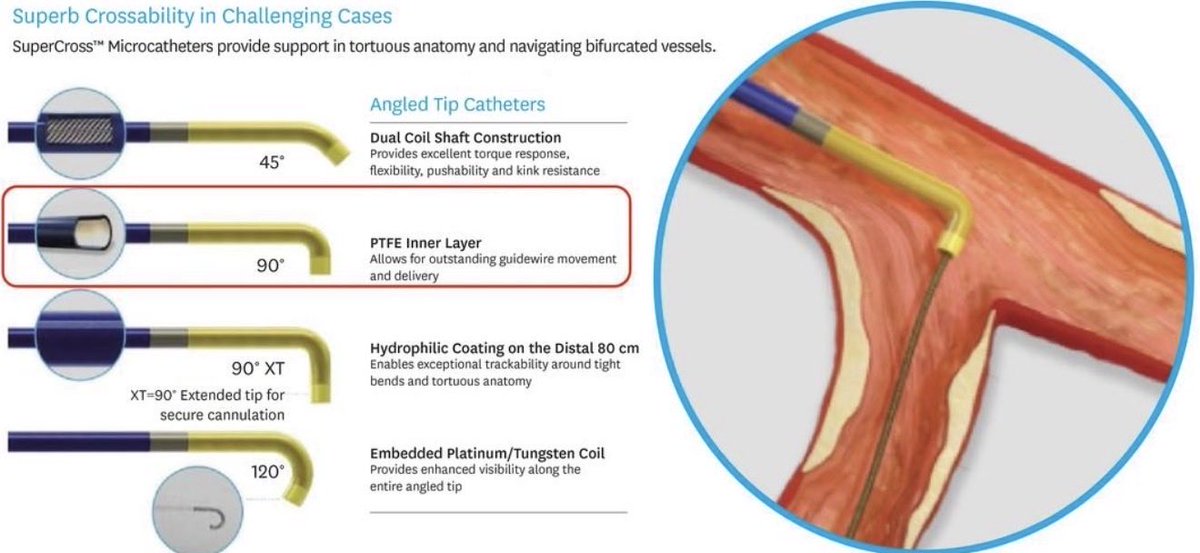
A flush-occluded LAD with a near 90° takeoff, a 9 mm left main, and a 5 mm LAD at 4:30 PM after a full day in the cath lab… character-building STEMI 😊
The 90° SuperCross & Pilot 200 came to the rescue.
@TeleflexCardiol@AbbottCardio ✊🏾
Teaching points:
👉Know your tool box 🧰
👉We usually avoid “nailing” the ostium when there’s no landing zone. But when IVUS shows a 9mm left main nearly twice the size of the LAD, sometimes the perfect stent landing zone simply doesn’t exist.
👉Complex PCI is sometimes about choosing the best imperfect option.
#STEMI #PCI #IVUS #CathLab
@ACCinTouch@SCPEthiopia@HeartAEthiopia@mmamas1973
#ACCEarlyCareer
🔊 Proper IVL balloon prep matters!
Even small amounts of residual air can reduce sonic pressure by up to 20%. And remember: non-ionic contrast alone won’t work. IVL requires a saline-contrast mixture to generate shockwaves.
🎥 See the video for the correct technique.
🚦FFR-Positive, Ischemia-Negative: The Elephant in the Room
For years, we have been told that after an abnormal CCTA, functional testing helps identify the lesions that “really matter.”
This large individual patient-data meta-analysis challenges that assumption.
Among patients with ≥50% stenosis on CCTA:
✅ Functional imaging identified anatomically severe CAD reasonably well (81% sensitivity).
❌ But for lesions with FFR ≤0.80, sensitivity dropped to only 64% overall.
In other words:
A substantial proportion of FFR-positive lesions do NOT produce detectable ischemia on stress imaging.
This raises an uncomfortable question:
If a lesion is FFR-positive but does not generate measurable ischemia, what exactly are we measuring?
A pressure gradient?
A biological disease process?
Or a surrogate endpoint that only partially overlaps with clinically relevant myocardial ischemia?
The study also showed that the most advanced imaging techniques (PET and high-field CMR) were more sensitive, while more traditional approaches were more specific. Yet even the best modalities failed to identify all FFR-positive lesions.
The broader implication
Perhaps the problem is not that functional imaging is insufficient.
Perhaps the problem is the expectation that:
FFR-positive = ischemic = clinically relevant
These concepts are related.
They are not synonymous.
As cardiac imaging continues to evolve, the future may lie less in choosing between anatomy and physiology and more in integrating:
👉 plaque burden
👉 plaque phenotype
👉 myocardial consequences
👉 symptoms
👉 physiology
into a unified disease model.
Because coronary artery disease is more complex than a pressure wire value.
#CardiacCT #CCTA #FFR #PET #CMR #CoronaryArteryDisease #PrecisionMedicine #PreventiveCardiology #CardiovascularImaging
A p-value below the noninferiority threshold is not a free pass. Noninferiority margins need clinical justification, and intention-to-treat and per-protocol analyses should ideally point in the same direction. As DES outcomes continue to improve, noninferiority trials of coronary devices become increasingly fragile.
Here's a case describing a novel technique (the double-DCB technique) for the treatment of recurrent in-stent restenosis by applying 2 different DCBs, thereby avoiding the implantation of another layer of metal in our patients. https://t.co/dXa5lfToF9 #JACCCaseReports#PCI
In the multicentre randomised DOUBLE-CHOICE trial, the ACURATE neo2 valve was non-inferior to the Evolut platform in selected anatomies undergoing TAVI.
The primary composite endpoint at 30 days occurred less frequently with ACURATE neo2, largely driven by significantly lower permanent pacemaker implantation rates, while rates of stroke and moderate/severe prosthetic valve regurgitation remained low in both groups.
🔗https://t.co/5bCQYodw04
#TAVI #StructuralHeart #InterventionalCardiology #CardioTwitter #CardioEd
@feistritzerH_J@thiele_holger@mvonroeder
#CardioNugget™
In outlet/supracristal VSDs, the right coronary cusp can lose its supporting septal “shelf” and get pulled/prolapse into the VSD by the Venturi effect from the high-velocity LV→RV jet.
Over time:
RCC prolapse → poor cusp coaptation → progressive aortic regurgitation.
Board pearl:
VSD + new AR = think RCC prolapse, especially outlet/supracristal VSD.
#CardioNugget #MedEd #VSD #CardioMed #CongenitalHeartDisease
Image from: https://t.co/faTphG0eHx
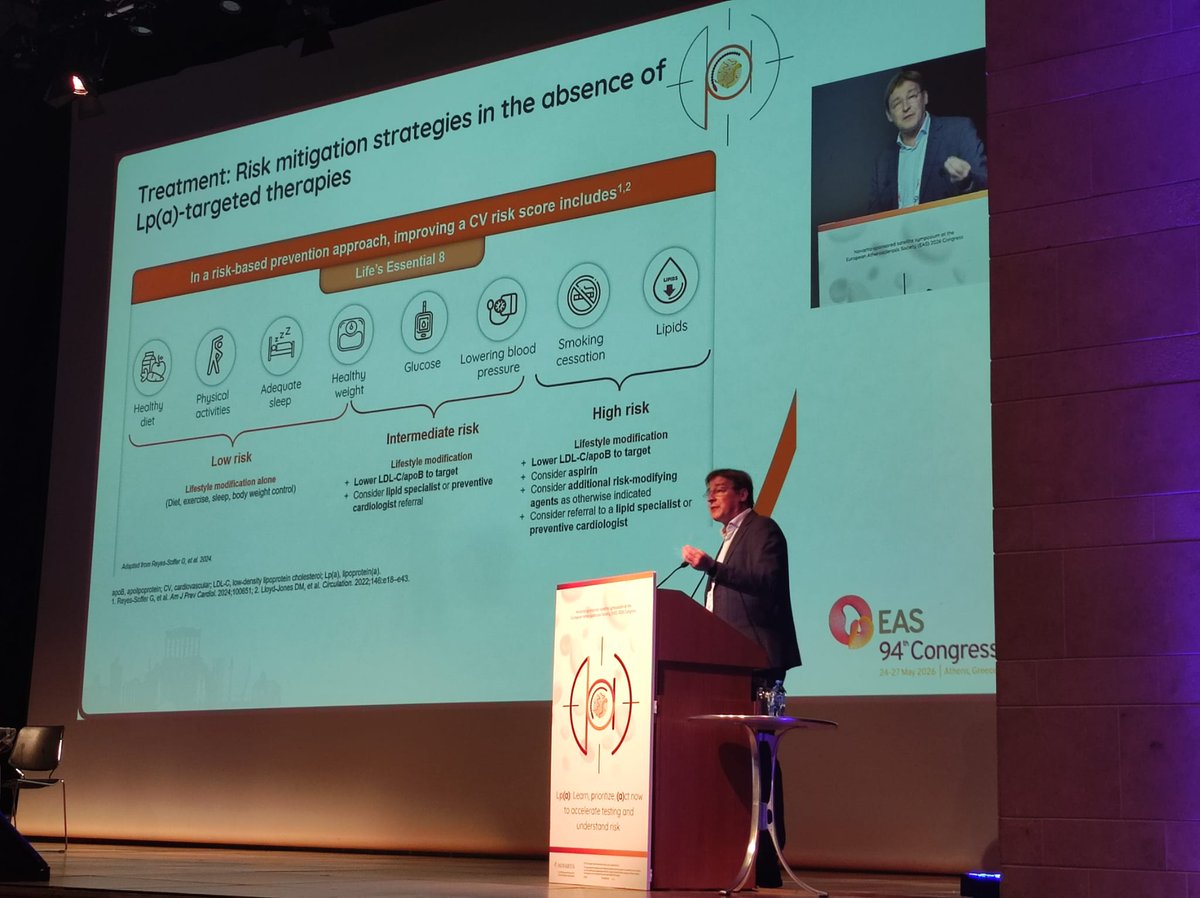
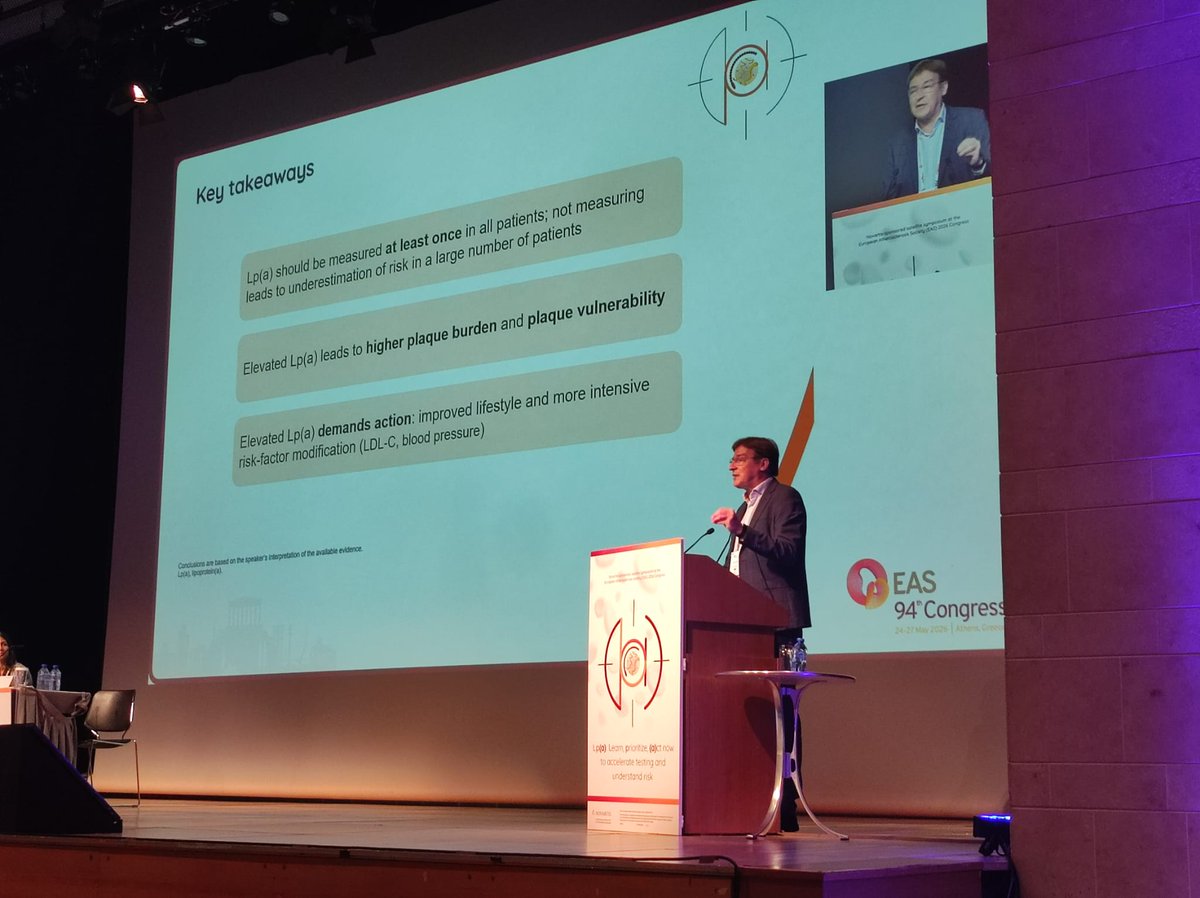
Not measuring Lp(a) means underestimating inherited risk in many patients.
Elevated Lp(a) is linked to higher plaque burden/vulnerability, and should push us to act on total risk: LDL-C/ApoB, BP, lifestyle and other modifiable factors. #MyEAS2026#EASCongress2026
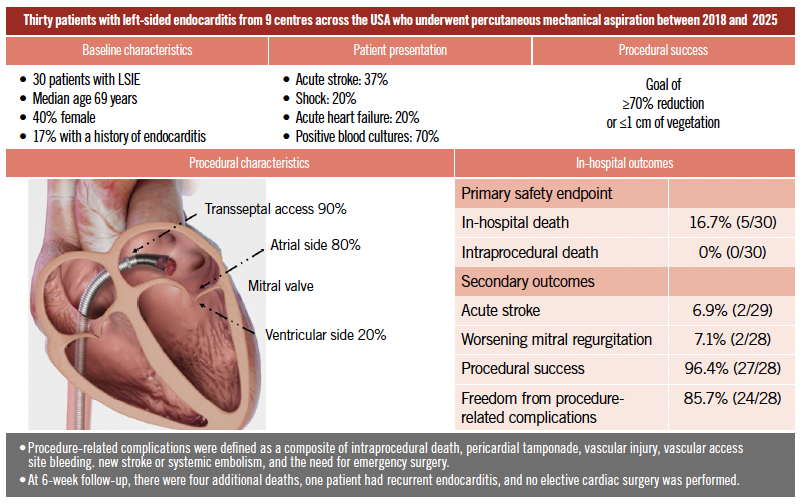
This analysis presented as SIMULTANEOUS PUBLICATION #EuroPCR from the CLEAR-IE registry evaluated percutaneous mechanical aspiration in patients with left-sided infective endocarditis.
In a high-risk cohort, PMA was associated with high procedural success and a favourable rate of procedural complications despite the complexity of disease presentation.
Read full paper 🔗https://t.co/UlbXFzLItA
#Endocarditis #StructuralHeart #InterventionalCardio
@NahyrLugo@benhibbertMDPhD@PedroMDMSc@SripalBangalore@MohammedQintar@SEH_MD@psorajja@HamidNadira@sahilparikhmd@aelsab
What are you doing after BCIS-CHIP 3?
❓Impella vs no Impella for high risk PCI
❓Should we be renaming it- High hemodynamic risk PCI?
Here’s a case where PCI was not possible
w/o support. EF 15% EDP 34. Lost pulsitility even w/ RCA PTCA. DK crush LM not possible without support
#Cardiology #CardioX #PCI #Impella @BotPci@RadialFirstBot
🔥 NOW ONLINE 🔥simultaneous presentation #EuroPCR
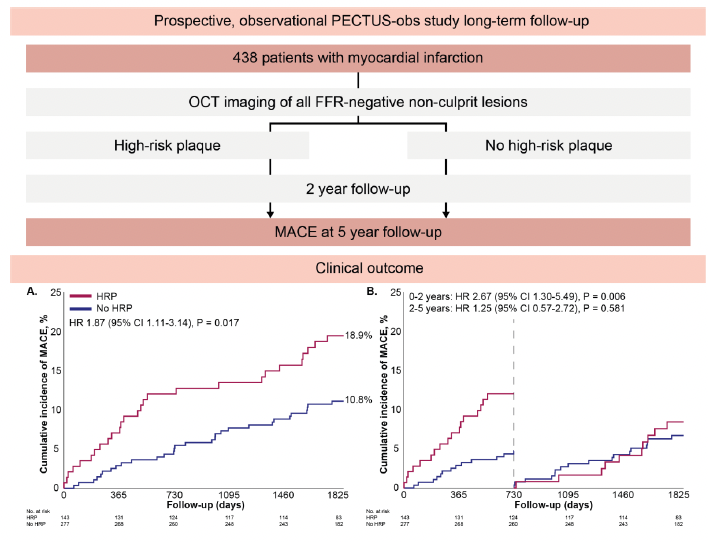
PECTUS-OBS LONG TERM FOLLOW-UP
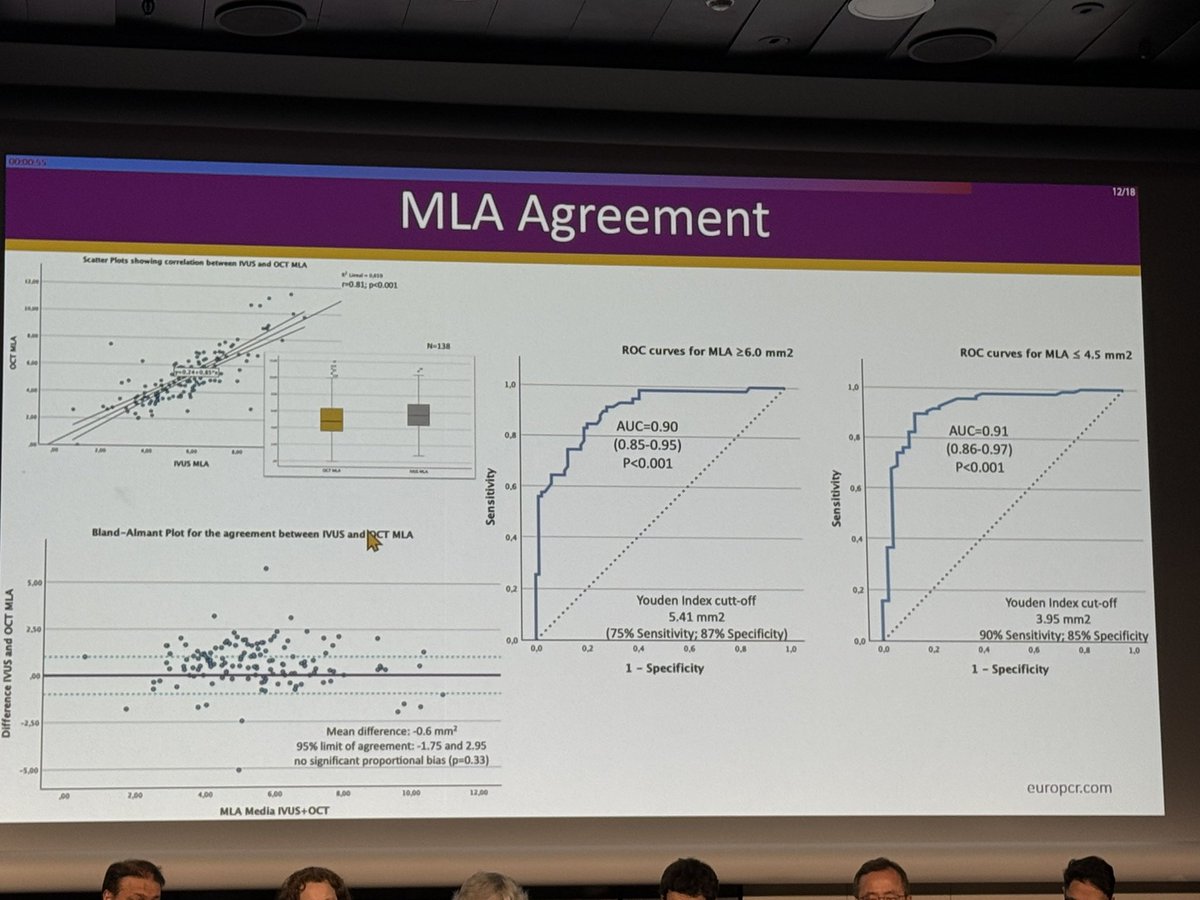
In this study, OCT-identified high-risk non-culprit plaques with negative FFR were associated with a significantly higher risk of long-term adverse cardiovascular events after myocardial infarction.
At 5 years, patients with at least one high-risk plaque had increased rates of non-fatal MI and unplanned revascularization despite non-flow limiting physiology.
🔗https://t.co/lmdobkYGur
@RickVolleberg@NielsRoyen@RGeuns
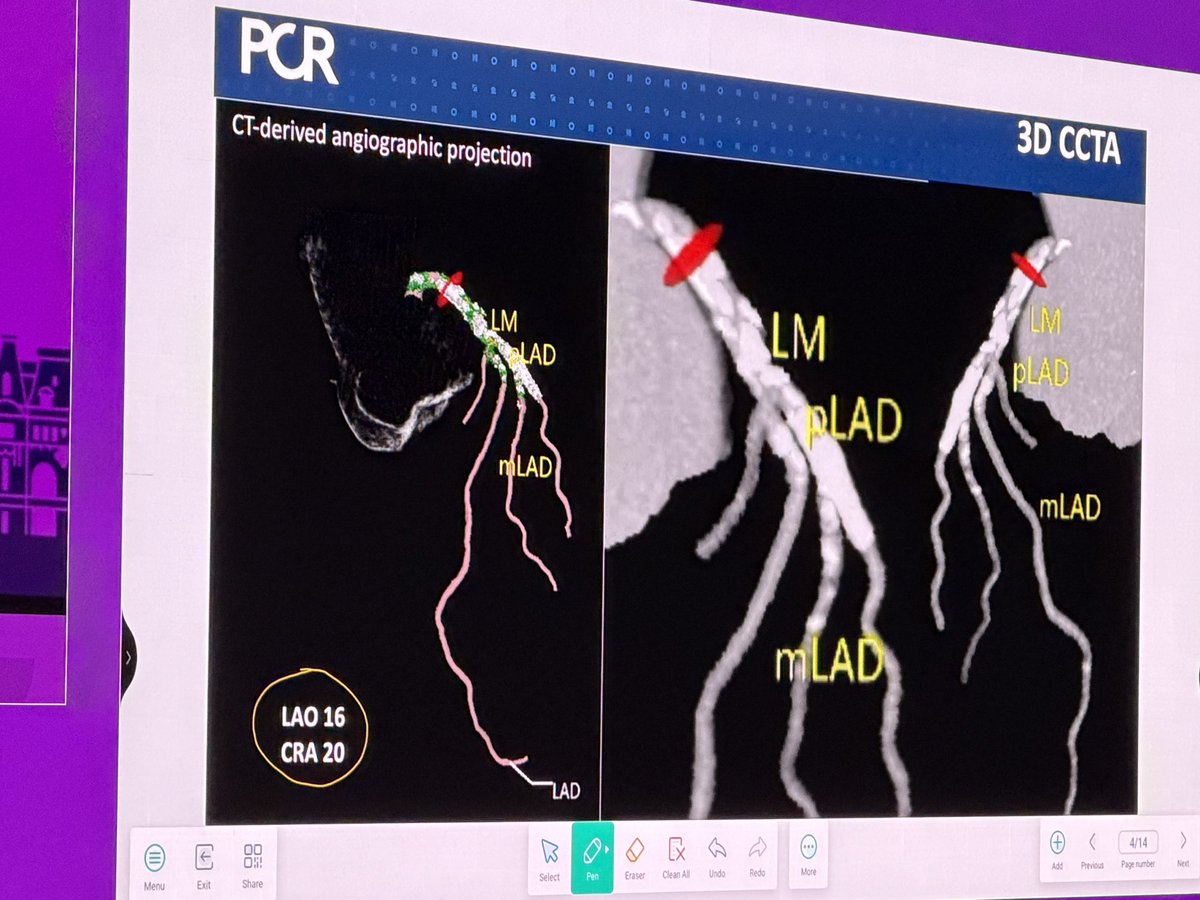
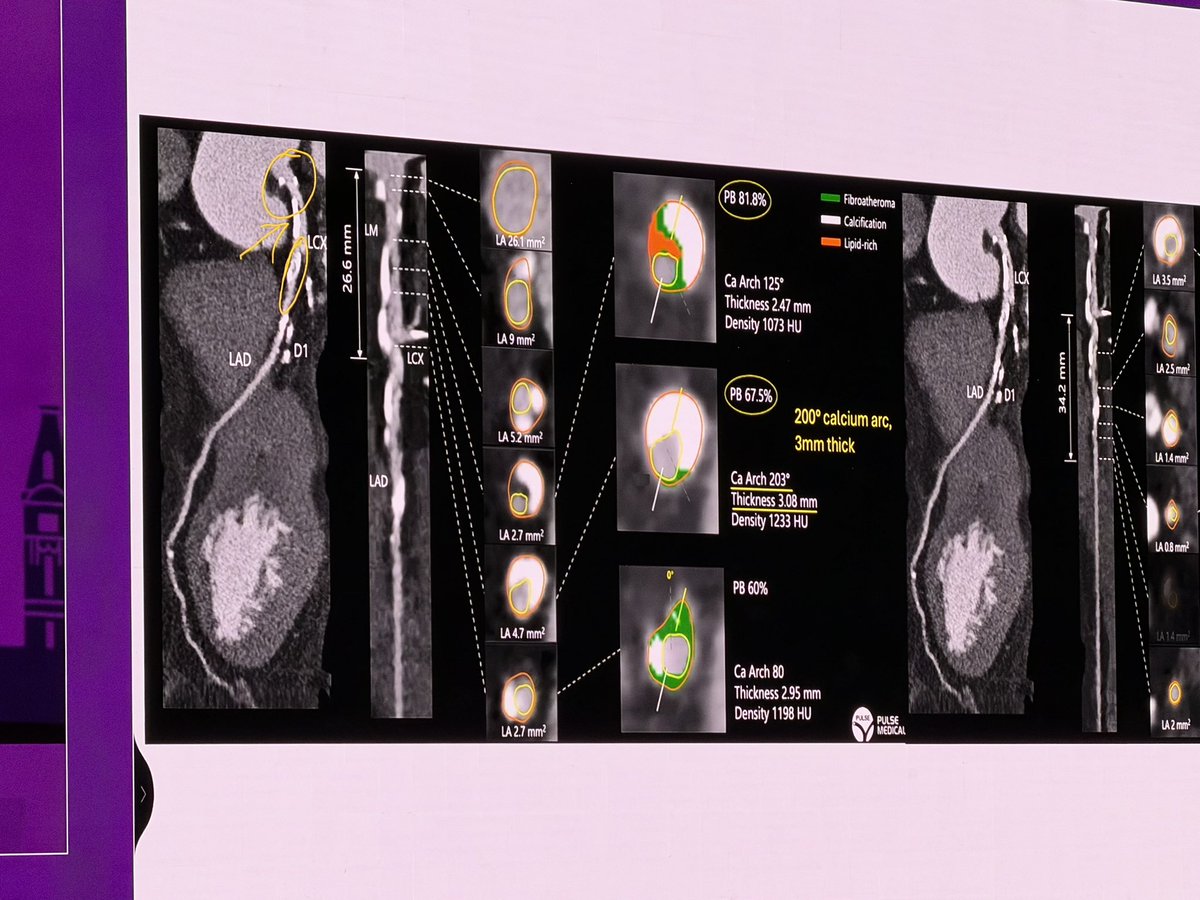
I wanted to go have a coffee, but I can’t leave my seat! @GoranEBC#EuroPCR and an AMAZING analysis of the CTCA before going live, I will do this when back home! @PCRonline
Stepwise provisional strategy decided by looking at the CT images!!
Transcaval TAVR case today with @BinAbdulHak_A.
Transcaval remains one of the crown jewels in our field. It’s hard to think of another structural procedure, besides VECTOR, that challenged traditional endovascular dogma to this extent: safely and predictably exiting vessels, delivering large-bore sheaths, and achieving percutaneous closure.
Regarding this case:
• Traversal: 6 Fr IMA 55 cm, 135 Turnpike, 90 Navi, Astato 20 (50 W electrocautery), 20 mm Gooseneck
• Aortic closure: Agilis small curl, ADO 10/8
If a 55 cm JR is unavailable, using an IMA will usually bias the wire inferiorly. Advancing the Navi to the tip of the catheter helps eliminate that bias.
The Check-Flo 30 (shown below) is very helpful for locking the relationship between the Navi and Finecross. That’s useful not only in transcaval cases, but also in procedures such as UNICORN, BASILICA, BATMAN, and LAMPOON.
If you don’t have a Check-Flo 30, a 0.035 torquer can be a reasonable compromise.
Join us at @TCT_ME_ in Sep 2026. Will have a lot of great #Electrosurgery discussions.
@6ayyeboon@AlkashkariWail@mirvatalasnag@amrmohsen213@MarwanSaadMD@aelsab@MusaSharkawi@djc795@MohammedQintar@mhammadah@kalazizimd@AdamGreenbaumMD@AlhijjiM@EmoryUniversity@JDDCFratti@acamajmd@crfheart@djc795@mmamas1973@TCT_ME_@crfheart@BakhshiHooman@Almanfi_Cardio@Dr_ibrahimHarbi@scottiejj12
I would say that the KISS trial @JACCJournals not only proved that you do not need to do routine SB intervention (commonly kissing), rather I would say the most significant change is proving the concept of POT-side-POT (done in 57% of SB interventions and seems to be more favorable than kissing).
I have been recently doing POT-side-POT instead of kissing when I need SBI and that study proved it can be better!
Congrats to the authors and @sbrugaletta for an insightful editorial!
https://t.co/H3m2dHoufQ
#cardioX
Whoa!!!
Here!
The Swiss cheese layered airline model to prevent complications.. a chapter that should be read by everyone who works in a Cath Lab!
@PCRonline , open for free just on the eve of #EuroPCR my read on the flight from Cairo.