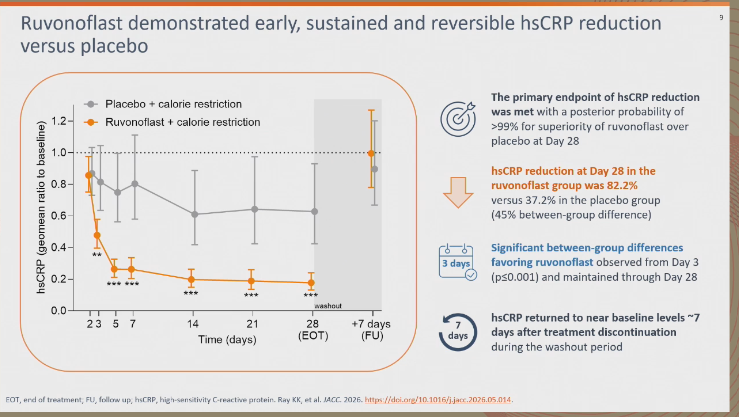
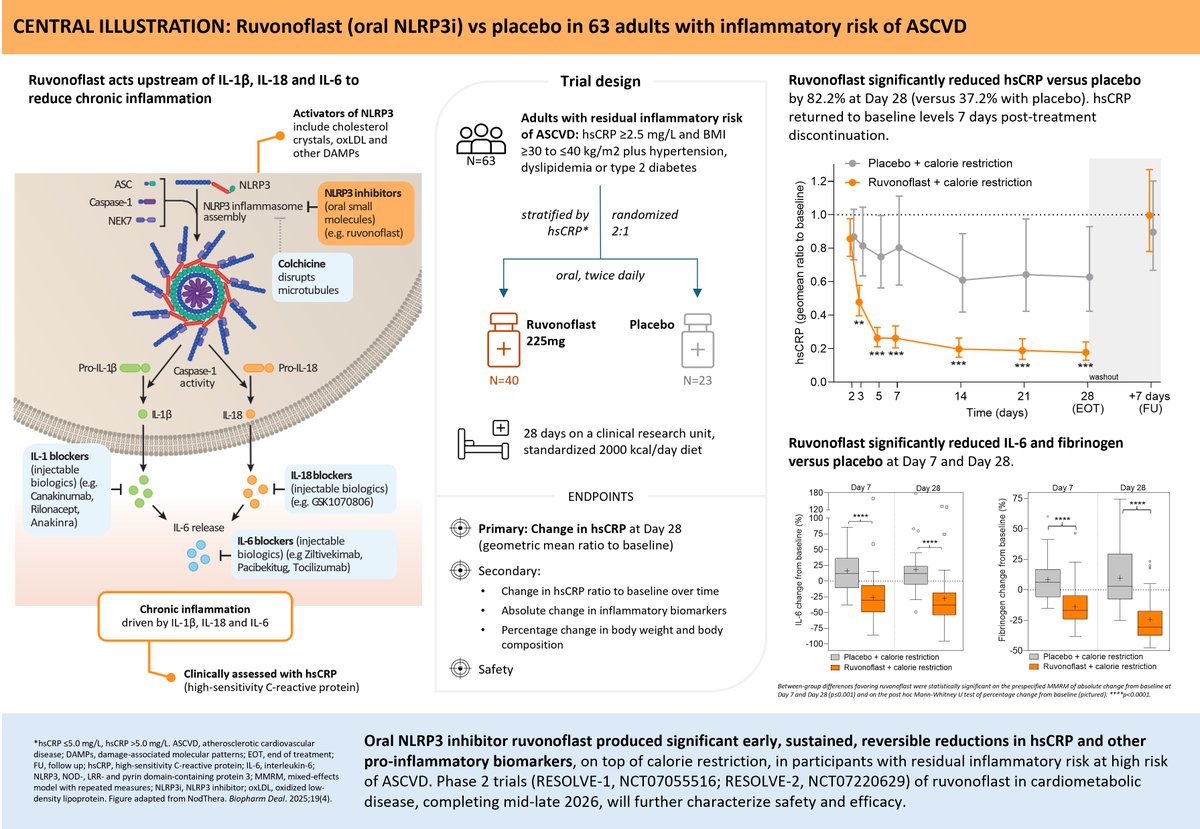
Ruvonoflast, an oral NLRP3 inhibitor, provides early, sustained, & reversible reductions in #hsCRP & significantly lowers inflammatory biomarkers IL-6 & fibrinogen in cardiometabolic patients with elevated #ASCVD risk https://t.co/HAQsOzox8i
#EASCongress2026#JACC@ProfKausikRay
Can Earlier LDL-C Lowering Change the Trajectory of Cardiovascular Disease?
https://t.co/eVDmXuZrsT
A thought-provoking simultaneous publication new @ProfKausikRay published in @AJPCardio presented at @society_eas yesterday revisits one of the central questions in prevention:
Are we intervening too late?
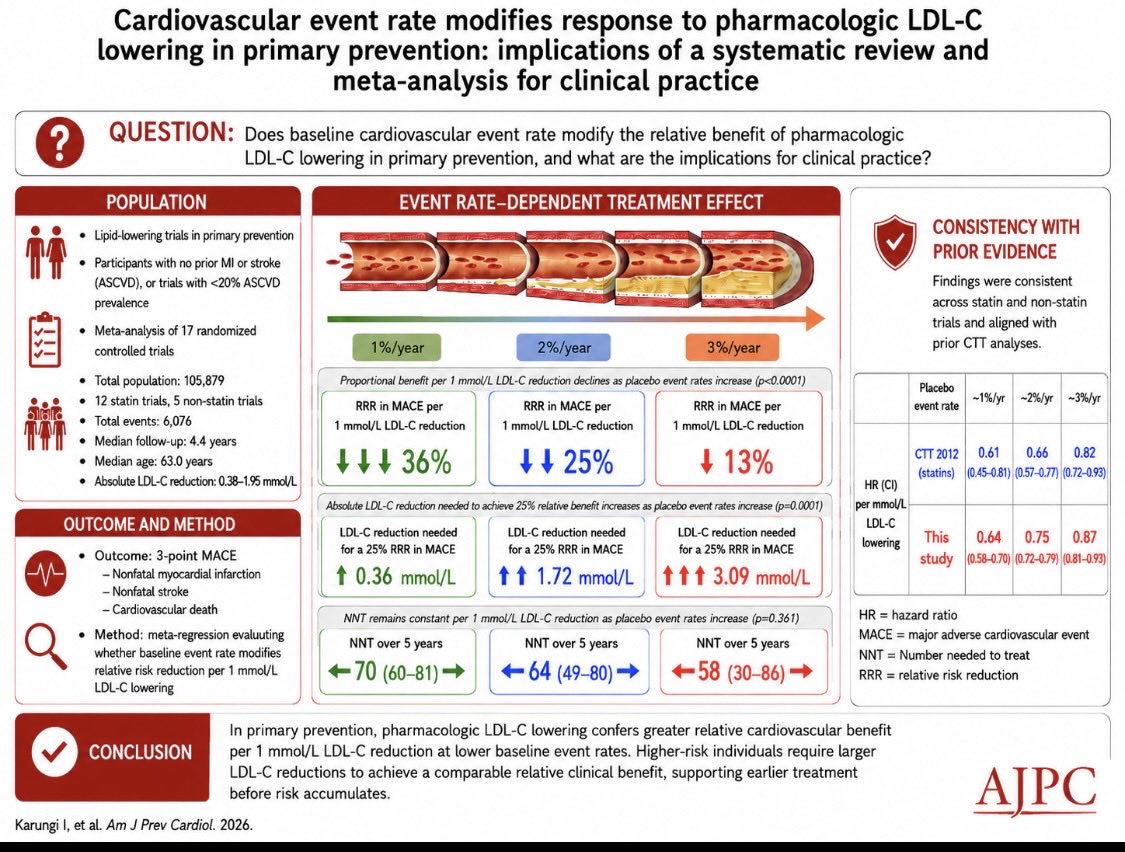
Using data from 17 randomized lipid-lowering trials involving more than 105,000 participants, Karungi and colleagues examined how the relative cardiovascular benefit of LDL-C lowering changes across different baseline risk levels.
The findings are intriguing.
1. Contrary to the traditional assumption that lower-risk individuals derive only modest benefit, the investigators observed that relative risk reduction per 1 mmol/L LDL-C lowering was actually greater in lower-risk primary prevention populations.
2. In trial populations with annualized event rates around 1% per year, each mmol/L LDL-C reduction was associated with roughly a 36% relative reduction in events, compared with approximately 13% in populations with event rates near 3% per year.
The paper bring to light an important conceptual framework.
1. As atherosclerosis advances, larger LDL-C reductions may be required to achieve the same proportional benefit.
2. In lower-risk and presumably earlier-stage disease, even modest LDL-C reductions may yield meaningful relative risk reduction.
This shifts the discussion from simply “who is high risk today?” toward a broader life-course perspective:
1. Are we waiting long before intervening?
2. Can modest but earlier LDL-C lowering alter cumulative vascular exposure before disease becomes biologically irreversible?
3. Should early primary prevention become more central to our prevention frameworks?
I think the implications extend beyond statins alone. For the future we need to think around long-duration therapies, , AI-guided risk prediction, imaging-guided prevention, and cumulative LDL exposure increasingly points toward a future where prevention may begin earlier, become more personalized, and focus more on preserving vascular health before advanced disease develops.
@ASPCardio@rblument1
An important extension of the accompanying paper is the editorial by @rblument1 and @AlexRazavi , which frames these findings through a simple but powerful analogy borrowed from Arnold Palmer: “Timing is everything in life and in golf.”
https://t.co/Yd6bOEgLRo
For decades, much of our prevention framework has focused on identifying individuals once short-term risk becomes sufficiently high.
What if we can address the cumulative exposure , then when we lower LDL-C may matter just as much as how much we lower it.
Importantly, the authors do not advocate indiscriminate pharmacotherapy.
Instead, they highlight a more personalized strategy integrating PREVENT risk estimation, inflammatory markers, lipoprotein(a), CKM risk factors, and importantly CAC imaging to identify those most likely to benefit from earlier intervention.
In many ways, the editorial captures an important philosophical shift. The future may not simply be about treating advanced disease more aggressively, but preserving vascular health before advanced atherosclerosis develops.
Timing, indeed, may be everything.
@ProfKausikRay@society_eas@ASPCardio
#EASCongress2026 A new actionable pathway is tested in a phase 1 study by @ProfKausikRay and collaborators. Rivonoplast, a potent inhibitor of NLRP3 inflamassome led to early and sustained reversible sCRP reduction compared to placebo. (Follow next tweet👇👇)
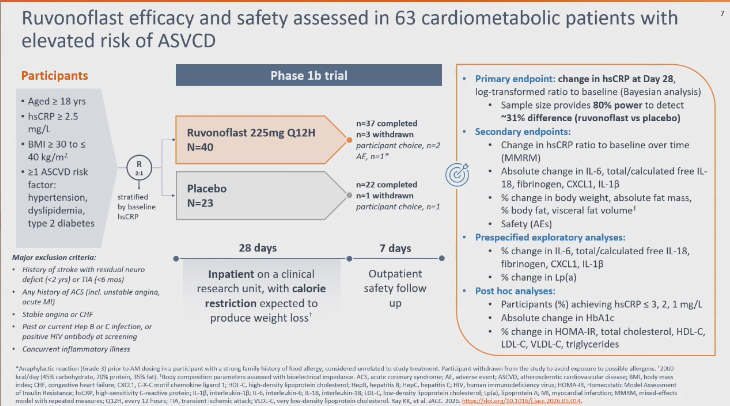
Thread #1 This afternoon, there will be an unmissable late-breaker presentation by @ProfKausikRay, at Aravanis Hall, exploring NLRP3 inflamassome inibition in humans with inflammatory residual risk for ASCVD, as depicted below (Read following tweet for additional information)
👉Current leadership and future leadership sharing the stage at #EAS2026.
A great moment to witness the strength of continuity within the European Atherosclerosis Society, with the current EAS President @BNordestgaard and the immediate Past President @ProfKausikRay leading discussions on the EAS Stage in Athens.
From global outreach initiatives to challenging lipid cases, this session highlights the collaborative spirit, scientific excellence, and international engagement that continue to drive the EAS mission forward.
@society_eas
A very important paper from @ProfKausikRay et al
Lower-risk 1y prevention populations derive greater relative benefits per 1mmol/L LDL-C lowering. higher-risk populations get less benefit per 1mmol/L LDL-C lowering & need greater absolute LDL reduction
https://t.co/wqN1IMcIYn
#EASCongress2026. A master class talk by @ProfKausikRay on combination drug therapy for lipid lowering. Highlighted concept of “time” and “just doing it” when approaching treatment of atherosclerosis. Start early and overcome clinical inertia.
“The higher the risk, the greater the LDL-C reduction required.”
Excellent presentation by Kausik Ray at the NLA–EAS Joint Session on Primary Prevention.
A key message: while the relative benefit of LDL-C lowering may attenuate as baseline risk increases, achieving meaningful absolute risk reduction requires progressively larger LDL-C reductions.
🔹 Earlier intervention
🔹 Lower LDL-C levels
🔹 Combination therapy when needed
🔹 Better implementation of guideline recommendations
In lipid management, intensity should match risk.
@society_eas@ProfKausikRay@nationallipid
Our paper EHJ. In ~ 3k Japanese pts ldl-c <55 mg/dl attenuated risk of MACE in those with high LPa. However residual risk still present hence lowering LPa is an unmet need. The risk goes up at 30mg/dl so lower than other groups
https://t.co/xFKiRaaBbB
Trial evidence from 17 trials in people without ASCVD including statins and non statins in 105 000 individuals about why you get a bigger benefit from starting prevention early . AJPC open access