Starting residency can be challenging—presenting 10 patients daily on floors is no joke! Here’s my approach to staying efficient:
-Arrive early.
-Review age, PMH, and chief complaint.
-Check ED vitals, labs, imaging, and where the patient came from.
-Review overnight events (ask the night team), vitals, and morning labs.
-Check consultant notes (e.g., cardiology updates).
-Update assessment/plan, and place necessary orders.
-For new patients, review prior hospitalizations.
-Track hospitalization course—know the big picture.
-Check PT/case management for mobility concerns and placement.
-After chart review, talk to nurses, check telemetry, and ensure alignment.
-See patients, update them, take history, do a physical exam—always introduce yourself!
-Review with seniors to catch anything missed.
It’s challenging at first, but practice makes perfect.
I hope this helps future interns; however, I am still learning and improving!
#ResidencyLife #MedTwitter #Efficiency #medicine
Confession: I LOVE hyponatremia 🤓
(I know, I know. What can I say, I'm a true internist!)
HypoNa is often feared, maligned, and misunderstood - but I promise it doesn't have to be scary!
Here are my top 10 hyponatremia tips and tricks - a 🧵
Every week, I see a new study talking about this or that effect of GLP-1 receptor agonists like #ozempic. FINALLY, we have a study evaluating all the outcomes (good and bad) in one dataset. There are some... surprises. 🧵
(1/x) Intubating a critically ill patients is the most dangerous procedure we do in the ICU (3.1% cardiac arrest rate) not because of hypoxia or tube placement, but hemodynamic collapse 🫀
(Russotto et al. JAMA 2021)
A 🧵on making high risk hemodynamic intubations as safe as possible.
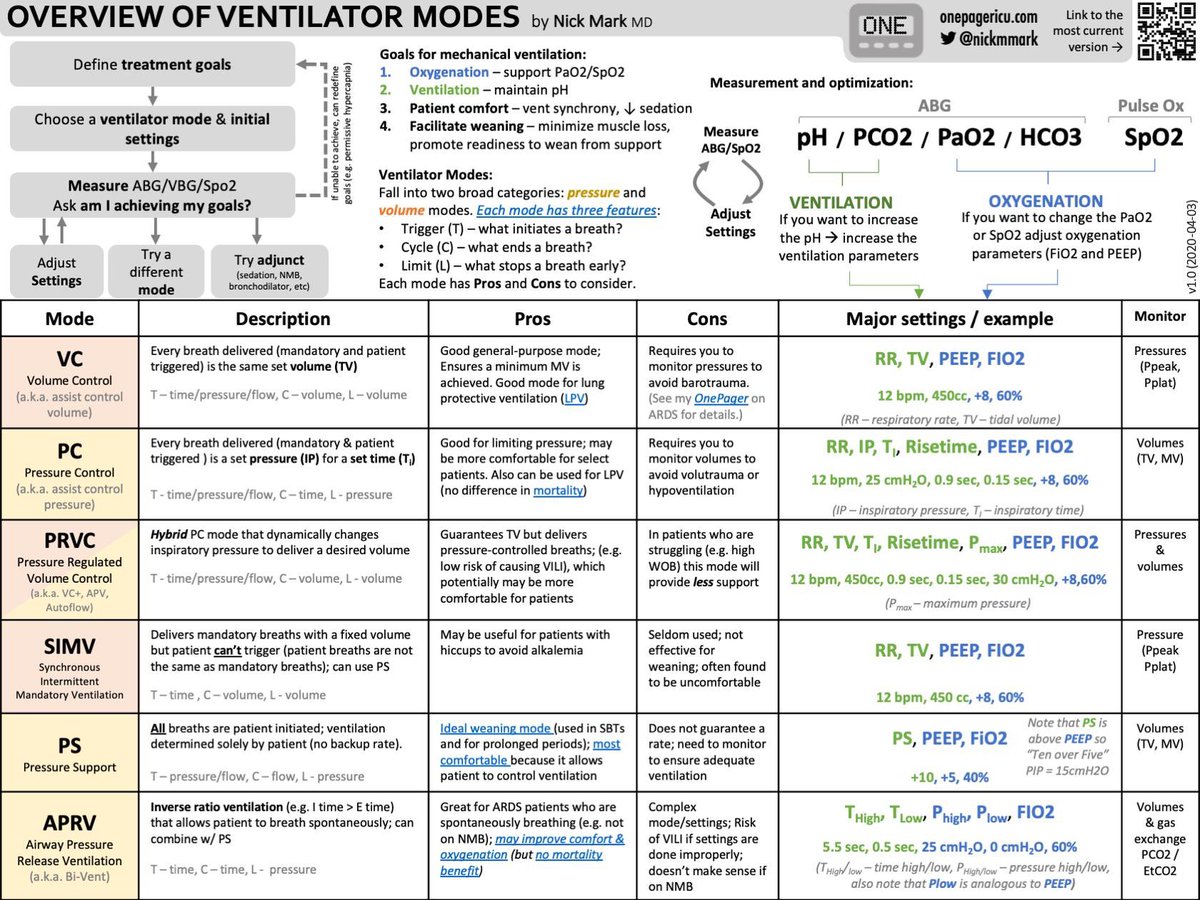
“Ventilator Modes Overview 🫁:
1️⃣ VC (Volume Control): Fixed volume; good for LPV but risk of barotrauma.
2️⃣ PC (Pressure Control): Set pressure; prevents barotrauma but may cause hypoventilation.
3️⃣ PRVC: Adaptive mode; ensures tidal volume but increases work of breathing.
4️⃣ SIMV: Partial support; useful for weaning but less effective for full support.
5️⃣ PS (Pressure Support): Weaning mode; patient-triggered but no set rate.
6️⃣ APRV: ARDS mode; improves oxygenation but complex settings.
VBG Interpretation 🩸:
1️⃣ pH: Evaluates ventilation.
2️⃣ pCO2: Adjust ventilation to correct acidosis/alkalosis.
3️⃣ FIO2 and PaO2: Assesses oxygenation.
4️⃣ SpO2: Monitor and adjust O2 delivery.
ICU (Central Venous/Arterial) Line Secrets - Part 1:
An ICU where the patients have no central lines & are not connected to ventilators is not a real ICU. This may be a controversial statement but in my humble opinion not far from truth
1/Do radiologists sound like they are speaking a different language when they talk about MRI?
T1 shortening what? T2 prolongation who?
Here’s a translation w/an introductory thread to MRI.
1/
Why can furosemide improve dyspnea/pulmonary edema from acute congestive heart failure within minutes of administration?
The answer does not involve diuresis.
#medtwitter#tweetorial
🧵regarding the useful technique of 'straightening the wire' during central line placement when the plastic guide is no longer within reach.
If you do a lot of central lines (or a lot of percutaneous procedures), this technique will come in handy over and over again.
(1/ )
Dear incoming interns:
Remember that your attendings have been practicing medicine for years, while you're essentially getting a new job every 4 weeks.
Know that your job is not to know everything. You job is to show up, ask questions, & care deeply for your patients.