombotic strategy in a patient with extensive polyvascular disease and chronic kidney disease?
• How should cascade screening be implemented when both FH and markedly elevated Lp(a) are suspected?
@society_eas@nationallipid@natinardelli_
The Unpaid Infrastructure of Cardiovascular Science @JACCJournals
🫀 Behind nearly every advance in cardiology lies a network of clinicians voluntarily assessing evidence & refining scientific work before it reaches the clinical community
😩 Professional obligation 🆚 Unpaid Labour
How should we move forward when publications are billion dollar businesses? #CardioTwitter
🔗 https://t.co/2Y3tVSi9qt
Something just changed in medicine that most physicians haven't noticed yet.
As of early 2026, a practicing doctor can prototype a working clinical tool — solo, in a weekend. No CS degree. No team. No budget.
I gave Cardiology Grand Rounds @UCSDHealth on the emerging role of the physician-developer today.
Here's what changed, and why the next decade of medical software gets built by us 🧵
Can Earlier LDL-C Lowering Change the Trajectory of Cardiovascular Disease?
https://t.co/eVDmXuZrsT
A thought-provoking simultaneous publication new @ProfKausikRay published in @AJPCardio presented at @society_eas yesterday revisits one of the central questions in prevention:
Are we intervening too late?
Using data from 17 randomized lipid-lowering trials involving more than 105,000 participants, Karungi and colleagues examined how the relative cardiovascular benefit of LDL-C lowering changes across different baseline risk levels.
The findings are intriguing.
1. Contrary to the traditional assumption that lower-risk individuals derive only modest benefit, the investigators observed that relative risk reduction per 1 mmol/L LDL-C lowering was actually greater in lower-risk primary prevention populations.
2. In trial populations with annualized event rates around 1% per year, each mmol/L LDL-C reduction was associated with roughly a 36% relative reduction in events, compared with approximately 13% in populations with event rates near 3% per year.
The paper bring to light an important conceptual framework.
1. As atherosclerosis advances, larger LDL-C reductions may be required to achieve the same proportional benefit.
2. In lower-risk and presumably earlier-stage disease, even modest LDL-C reductions may yield meaningful relative risk reduction.
This shifts the discussion from simply “who is high risk today?” toward a broader life-course perspective:
1. Are we waiting long before intervening?
2. Can modest but earlier LDL-C lowering alter cumulative vascular exposure before disease becomes biologically irreversible?
3. Should early primary prevention become more central to our prevention frameworks?
I think the implications extend beyond statins alone. For the future we need to think around long-duration therapies, , AI-guided risk prediction, imaging-guided prevention, and cumulative LDL exposure increasingly points toward a future where prevention may begin earlier, become more personalized, and focus more on preserving vascular health before advanced disease develops.
@ASPCardio@rblument1
“The higher the risk, the greater the LDL-C reduction required.”
Excellent presentation by Kausik Ray at the NLA–EAS Joint Session on Primary Prevention.
A key message: while the relative benefit of LDL-C lowering may attenuate as baseline risk increases, achieving meaningful absolute risk reduction requires progressively larger LDL-C reductions.
🔹 Earlier intervention
🔹 Lower LDL-C levels
🔹 Combination therapy when needed
🔹 Better implementation of guideline recommendations
In lipid management, intensity should match risk.
@society_eas@ProfKausikRay@nationallipid
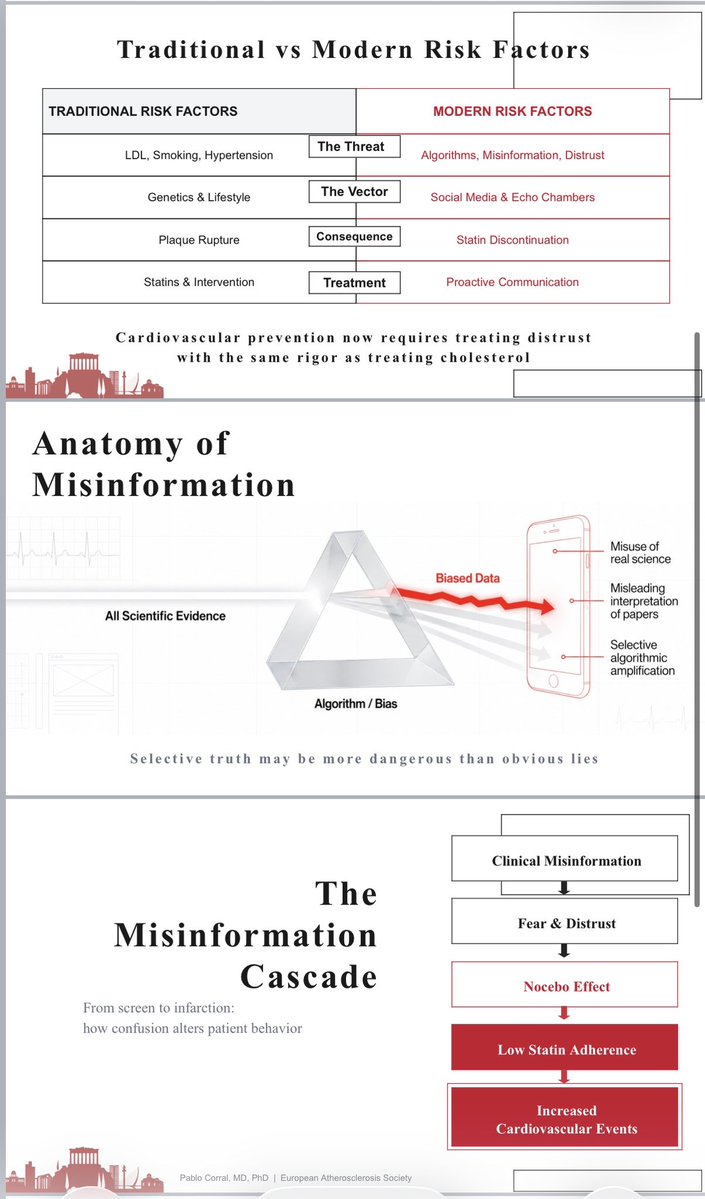
❤️ Safe Hearts Require Safe ℹ️
🙏🏻 Honored to share my perspective at #EAS2026 on one of the most underestimated cardiovascular risk factors of our time: misinformation.
👉Today, cardiovascular prevention is no longer limited to controlling LDL-C, blood pressure, or smoking. We must also address the growing impact of distrust, misinformation, and algorithm-driven health content on patient behavior.
Key messages:
🔹 Virality is not validity
🔹 Selective truths can be as harmful as outright falsehoods
🔹 Poor information fuels fear, nocebo effects, and treatment discontinuation
🔹 Scientific societies must proactively engage in the digital space
🔹 Safe hearts require safe information
☝️The future of prevention depends not only on developing better therapies, but also on ensuring that evidence-based medicine reaches patients clearly, accurately, and effectively.
@society_eas@BNordestgaard@ProfKausikRay@nationallipid@DrMarthaGulati@LondonoMd@Drlipid@DrMauinforma
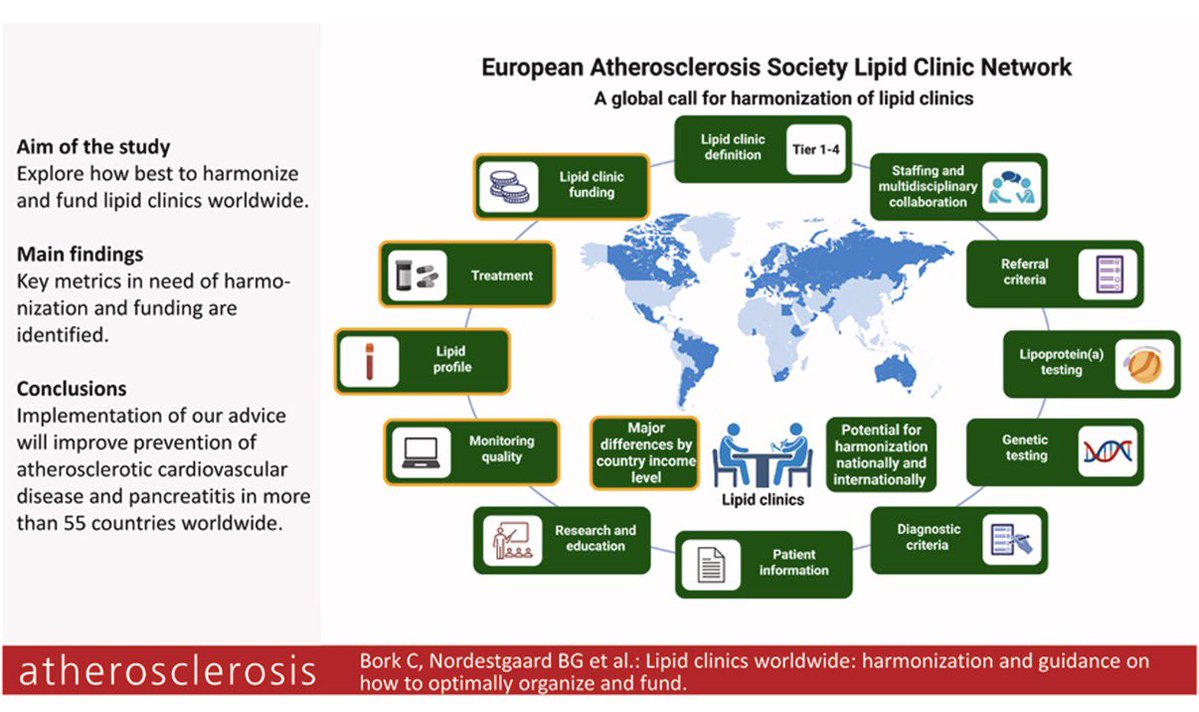
👉Just published in Atherosclerosis — a true milestone for the global lipid community. 🌍🫀
☝️The new EAS Consensus Statement on lipid clinics brings together experts from 55 countries and more than 500 lipid clinics to provide practical guidance on harmonization, organization, staffing, education, patient pathways, and funding of lipid services worldwide.
📌 Why it matters:
• Establishes a global framework for lipid clinic development
• Promotes equitable access to high-quality lipid care
• Supports earlier diagnosis and better management of inherited and complex lipid disorders
• Strengthens prevention of ASCVD on a worldwide scale
• Highlights the importance of education, registries, and multidisciplinary care
☝️A fantastic initiative by the European Atherosclerosis Society Lipid Clinic Network and all contributing authors. Proud to have participated in this important international effort.
☝️A must-read for anyone involved in preventive cardiology, lipidology, cardiovascular prevention, and healthcare policy.
🔓🔗 https://t.co/TowmAM6FZH
@society_eas@ATHjournal@BNordestgaard@ProfKausikRay
🚨 New Commentary Published: Advancing Awareness & Testing for Lipoprotein(a) (Lp[a])
The American Heart Association’s new Lipoprotein(a) Discovery Project highlights a national effort to improve awareness, screening, and care pathways for patients with elevated Lp(a) — a genetically inherited and underrecognized cardiovascular risk factor linked to ASCVD, stroke, and aortic stenosis.
With the 2026 ACC/AHA Dyslipidemia Guideline now recommending at least one lifetime Lp(a) measurement for every adult, this initiative aims to expand testing, improve clinical workflows, and strengthen patient-centered cardiovascular prevention strategies.
📖 Read the commentary here: https://t.co/J4We9mWYCh
#LipoproteinA #LpA #PreventiveCardiology #Cardiology #ASCVD #HeartHealth #AHA #LipidManagement #CardiovascularDisease
New research highlights the powerful role nutrition can play in early hypertension management. A higher adherence to the DASH eating pattern may help delay or reduce the need for medication initiation in adults with stage 1 hypertension.
The findings reinforce what many clinicians already see in practice: lifestyle interventions aren’t just complementary—they can be foundational.
The DASH diet emphasizes:
🥗 Fruits & vegetables
🌾 Whole grains
🥛 Low-fat dairy
🐟 Lean proteins
🧂 Reduced sodium intake
As rates of hypertension continue to rise, evidence-based nutrition strategies could have a major impact on long-term cardiovascular health and healthcare costs.
Read it here: https://t.co/JGTKiGbamj
🙌 Our last manuscript is out.
👉“Safety of Very Low LDL-Cholesterol:
Ten Common Concerns, Misconceptions, and Evidence-Based Clarifications”
📍Very low LDL-C levels continue to generate debate, fear, and misinformation in clinical practice.
📍In this review, we critically examined 10 of the most frequent concerns related to intensive LDL-C lowering:
— Cognitive decline
— Hemorrhagic stroke
— Cancer
— Cataracts
— Hormonal dysfunction
— Diabetes risk
— Muscle symptoms
— Older adults
— Sex differences
— Overall cardiovascular benefit
📍The key message is clear:
RCTs, meta-analyses, and genetic evidence consistently support the safety profile of very low achieved LDL-C levels in appropriately selected high-risk patients.
📍Some adverse effects are real — particularly statin-associated dysglycemia and muscle symptoms — but their absolute risk is generally modest compared with the magnitude of ASCVD risk reduction.
📍Therapeutic inertia and misinformation remain major barriers in preventive cardiology. Evidence-based communication matters.
📍Lower LDL-C. Earlier. Longer. Safer than many still believe.
☝️Proud to collaborate with outstanding colleagues from Latin America, Europe, and beyond in this international effort.
🔗 https://t.co/zEMcECn9El
@society_eas@ATHjournal
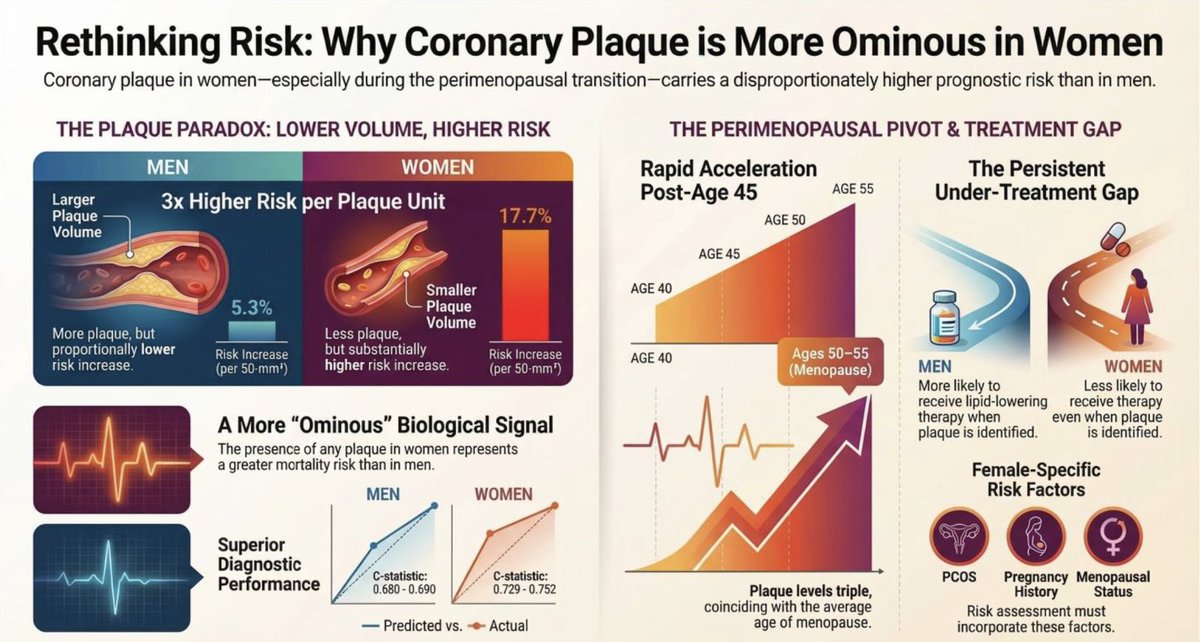
Coronary plaque in younger women may carry a far greater prognostic signal than equivalent plaque in men.
In our editorial in the Am Journal of Preventive Cardiology (https://t.co/s5vcvNHkSp), we discuss why sex-specific interpretation of CCTA findings is essential—and why even “mild” plaque in women should prompt aggressive prevention efforts.
#CardioTwitter #CCTA #WomensHeartHealth
This is my favorite study of the year.
What a waste of money. But keep telling physicians to see more patients every hour. Because that is working so well….
We are deeply saddened to have lost our founding chairman and the father of modern academic cardiology, Dr. Eugene Braunwald, who founded the TIMI Study Group in 1984, and with that vision profoundly shaped the practice of cardiovascular medicine across the world.
































![AJPCardio's tweet photo. 🚨 New Commentary Published: Advancing Awareness & Testing for Lipoprotein(a) (Lp[a])
The American Heart Association’s new Lipoprotein(a) Discovery Project highlights a national effort to improve awareness, screening, and care pathways for patients with elevated Lp(a) — a genetically inherited and underrecognized cardiovascular risk factor linked to ASCVD, stroke, and aortic stenosis.
With the 2026 ACC/AHA Dyslipidemia Guideline now recommending at least one lifetime Lp(a) measurement for every adult, this initiative aims to expand testing, improve clinical workflows, and strengthen patient-centered cardiovascular prevention strategies.
📖 Read the commentary here: https://t.co/J4We9mWYCh
#LipoproteinA #LpA #PreventiveCardiology #Cardiology #ASCVD #HeartHealth #AHA #LipidManagement #CardiovascularDisease](https://pbs.twimg.com/media/HISkkgVWQAA81S8.jpg)