1/11 My good deed for the week. A 🧵
Halfway through my endo list yesterday the DSU nurse came in.
“The last patient's arrived with his mother. He’s autistic and says he gets seizures when he is overstimulated.” She handed me his file. “There’s a letter from the neurologist”.
TW: ENDING OF LIFE
Have my #ActuallyAutistic comrades ever been bullied and harassed so much that this is something they’ve considered?
We are 11x more likely to according to the latest study.
We need more support. More awareness.
YOU’RE NOT ALONE
#AskingAutistics
@DocEd@doctorcaldwell@TimBonnici Imagine if you added an ML to it to make sure it’s the true abnormals/trend of change for that pt (not just everything out of lab ref range)
I die a little in reposting my own stuff, but I think this is fascinating stuff. The NHS desperately needs to improve productivity, and there's an answer to that staring us right in the face. Training clinicians properly on EPRs can deliver massively increased efficiencies.
@DigitalNurseMel @DHCNIO Spot on. And I reckon we can do both. The safety work helps work out what to monitor and how to weave into quality management systems. Nuanced Agile methodology helps too.
Clinical decision-making is a complex process involving patient characteristics, medical history, evidence, and clinician and patient values. It's crucial to consider risks, benefits, resources, and ethical and legal aspects. It's much more challenging than many people realise.
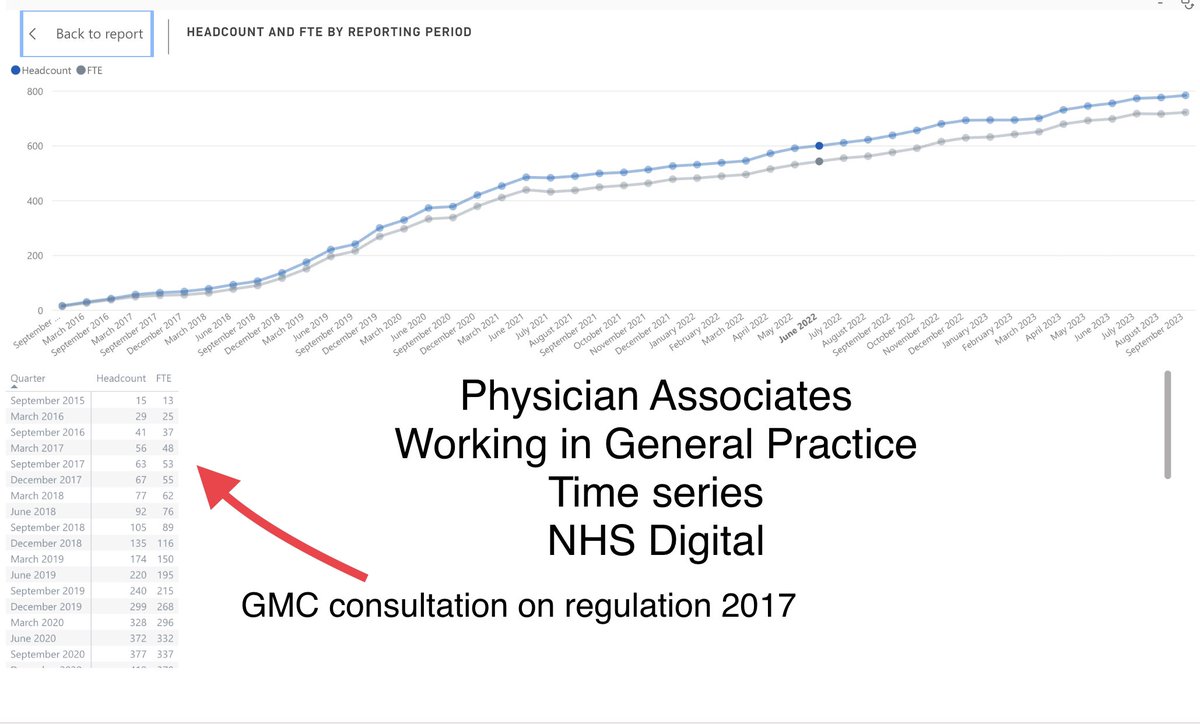
The consultation on the regulations around PAs was in 2017 (Published 2019)
Less than 70 PAs were working in GP at the time & very few GPs responded
It is important to get this right for PAs, making it safe for them & patients, giving clear future guidance for all concerned
@hasyourregtried I did a vasc surgery job as a ho. When I was relieved from retractor holding, I sat with the anaesthetist and we talked physiology. Those weekly 1:2:1 discussions nearly made me choose anaesthetics. & def helped in every exam I did after that.
You make a good point.
@jraph97 Being a supervisor of a dr in training is different than being the supervisor for other HCPs.
JDs present cases so they can hone Hx & exam skills in a relatively safe way, so they will spot when things don’t fit the textbook. Protocols, algorithms and lesser experience ≠
@jraph97 It also depends how the case was presented. Which will have been verbal. If you don’t know to put the Sx together in the right way then, unless the reviewer sees and hears from the pt themselves, it will continue to be missed.
I'm genuinely upset that non-MBBS graduates can now join FY1. Yes, its a trial scheme, but this is a real erosion of the NHS doctor.
There is no equivalency, a medical degree is accredited, registered, audited and rigorous. Its 110% from day one for 5-6yrs.
@TheEMboardround@DrLindaDykes Not being funny, but did you read the constellation of symptoms?
We need to look at how skills are being matched in settings and to symptoms to make sure pts are the someone with the right skill-mix to see them. And ppl whose knee jerk isn’t “you’re fine, go home”
@drkeithsiau PS for anyone who gets them, when you feel them start, stop what you’re doing, press hard/squeeze and put your hand above your head. Usually stops them from being super painful.