🍄🚨🍄🚨 Another day, another cool preprint from our group:
An open-label, dose-escalation trial of psilocybin-assisted therapy for bipolar 2 depression
We enrolled individuals with #bipolar 2 (BD-II) currently experiencing a major #depressive episode. Participants must have had at least one unsuccessful medication trial of >6 weeks duration for BD-II over their lifetime. Four participants were on medications with potential #psilocybin interactions, which were tapered under psychiatric supervision to ensure clearance (≥5 half lives) before each administration. Psychiatric exclusions included current hypomania, history of psychotic disorder, moderate substance use disorder in the past 12 months, psychedelic use in the past six months and imminent risk of suicide.
In this open-label, single-arm dose-escalation pilot trial, 14 participants received 10 mg of psilocybin, followed by 25 mg if depressive symptoms persisted. As usual participants underwent psychotherapy before, during, and after psilocybin administration sessions and were proactively monitored for adverse events. Depression and quality of life were assessed using the Montgomery-Asberg Depression Rating Scale (MADRS) and Quality of Life in Bipolar Disorder Questionnaire (QoL-BD), along with exploratory measures.
Following the 10 mg session, MADRS scores significantly improved at all timepoints (A21: -12.7 [2.7], n=14, p<0.001) with 4 participants (28.5%) meeting remission criteria (MADRS ≤ 6) at 21 days after the 10mg dose. Non-remitting patients were given the 25 mg dose per protocol. After the 25 mg session, MADRS scores improved from baseline (B21: -18.6 [3.1], n=9, p<0.001). Sustained improvements in MADRS scores were observed at the 90-day assessment compared to baseline (AB90: -14.3 [2.8], n=12, p<0.001); Hedges’ g=1.9. QoL-BD scores improved 21 days following both the 10 and 25 mg administration sessions (A21: 35.5 [9.4], p<.001; B21: 55.9 [10.9], p<.001) and at the 90-day assessment (AB90: 31.2 [10.2], p=0.004); Hedges’ g=1.6.
As expected, common adverse events included mild-to-moderate anxiety, nausea, and headache on dosing day. There were three notable adverse events: active suicidal ideation 37 days after an administration session, passive suicidal ideation 11 days after an administration session, and a hypomanic episode two weeks after an administration session.
The small sample size and open-label design warrant cautious interpretation. The placebo response likely explains some of the observed benefits. However, in line with previous findings, baseline expectancy was not associated with clinical outcomes - to the best of my knowledge no psychedelic trial has provided empirical evidence for a positive expectancy bias at this point.
Our results offer initial evidence that psilocybin therapy may be clinically beneficial in BD-II when administered under controlled conditions with a safety profile similar to studies in other patient populations.
Full preprint: https://t.co/w0M1NNzoF1
🙏+♥️to all coauthors: @drdowneydoes@thebandlab@ellenbradshaw and many others from the @UCSFPsychiatry 's @TrPR_Program!
#psychedelic #trial #MentalHealthMonday #medicalinnovation
Important to read this if you do work with psychedelic (and other consciousness-changing) drugs in the treatment of psychiatric disorders. Sobering, as they write. Great work by @psybalazs
🔗https://t.co/u0NwBNGV0z
📢New pub from @TrPR_Program@UCSFPsychiatry@UCSFPediatrics
🧠A compelling case for the direct involvement of caregivers in psychedelic therapy for adolescent populations
Treating severe eating disorders in private practice comes with unique challenges.
Join AED on March 25 for expert insights on harm reduction, documentation & team collaboration.
📅 Register today: https://t.co/DtugrbuhQ6
#EatingDisorders#PrivatePractice#EDResearch
Mind the gap! @IntJEatDisord article shows that there is a large unmet treatment need among publicly insured youth with #Eating Disorder in California. They experience high hospitalization rates but receive limited outpatient therapy. https://t.co/yGZLYJ5a7q
In the midst of the national IV fluid shortage, here are some essential tips on IV fluid management for patients with eating disorders.
Take 65 seconds and listen to expert advice on ensuring safe & effective care: https://t.co/SQ3IoCKUbf
#IVFluidShortage#EatingDisorderCare
We really enjoyed the MSR Breakfast which featured some amazing speakers like @drdowneydoes Dr. Young-Walker and Dr. Adelaide Robb sharing insights from their careers! #aacap24
Want confidence in prescribing for patients with eating disorders? Let the AED guide you! Check out "The AED Guide to Selecting Pharmacologic Treatments for Patients with Eating Disorders." 🏥📘
#EatingDisorderResearch
Learn more: https://t.co/TBqUsadf6k
📢 Exciting news! The AED Medical Care Standards Committee has just released "The AED Guide to Selecting Pharmacologic Treatments for Patients with #EatingDisorders."
Want to read more? https://t.co/AMh6RrAUGD
#MedicalCare#Pharmacology#HealthGuidelines
Collection - 'Mindful Journeys: A Careful Exploration of Psychedelics in Eating Disorder Treatment":
💊Exploring physiological responses to psilocybin therapy and their unique impact on Anorexia
📕Read more: https://t.co/pSuiXe5JTR
➡️Submit to collection: https://t.co/yjvICKMj0G https://t.co/zLDwYCDjkX
"Expectancy" and "unblind" was on full repeat yesterday during @US_FDA's discussion of @MAPS's #MDMA trial, so here are a few points that I think can enrich the conversation:
- I do not think its an issue if an intervention has some expectancy effects. The issue is if all or nearly all of it is expectancy.
- That said, MDMA's effect sizes are large enough to accommodate both some expectancy and a drug effect. For example, in one phase 3 trial (https://t.co/4wjdajXrlV), the between-treatment difference was 0.9 standardized mean difference (SMD). That's a LARGE effect. Even if half of it is expectancy, that is still 0.45 SMD. For context, the the difference between placebo and SSRIs is 0.3 SMD (https://t.co/q7wtTpUBZ5).
- Could 0.9 SMD be reasonably explained as just expectancy/unblinding? Did a quick calculation to estimate the unblinding effect on anxiety in our self-blinding microdose trial (https://t.co/clFBOkLJwg), a trial that has a lot of unblinding and clearly high expectancy. The effect was 0.5 SMD.
- Expectancy effects are also expected in #psilocybin therapy just like for MDMA. The only trial that ever assessed it, found no evidence for expectancy effects in psilocybin treatment (https://t.co/UYqBLPvmcV). I am not aware of a single MDMA trial that would have tried to measure it.
I am open to the possibility that much of MDMA's observed effect is expectancy/unblinding, but where I found these arguments shallow yesterday is that there was zero effort trying to quantify the magnitude of expectancy and unblinding effects. You can measure these and provide context from other trials. Given the weight of the decision I expected more in-depth and quantitative arguments around these issues.
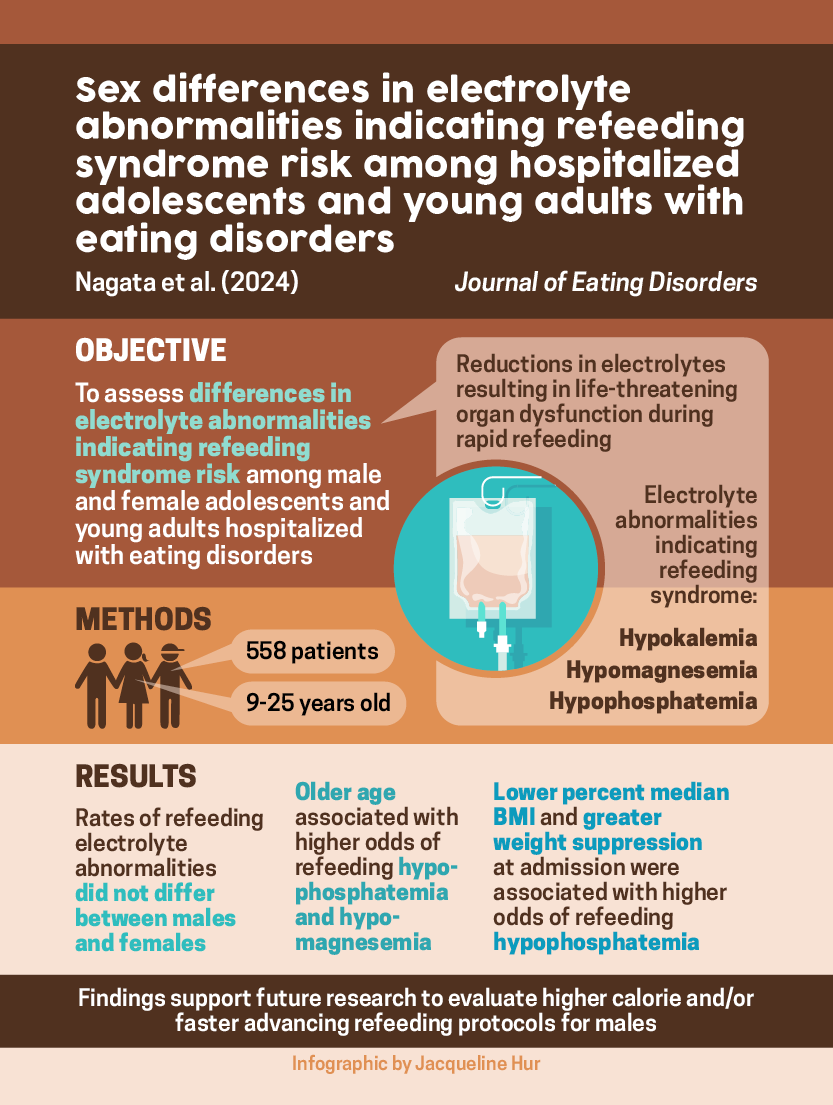
New @UCSFChildrens study in @JEatDisord!
Low rates of refeeding electrolyte abnormalities in males hospitalized with #EatingDisorders
➡️Future studies may consider higher calorie refeeding in males given longer hospital stays and ⬆️ caloric requirements🔗https://t.co/mxUtqm8Gpx
Minor, thoughtful modifications to existing safety protocols are likely to address the unique physiologic vulnerabilities seen in people with AN. Here we provide risk mitigation strategies.
While no study has explicitly examined the pharmacokinetic and pharmacodynamic properties of psilocybin in the setting of malnutrition, studies point to safety regardless of body weight.
🚨 Psilocybin therapy and anorexia nervosa: a narrative review of safety considerations for researchers and clinicians @TrPR_Program https://t.co/wVBmPNaDpX
A Plea for Nuance: Should People with a Family History of Bipolar Disorder Be Excluded from Clinical Trials of Psilocybin Therapy? | Psychedelic Medicine https://t.co/k9cQfynT0C
🚨 New pub from @TrPR_Program@UCSFPsychiatry
🧵 Is near-universal exclusion necessary?
🧵 5/5 We review existing evidence that could inform risk stratification for these individuals and propose a risk stratification tool to be utilized when determining the relative risks of psilocybin therapy to those with a family history of BD in the context of clinical trials.

![psybalazs's tweet photo. 🍄🚨🍄🚨 Another day, another cool preprint from our group:
An open-label, dose-escalation trial of psilocybin-assisted therapy for bipolar 2 depression
We enrolled individuals with #bipolar 2 (BD-II) currently experiencing a major #depressive episode. Participants must have had at least one unsuccessful medication trial of >6 weeks duration for BD-II over their lifetime. Four participants were on medications with potential #psilocybin interactions, which were tapered under psychiatric supervision to ensure clearance (≥5 half lives) before each administration. Psychiatric exclusions included current hypomania, history of psychotic disorder, moderate substance use disorder in the past 12 months, psychedelic use in the past six months and imminent risk of suicide.
In this open-label, single-arm dose-escalation pilot trial, 14 participants received 10 mg of psilocybin, followed by 25 mg if depressive symptoms persisted. As usual participants underwent psychotherapy before, during, and after psilocybin administration sessions and were proactively monitored for adverse events. Depression and quality of life were assessed using the Montgomery-Asberg Depression Rating Scale (MADRS) and Quality of Life in Bipolar Disorder Questionnaire (QoL-BD), along with exploratory measures.
Following the 10 mg session, MADRS scores significantly improved at all timepoints (A21: -12.7 [2.7], n=14, p<0.001) with 4 participants (28.5%) meeting remission criteria (MADRS ≤ 6) at 21 days after the 10mg dose. Non-remitting patients were given the 25 mg dose per protocol. After the 25 mg session, MADRS scores improved from baseline (B21: -18.6 [3.1], n=9, p<0.001). Sustained improvements in MADRS scores were observed at the 90-day assessment compared to baseline (AB90: -14.3 [2.8], n=12, p<0.001); Hedges’ g=1.9. QoL-BD scores improved 21 days following both the 10 and 25 mg administration sessions (A21: 35.5 [9.4], p<.001; B21: 55.9 [10.9], p<.001) and at the 90-day assessment (AB90: 31.2 [10.2], p=0.004); Hedges’ g=1.6.
As expected, common adverse events included mild-to-moderate anxiety, nausea, and headache on dosing day. There were three notable adverse events: active suicidal ideation 37 days after an administration session, passive suicidal ideation 11 days after an administration session, and a hypomanic episode two weeks after an administration session.
The small sample size and open-label design warrant cautious interpretation. The placebo response likely explains some of the observed benefits. However, in line with previous findings, baseline expectancy was not associated with clinical outcomes - to the best of my knowledge no psychedelic trial has provided empirical evidence for a positive expectancy bias at this point.
Our results offer initial evidence that psilocybin therapy may be clinically beneficial in BD-II when administered under controlled conditions with a safety profile similar to studies in other patient populations.
Full preprint: https://t.co/w0M1NNzoF1
🙏+♥️to all coauthors: @drdowneydoes @thebandlab @ellenbradshaw and many others from the @UCSFPsychiatry 's @TrPR_Program!
#psychedelic #trial #MentalHealthMonday #medicalinnovation](https://pbs.twimg.com/media/GvSHDzIaYAIEZ4Q.jpg)






















![psybalazs's tweet photo. 🍄🚨🍄🚨 Another day, another cool preprint from our group:
An open-label, dose-escalation trial of psilocybin-assisted therapy for bipolar 2 depression
We enrolled individuals with #bipolar 2 (BD-II) currently experiencing a major #depressive episode. Participants must have had at least one unsuccessful medication trial of >6 weeks duration for BD-II over their lifetime. Four participants were on medications with potential #psilocybin interactions, which were tapered under psychiatric supervision to ensure clearance (≥5 half lives) before each administration. Psychiatric exclusions included current hypomania, history of psychotic disorder, moderate substance use disorder in the past 12 months, psychedelic use in the past six months and imminent risk of suicide.
In this open-label, single-arm dose-escalation pilot trial, 14 participants received 10 mg of psilocybin, followed by 25 mg if depressive symptoms persisted. As usual participants underwent psychotherapy before, during, and after psilocybin administration sessions and were proactively monitored for adverse events. Depression and quality of life were assessed using the Montgomery-Asberg Depression Rating Scale (MADRS) and Quality of Life in Bipolar Disorder Questionnaire (QoL-BD), along with exploratory measures.
Following the 10 mg session, MADRS scores significantly improved at all timepoints (A21: -12.7 [2.7], n=14, p<0.001) with 4 participants (28.5%) meeting remission criteria (MADRS ≤ 6) at 21 days after the 10mg dose. Non-remitting patients were given the 25 mg dose per protocol. After the 25 mg session, MADRS scores improved from baseline (B21: -18.6 [3.1], n=9, p<0.001). Sustained improvements in MADRS scores were observed at the 90-day assessment compared to baseline (AB90: -14.3 [2.8], n=12, p<0.001); Hedges’ g=1.9. QoL-BD scores improved 21 days following both the 10 and 25 mg administration sessions (A21: 35.5 [9.4], p<.001; B21: 55.9 [10.9], p<.001) and at the 90-day assessment (AB90: 31.2 [10.2], p=0.004); Hedges’ g=1.6.
As expected, common adverse events included mild-to-moderate anxiety, nausea, and headache on dosing day. There were three notable adverse events: active suicidal ideation 37 days after an administration session, passive suicidal ideation 11 days after an administration session, and a hypomanic episode two weeks after an administration session.
The small sample size and open-label design warrant cautious interpretation. The placebo response likely explains some of the observed benefits. However, in line with previous findings, baseline expectancy was not associated with clinical outcomes - to the best of my knowledge no psychedelic trial has provided empirical evidence for a positive expectancy bias at this point.
Our results offer initial evidence that psilocybin therapy may be clinically beneficial in BD-II when administered under controlled conditions with a safety profile similar to studies in other patient populations.
Full preprint: https://t.co/w0M1NNzoF1
🙏+♥️to all coauthors: @drdowneydoes @thebandlab @ellenbradshaw and many others from the @UCSFPsychiatry 's @TrPR_Program!
#psychedelic #trial #MentalHealthMonday #medicalinnovation](https://pbs.twimg.com/media/GvSHJfzX0AALeB8.jpg)