A student asked: "If sore throats are caused by a virus or bacteria, how come sleeping under the fan or drinking cold water gives it?"
I am surprised most people are not aware of the answer to this.
Who runs the #PICU?
The Pediatric Intensivist.
Everyone else owns an organ…
we handle the situation
When things go south, #PedsICU connects the dots, with physiology, evidence& experience.
PICU is not just a unit. We r the calm in storm
Submit abstract https://t.co/pBzFtmR0wR
The real (and exciting) reason this paper caught my attention is its eloquent discussion of the RCT transportability problem.
The author argues that while some trials in critical care may be internally valid (thanks to randomization), their results cannot be reliably applied (transported) to future patients, other hospitals, or subsequent trials.
In the causality literature, transportability was rigorously treated by @yudapearl and @eliasbareinboim. But seeing it articulated so clearly in clinical discourse—“non-transportability means results from an RCT cannot reliably apply to your next patient”—had a real Christmas-came-early vibe.
The article argues that non-transportability arises because enrollment criteria lump together distinct diseases, such as viral and bacterial pneumonia.
The reported treatment effect is therefore a weighted average over a mixed-disease population. If the patient mix changes across hospitals or populations, the average treatment effect estimated by an RCT changes too.
True, randomization guarantees internal balance, but the findings remain unhelpful for real-world critical care. By averaging opposing biological responses, trials can mask how treatment might save a bacterial patient while harming a viral one.
Strong words. Takes guts.
How we use critical care ultrasonography in the management of cardiogenic shock: a strategic game of chess in intensive care
CCR Journal Watch - tracking the critical care literature daily
https://t.co/Sp06oA6IDG
Congratulations to Devika on securing first prize poster presentation in World ARDS meet Delhi!It's an achievement & acknowledgement of our collective effort of antivirals and immunomodulation therapy in Adenoviral ARDS @rakshay_shetty @bhat_chandrika@Manu_Delhi87@DrPavitraV
Join us for an electrifying Cytokine Storm Symposium!Dive into cutting-edge insights with Dr. Randy Cron as he unravels "Personalized Approaches to Treating Secondary CSS."
Don’t miss this chance to learn from a global expert! Register now!
https://t.co/phzz2Gvh9u
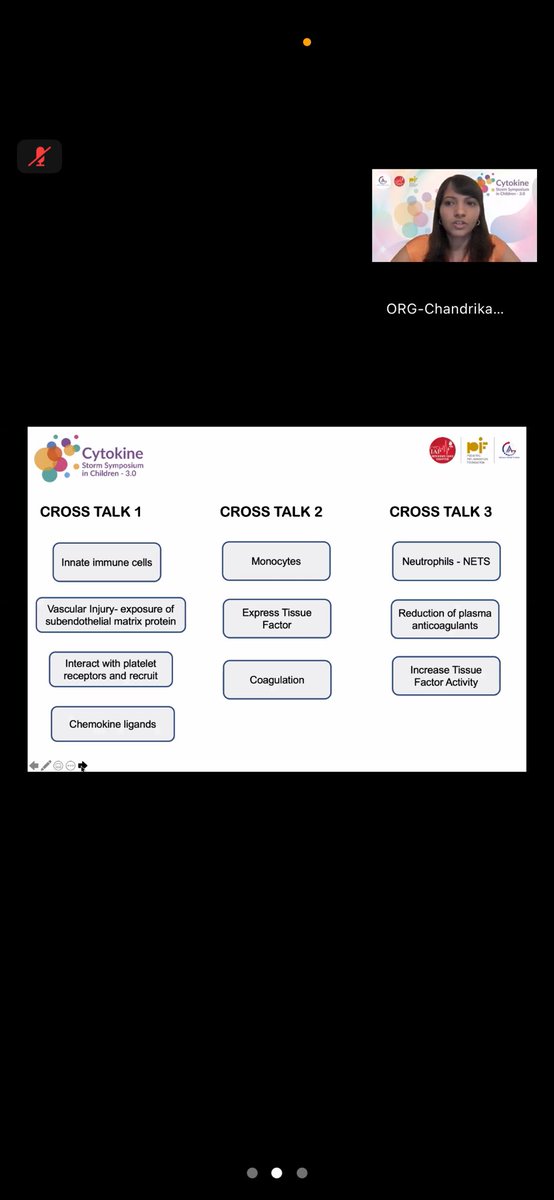
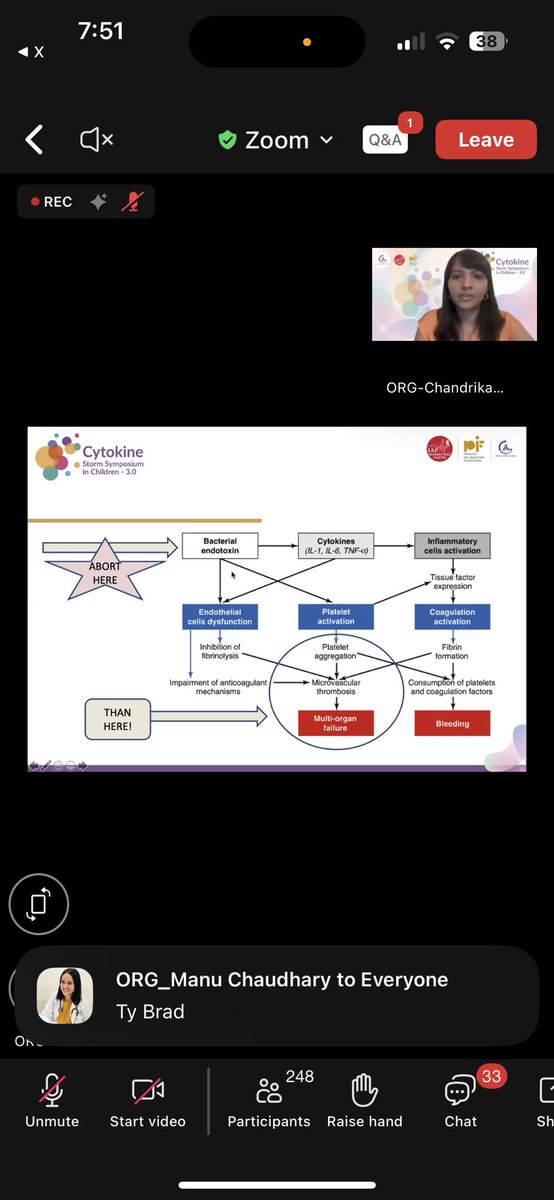
Cytokine Storm Symposium Alert! 🔬
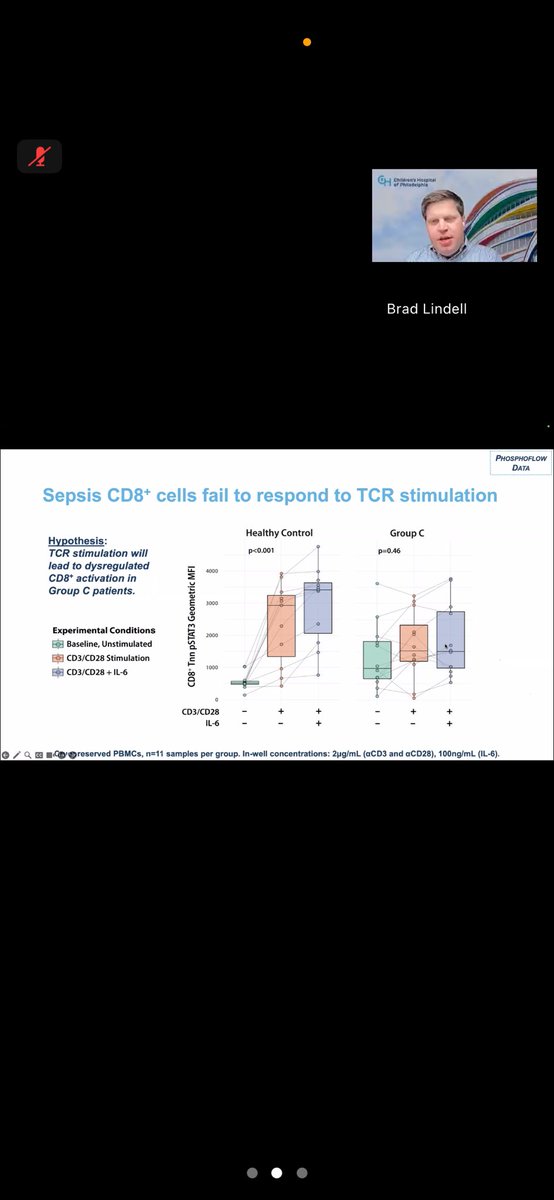
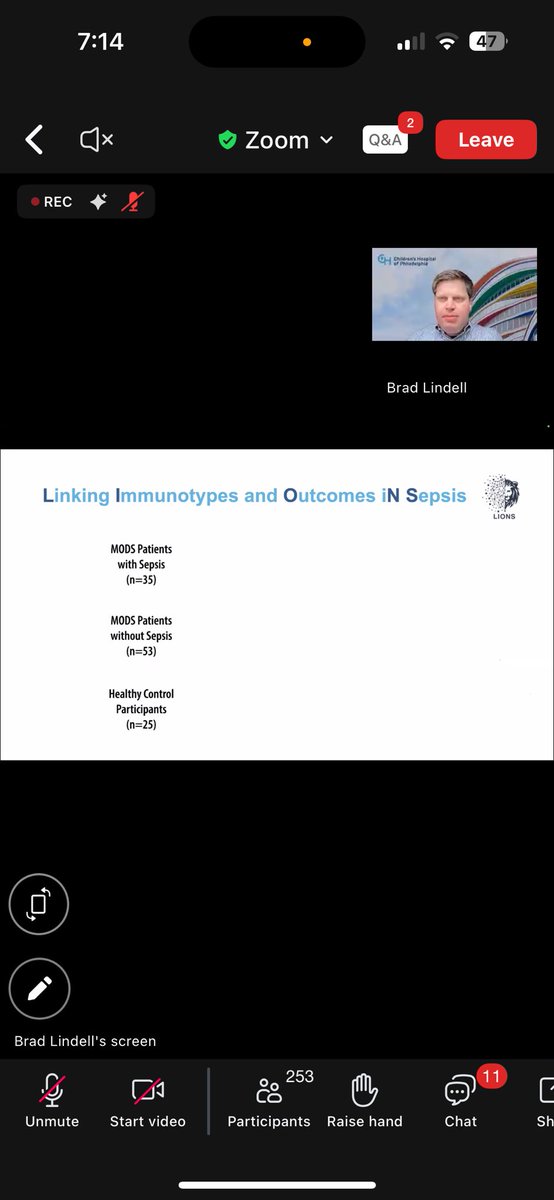
Join Dr. Joe Carcillo as he unravels the phenotypes of cytokine storm in sepsis Hyper Inflammatory chaos to immune paralysis! management strategies must adapt!!A must-attend for all !
#CytokineStorm#Sepsis#CriticalCare https://t.co/phzz2GvOZ2
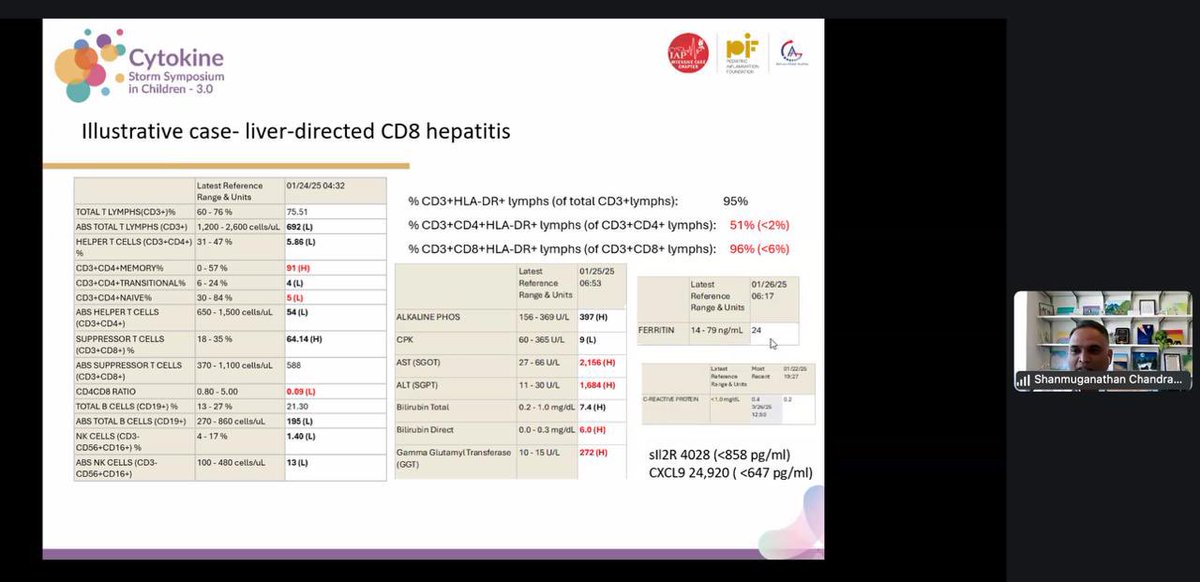
Speaker Spotlight!
Dr. Shanmuganathan Chandrakasan—immunology expert & Director of Immune Dysregulation at Emory—joins our #CytokineStorm symposium!
He'll expose how PIDs can masquerade as cytokine storms 🔥🧬
Don’t miss this eye-opening session!
https://t.co/phzz2Gvh9u
Get ready for a surge of knowledge! Our #CytokineStorm Symposium features a powerhouse lineup of expert faculty you won’t want to miss. Don’t wait—register now for cutting-edge insights and dynamic discussions!
https://t.co/phzz2Gvh9u
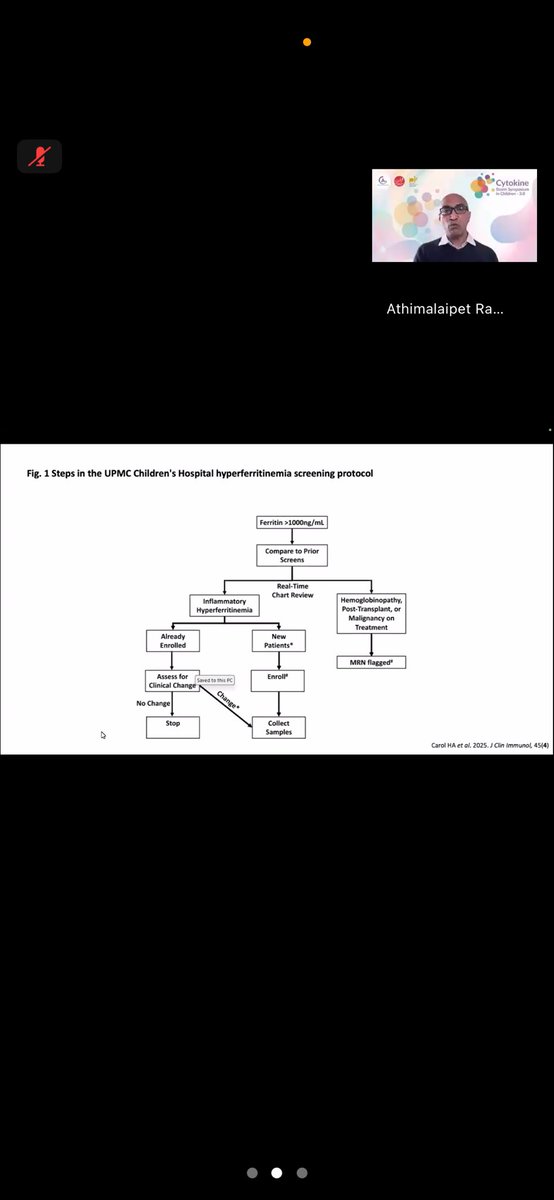
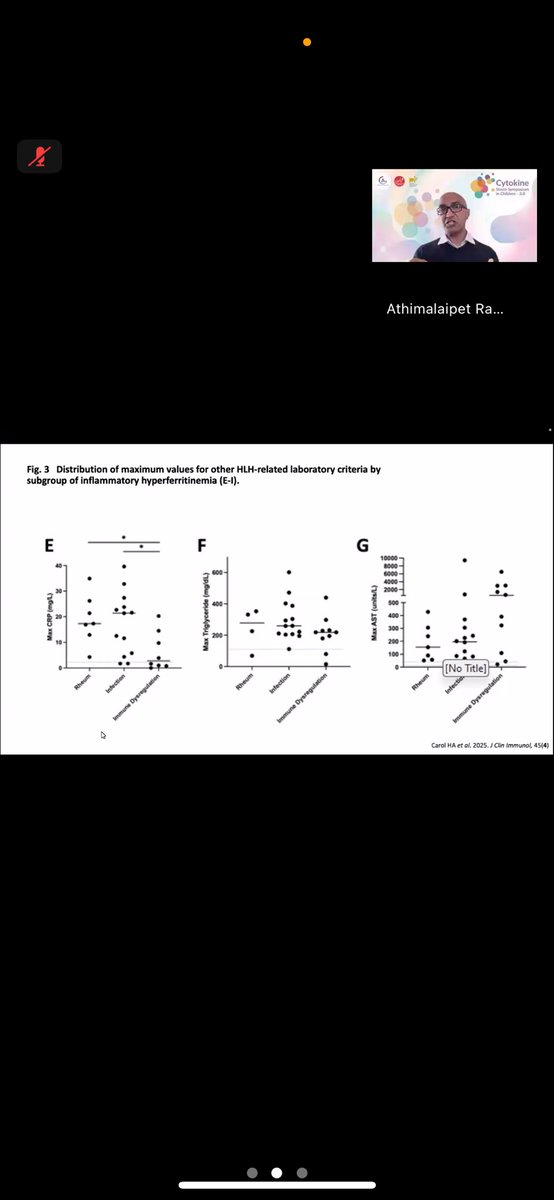
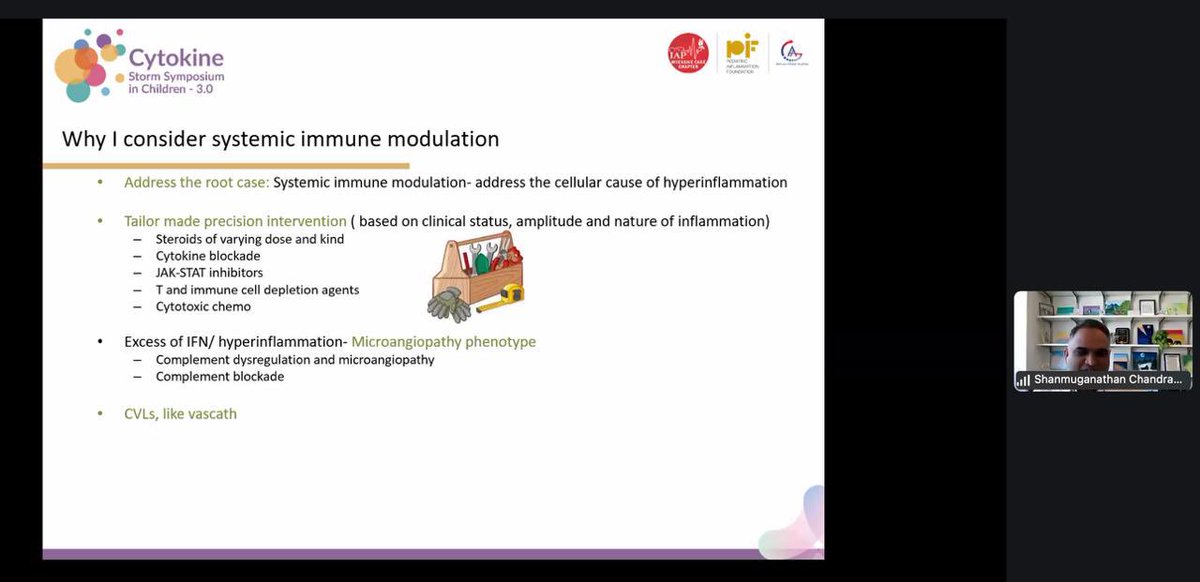
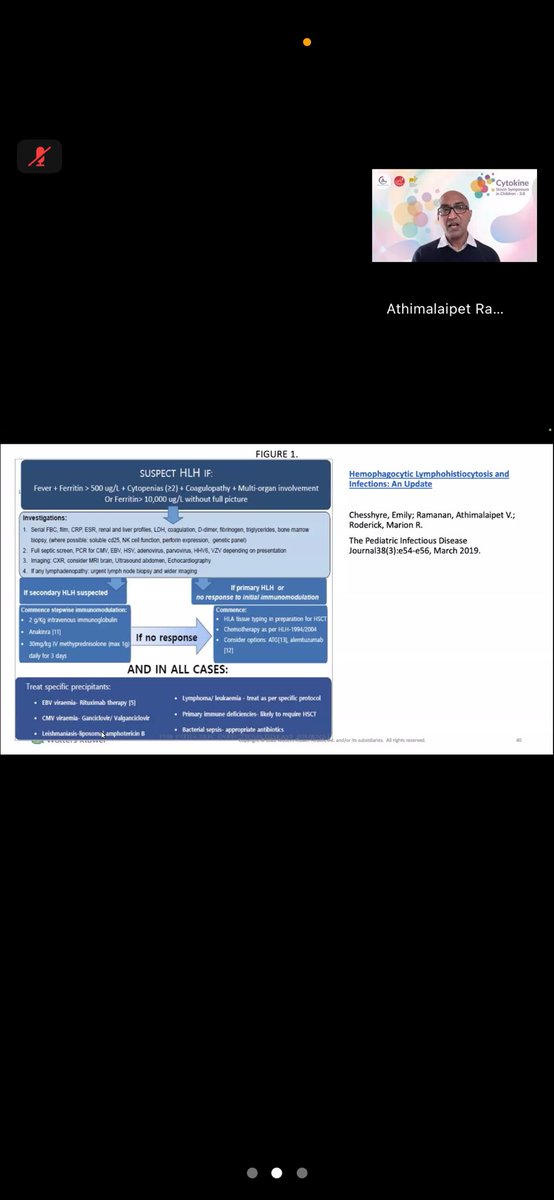
Dr. A.V. Ramanan just delivered a powerful session on ‘Hyperferritinemia in Sepsis: When to Immunomodulate?’ at the Cytokine Storm Symposium — expert insights into timing, thresholds, and therapeutic windows. A masterclass in managing immune chaos!