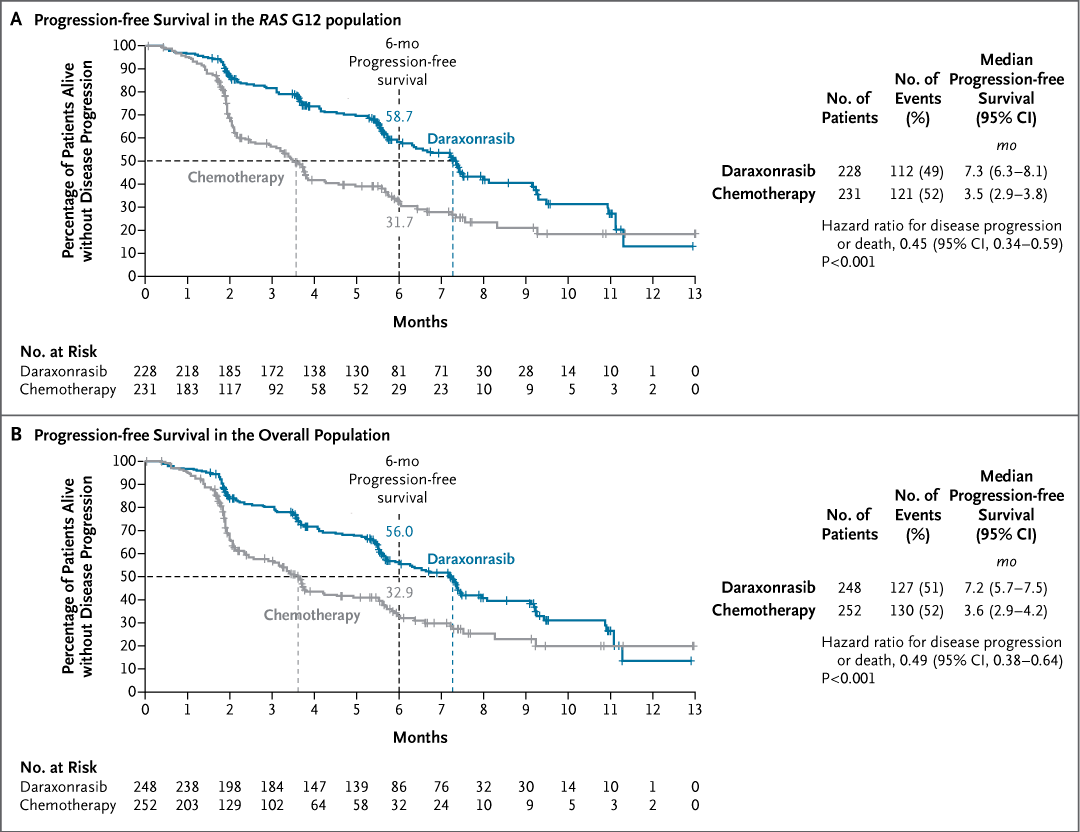
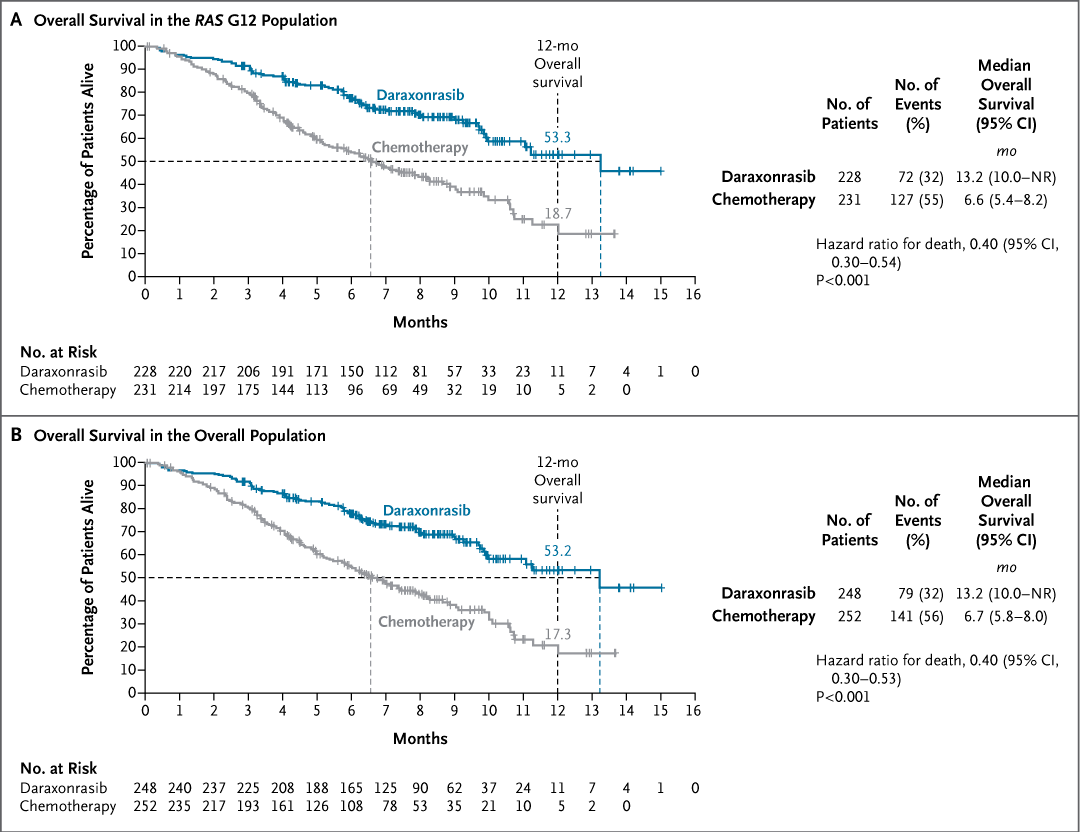
Original Article: Daraxonrasib or Chemotherapy in Previously Treated Metastatic Pancreatic Cancer (phase 3 RASolute 302 trial) https://t.co/y4G27hfORg
#ASCO26 | @ASCO
NEW: You might be charged double for a routine medical visit.
Corporations and hospitals are buying up private practices across the country, then tacking “facility fees” onto standard appointments.
While Americans are stuck paying hundreds more for a single doctor’s visit, corporate executives are raking in billions.
Who the hell were these gynecologists treating Epstein’s victims? Because let’s be crystal clear, if you were a physician and you ignored, enabled, minimized, or looked the other way while children were being abused, you failed medicine, you failed ethics, and you failed humanity. Like, y’all just suck. Licenses don’t cancel mandatory reporting. And “just doing your job” is not a defense when children are being exploited. Y’all should be ashamed of yourselves.
$71.8 million.
That is how much one 50-employee independent practice loses to insurance carriers over a 30-year career.
It is insane!
The grift is real!
Not to malpractice.
Not to bad management.
To the middleman.
I did the math.
Today I published the receipt.
Full breakdown here:
https://t.co/OqJnkJK9AG
60,000+ healthcare professionals read The Rojas Report.
The public should be far angrier about facility fees than it is.
Picture two clinics. One is an independent physician practice. The other is the exact same type of clinic, same doctors, same rooms, same services, but owned by a large hospital system.
That second clinic is classified as a hospital outpatient department. Nothing about the care is different. But the prices a "hospital outpatient department" gets to charge the government are multiple times higher than the independent clinic.
Routine office visits, imaging, echocardiograms, in office procedures all get marked up simply because a hospital’s name is on the door. The independent doctor gets paid one rate. The hospital owned clinic gets paid more for doing the exact same thing.
That extra money lets the hospital pay higher staff salaries, outbid independents for equipment, spend more on marketing, and layer on amenities that have nothing to do with care. The independent physician is now competing against a system that is legally allowed to charge more for identical services.
Patients are mostly blind to this. They are not told they are walking into a higher priced clinic. They do not see the facility fee until the bill shows up.
And then the patients are screwed again once enough independent practices are driven out of business. Patients lose the option of seeing a lower cost physician altogether. They are forced into hospital owned clinics that charge more and often deliver a worse experience.
This is not an accident. Medicare explicitly wrote these payment rules into its fee schedules. Private insurers largely follow Medicare’s lead, so the distortion spreads across the entire system.
It's almost as if the system is designed to elminate independent physician practice...
$275 billion.
That's the annual subsidy flowing to health systems.
This is the moat.
This is why health insurance premiums rise.
Subsidies do not flow to patients.
Not to physicians or your communities.
Instead, they flow to health systems.
And you're paying for it.
Every premium.
Every tax dollar.
Every bill you can't afford.
$UNH loses $96B in market cap because … checks notes … 0.09% increase in Medicare 2027 insurer rates
Meanwhile … standard cataract surgery reimbursement has faced cumulative cut for CPT 66984 from 2020 to 2026: -17% unadjusted (-30%+ inflation-adjusted, assuming ~2-3% annual CPI).
Such a shame their CEOs will only take home 15-20 million next year instead of 30. It is actually a travesty that these companies that make profit off of denying Americans healthcare ( with no accountability or liability) are so integral to the Dow Jones performance.
Humana and United stocks are tanking today because CMS is only giving them a small raise next year 0.09%. Meanwhile independent physicians have had reimbursement cut by 30 percent over the past 2 decades. Where are the histrionics and press releases on this tragedy which is driving the private practitioner into extinction.
The American Hospital Association spent $29 million on lobbying in 2024.
55% of their lobbyists are former government officials.
People who wrote the rules.
Then crossed the street to protect them.
This is the health system business model....
Week 2 — Medicare Physician Fee Schedule Updates and Cuts: Ongoing Threats to Independent Practice Viability
Happy Monday. This week we’re taking a deep dive into the CY 2026 Medicare Physician Fee Schedule (PFS) final rule (CMS-1832-F, released October 31, 2025)—and what it really means for independent physician practices.
At first glance, the news looks positive. CMS finalized a 3.26% increase in the conversion factor for most physicians (non-qualifying APM participants), raising it to $33.40 (from $32.35 in 2025). That increase reflects a one-time 2.5% statutory boost from Congress (via the One Big Beautiful Bill Act) plus a +0.49% budget-neutrality adjustment.
After years of cuts, that’s welcome relief. But let’s be clear: this is a temporary patch, not a structural fix.
Key threats to independent practice viability in the final rule include:
• A new –2.5% “efficiency adjustment” applied to work RVUs for most non-time-based services, based on a 5-year lookback of MEI productivity factors—disproportionately impacting procedural and diagnostic specialties.
• Changes to indirect practice expense allocation in facility settings, cutting the portion tied to work RVUs in half and widening site-of-service differentials that favor hospital outpatient departments over independent offices.
• No permanent inflation adjustment: Medicare physician payments have declined an estimated 25-33% in real terms since 2001, while practice costs (rent, staffing, supplies) continue to rise—and hospitals still receive automatic MEI-linked updates.
The result is continued pressure on independent practices, accelerating consolidation into hospital or corporate models that often prioritize scale and volume over patient-centered care. Despite the headline increase, many specialists—including orthopedics, interventional, and surgical fields—face net cuts, threatening access in rural and suburban communities, including here in Texas.
This week, we’ll unpack the details:
• Tuesday: The efficiency adjustment—why it’s flawed and who it hurts most
• Wednesday: Site-of-service differentials and the quiet erosion of independent offices
• Thursday: Specialty-specific impacts (skin substitutes, telehealth, and more)
• Friday: Policy Solutions—why permanent MEI-linked updates matter and how physicians can engage
Independent practices remain the backbone of personalized, high-quality care. Outdated payment policy shouldn’t be the reason they disappear.
😭😭😭
Who exactly is going to cut their prices ? Independent physicians can barely pay their bills. DPC is already a bargain. Hospitals are going to get rid of facility fees or walk away from keeping 340b margins and passing that to the patient ? No.
Big PBMs are going to stop charging fees ? No. Big insurers are going to stop gaming vertical integration transfers ? No
Break up the big insurance companies first. Make them divest each vertical , PBMs, Providers, ASOs , Digital They are the ATT1984 of 2026.
Break them up.
They have become Too Big To Care
We should put together a thread of common misconceptions about money in Healthcare.
1. Doctors don't get a tax write-off for charity care or unpaid bills
2. Medicare hasn't increased payment rates to doctors since 1992
3. Seeing a hospital-employed doctor costs twice as much as seeing a private doctor in the same office building, because of facility fees
4. We spend $50-60 Billion per year in facility fees for office visits, enough to fund ACA subsidies and finally tie physician payments to inflation, and still have $ leftover
5. After overhead and taxes, a surgeon takes home about $300 for doing a complex 3-hour revision hip replacement
6. Doctor and nurse salaries account for a smaller portion of Healthcare spending in America than in our peer countries (Combined 16%)
7. Total Administration spending in America is 30% of Healthcare costs, which is substantially higher than any other country (Singapore is 3-5%)
8. Healthcare administrator salaries have tripled since 1992, while physician payments per work-RVU from Medicare have increased 3%
Got any more to add?
Site-Neutral Payments, the 80 Billion Typo
Here’s a simple question:
Why does Medicare pay 3x more for the exact same service simply because it happens inside a hospital building?
It’s called “site-of-service differential,” and it’s the most expensive pricing mistake in American healthcare.
Hospitals figured this out fast:
Buy a physician’s office,
flip the billing code,
keep doing the exact same thing,
but now charge 10x.
Costs exploded.
Competition collapsed.
Premiums rose.
And Congress?
They’ve known about this for 15 years….
Medicare site-neutral payments would cause CMS to lose its influence and bankrupt the subsidy model that props up the non profit health system monopolies. Thats why your premiums are high.
CMS reimburses hospital outpatient departments (HOPDs) at significantly higher rates—often 40-60% more—than ambulatory surgical centers (ASCs) for identical procedures under Medicare's outpatient prospective payment system (OPPS) versus ASC-specific rates. This disparity stems from historical hospital cost structures baked into OPPS, without adjustments for actual procedure complexity in non-hospital settings. It drives the "HOPD shift," where hospitals acquire ASCs or offices to bill at premium levels, inflating national spending by billions annually while ASCs face competitive disadvantages. Site-neutral reforms aim to equalize payments based on service, not location.
Nonprofit health systems issue tax-free municipal bonds.
They skip income tax.
They skip property tax.
They skip sales tax.
They even access low-cost capital like Wall Street firms.
Independent doctors get commercial loans at full interest and pay taxes at every level.
So when a billion-dollar hospital tower goes up with a charity logo on it, that isn’t philanthropy.
Nonprofit is a label.
The financial model is pure arbitrage.