TAP or Trap? - Rethinking the True Territory of the Transversus Abdominis Plane Block
#BeyondTAP#AbdominalAnalgesia#RegionalAnesthesia#TAPBlock#QuadratusLumborum#QLBlock#EOIP#FascialPlaneBlocks#PainManagement#UGRA#AcutePain#AnatomyMatters#BlockSmart #SomaticVsVisceral #KnowBeforeYouBlock
#MyRATips #TipOfTheDay
Tip of the Day:
✨ The Transversus Abdominis Plane (TAP) block is often perceived as a comprehensive abdominal wall block.
✨ Anatomically and clinically, however, its coverage is selective, variable, and frequently incomplete. Let’s decode it logically.
🧠 Segmental - Not Complete Dermatomal Coverage
🔹 Targets anterior rami of T6–L1 within the fascial plane
🔹 Spread is plane-dependent and inconsistent
🔹 Neural branching forms a TAP plexus → dermatomal predictability drops
🔹 Upper abdominal coverage (T6–T9) is unreliable
➡️ Reality: Partial somatic sensory block - not uniform dermatomal anesthesia.
🧩 Medial Sparing - The Rectus Sheath Gap
🔹 Anterior Cutaneous Nerves (ACNs) pierce the posterior rectus sheath
🔹 TAP does not reliably block ACNs
🔹 Midline analgesia requires Rectus Sheath Block
🔹 “Medial escape zone” phenomenon
➡️ Reality : Without RSB, central abdominal wall remains inadequately covered.
⚡ Lateral Cutaneous Nerve Escape
🔹 Lateral cutaneous branches exit early from the neurovascular plane
🔹 Standard lateral TAP frequently spares them
🔹 Posterior TAP improves but does not guarantee coverage
➡️ Reality : Lateral abdominal wall analgesia may be incomplete.
💪 Muscle Innervation Overlap - No True Motor Promise
🔹 Abdominal wall muscles have overlapping segmental innervation
🔹 Blocking selected segments ≠ muscle paralysis
🔹 TAP is primarily sensory
➡️ Reality: It is not a muscle relaxation technique.
🔥 No Visceral Analgesia
🔹 Blocks somatic afferents only
🔹 Visceral pain travels via sympathetic & splanchnic pathways
🔹 Peritoneal stretch & bowel manipulation remain untouched
➡️ Reality: Not adequate as a standalone block for intra-abdominal surgery.
🤔 So Why Consider TAP at All?
Because it still has value, when chosen rationally.
✅ Superficial abdominal wall procedures
✅ Part of multimodal analgesia
✅ When neuraxial is contraindicated
✅ To reduce opioid requirement
✅ When combined strategically (RSB + posterior TAP)
🎯 Decision Lens
🔹 Lower abdominal superficial → TAP acceptable
🔹 Upper abdominal → EOIP preferred
🔹 Mixed somatic + visceral → QL more rational
🔹 Major open abdominal → Epidural still gold standard
🔑 Take-Home
✨ TAP is not wrong - it is simply limited.
✨ It is a plane block, not a pan-abdominal solution.
✨ Choose based on pain source: somatic vs visceral vs mixed.
حقيقة السوشي التي لا يعرفها الكثيرون ، #رشفه_صغيره_ومعلومة_كبيرة#yourzu
هل كنت تعتقد ان السوشي يعني سمك نيء فقط؟
يورزو يكشف الحقيقة المدهشة وراء السوشي ومعناه الحقيقي في الثقافة اليابانية
رشفة معرفة سريعة ستغير نظرتك للسوشي الى الابد
#السوشي#حقائق_غريبة
@alsayg (تفسير الاحلام الشامل)
تفسير رؤيا هدايا الذهب يعتمد على تفاصيل الرؤيا وسياقها، بالإضافة إلى حالة الرائي وظروفه. بشكل ��ام، الذهب في المنام يرمز إلى معانٍ متعددة، منها:
* **الخير والبركة:** الذهب معدن نفيس، وغالبًا ما يدل على الخير والرزق والبركة في...
https://t.co/dQwh9jLTRE
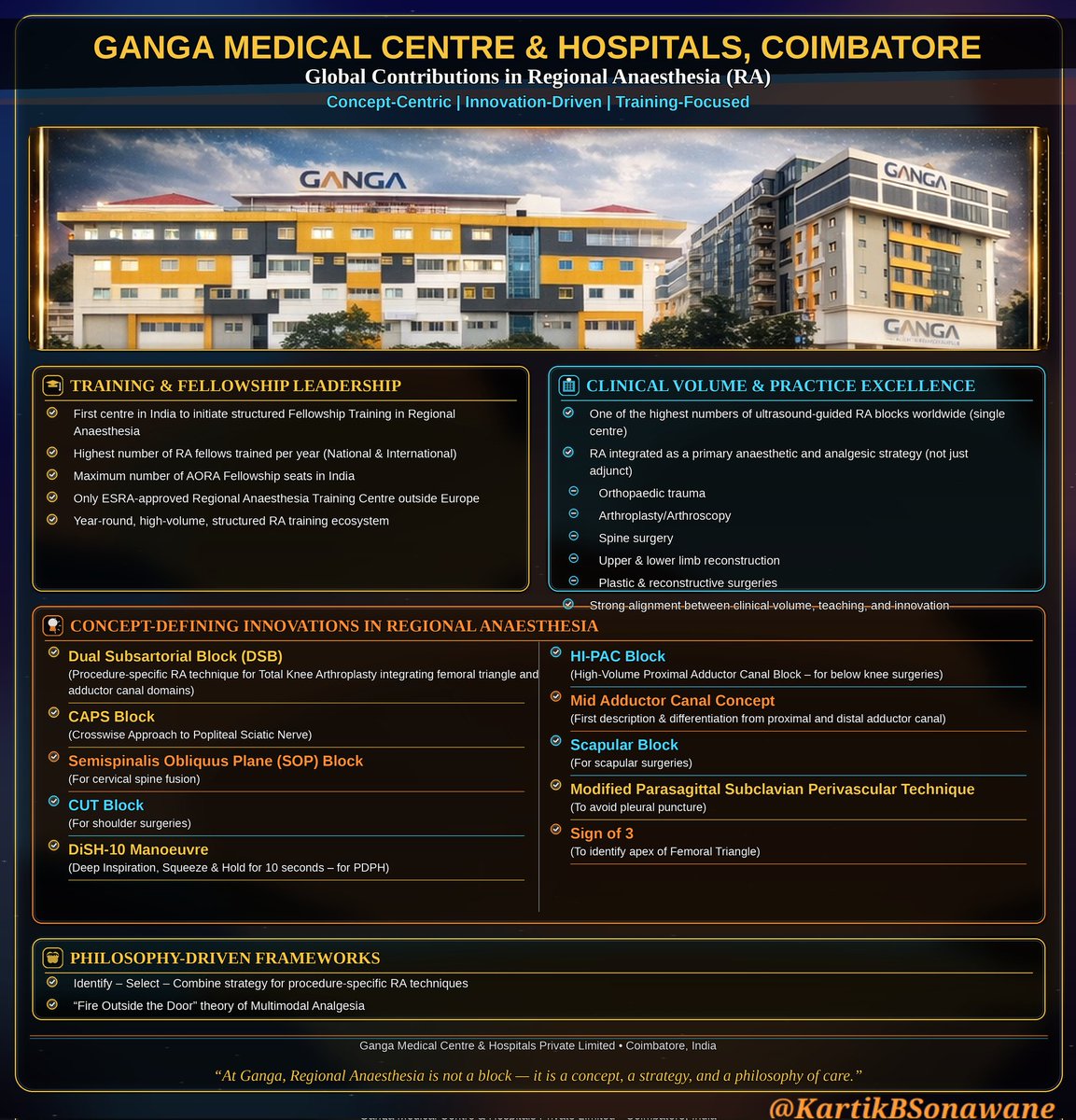
🌍✨ From Ganga to the Globe: Redefining Regional Anaesthesia (RA) ✨🌍
#RegionalAnaesthesia#UltrasoundGuidedRA#GangaHospital#GangaMedicalCentre#Coimbatore#India#Anesthesia#PainManagement#NerveBlocks#RegionalAnesthesia#RAInnovation#FellowshipTraining#ESRA#AORA #MedicalEducation #OrthoAnaesthesia #TKA #MultimodalAnalgesia #AcademicAnaesthesia #PatientCenteredCare
My 3 Ps (Place,Practice, Pride) 🏥🇮🇳
At Ganga Medical Centre & Hospitals Private Limited, Coimbatore, India 🇮🇳🏥
Regional Anaesthesia is not just a technique…
✅ It is a concept 💡
✅ It is a strategy 🎯
✅ It is a philosophy of care ❤️
🏆🎓 Training & Fellowship Leadership
✅ First centre in India to initiate structured Fellowship Training in Regional Anaesthesia
✅ Highest number of RA fellows trained per year (National 🌏 + International 🌍)
✅ Maximum number of AORA Fellowship seats in India
✅ Only ESRA-approved Regional Anaesthesia Training Centre outside Europe 🇪🇺➡️🌏
✅ Year-round high-volume structured RA training ecosystem 📚💉
⚡🏥 Clinical Volume & Practice Excellence
✅ Among the highest numbers of ultrasound-guided RA blocks worldwide (single centre) 🌎📈
✅ RA practiced as a primary anaesthetic + analgesic strategy, not just an adjunct 🔥
✅ Strong RA integration for:
🔸 Orthopaedic trauma 🦴
🔸 Arthroplasty/Arthroscopy🦿
🔸 Spine surgery 🧠
🔸 Upper & lower limb reconstruction 🦾🦵
🔸 Plastic & Reconstructive Surgeries
💡🚀 Concept-Defining Innovations in RA
✅ Dual Subsartorial Block (DSB) (Procedure-specific RA technique for TKR integrating femoral triangle + adductor canal domains)
✅ HI-PAC Block (High-volume Proximal Adductor Canal Block – for below-knee surgeries)
✅ Mid Adductor Canal Concept (First description & differentiation from proximal and distal AC)
✅ CAPS Block (Crosswise Approach to Popliteal Sciatic Nerve)
✅ Scapular Block (For scapular surgeries)
✅ Semispinalis Obliquus Plane (SOP) Block (For cervical spine fusion)
✅ Modified Parasagittal Subclavian Perivascular Technique (to avoid pleural puncture)
✅ CUT Block (For shoulder surgeries)
✅ Sign of 3 (Sonoanatomical Landmark to identify apex of femoral triangle)
✅ DiSH-10 Manoeuvre (Deep Inspiration + Squeeze + Hold for 10 sec – for PDPH)
🧠🔥 Philosophy-Driven Frameworks
✅ Identify – Select – Combine approach for procedure-specific RA techniques 🎯
✅ “Fire Outside the Door” theory of Multimodal Analgesia 🔥🚪
✅ "Gray Zone" of PENG block (Deciding ultimate fate of analgesia)
🌟 Ganga’s contribution is not a cluster of achievements - it is years of discipline, innovation, teaching, and scientific mindset. 💪📖✨
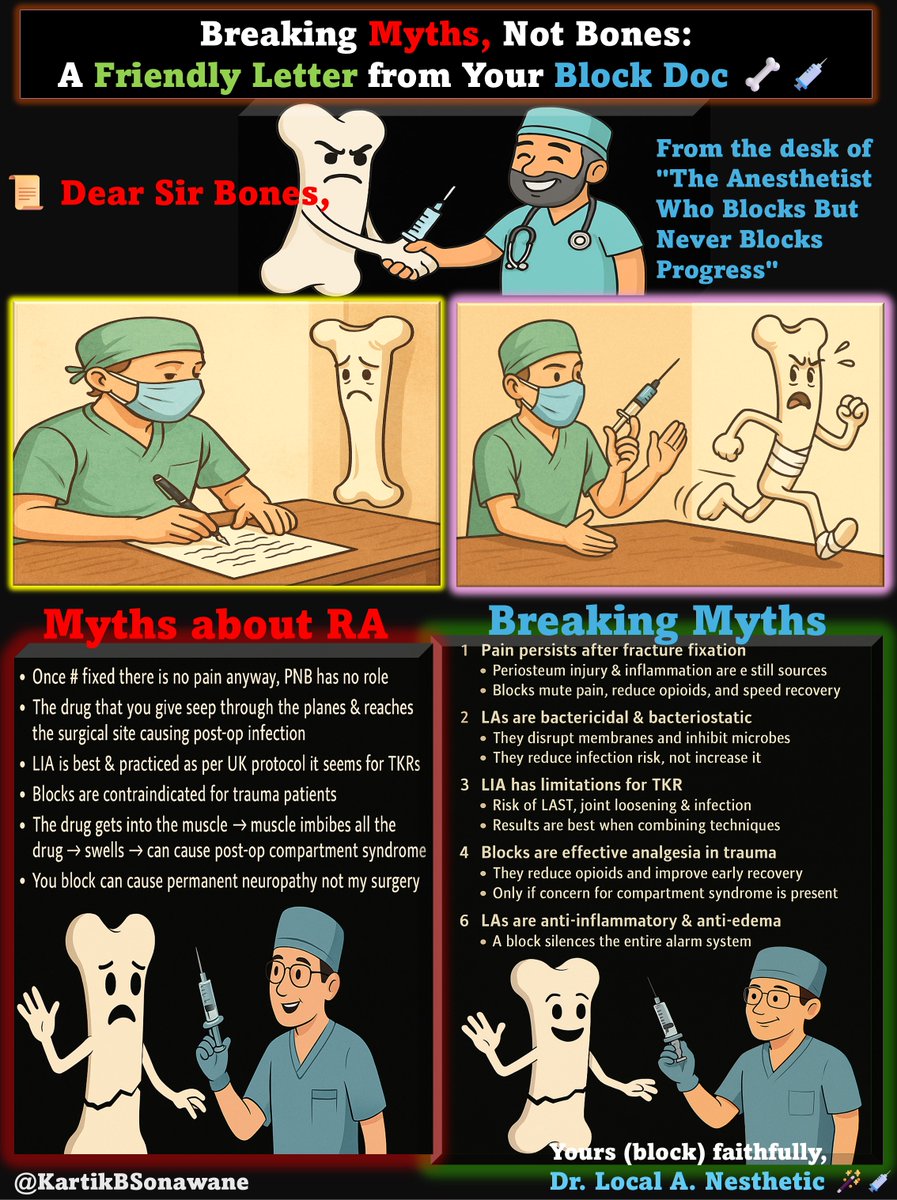
Breaking Myths, Not Bones: A Friendly Letter from Your Block Doc 🦴💉
#RegionalAnesthesia#NerveBlocks#PainFreeSurgery#BreakingMyths#MythBusting#BlockDoc#AnesthesiaEducation#LIA#TraumaCare#OrthopaedicMyths#TipOfTheDay#MyRATips
Tip of the Day:
📜 Dear Sir Bones,
From the desk of "The Anesthetist Who Blocks But Never Blocks Progress"
Your reasons for banning peripheral nerve blocks (PNBs) are so imaginative they could fill a stand-up special.
Unfortunately, in the theatre, patients aren’t laughing.
Here’s my myth-by-myth reply — fun to read, hard to refute.
💥 Excuse #1: "Once fracture fixed, there is no pain anyway"
🧠That’s like saying once a tooth is pulled, the nerve endings won’t notice.
📚 Fact: Fixation stops instability, but pain from soft tissue injury, periosteum, and inflammation remains. PNBs mute these signals and accelerate rehab.
🦠 Excuse #2: "Drug seeps to surgical site → infection"
🧽That’s like fearing soap will cause skin infections because it touches the skin.
📚 Fact: Local anesthetics are sterile and fight bacteria:
🔓 Disrupt membranes
⛔ Inhibit microbial enzymes
🧪 Work better in acidic tissue
Translation: They reduce infection risk.
🇬🇧 Excuse #3: "LIA is best; UK protocol for TKR"
🍽True, the UK likes tea - but coffee works too.
📚 Fact: LIA can work, but it’s far from flawless:
⏳ Short-lived analgesia → severe breakthrough pain
⚠️ Risk of LAST from high-volume infiltration
🔩 Joint loosening and infection risk if asepsis lapses
🔄 Redo surgeries in infected or unstable joints
Translation: Best practice = multimodal analgesia. Blocks add safety, comfort, and duration.
🚑 Excuse #4: "Blocks contraindicated for trauma patients"
⛑That’s like saying helmets are contraindicated for motorbike riders.
📚 Fact: Blocks reduce opioids, aid physio, and speed recovery. The exception? Suspected compartment syndrome — but that’s a specific, not a blanket, rule.
💪 Excuse #5: "Drug in muscle → swelling → compartment syndrome"
🎈That’s like thinking a cup of tea will swell your stomach until your belt snaps.
📚 Fact: Local anesthetics are anti-inflammatory & anti-edema:
🚫 Inhibit neutrophil migration
💨 Suppress pro-inflammatory cytokines (IL-1, TNF-α)
🧱 Reduce capillary permeability
Translation: They reduce swelling, not cause it.
🧩 Excuse #6: "I haven’t touched those nerves, why are you blocking them?"
🎯That’s like saying, I didn’t hit the alarm, so why turn it off while it’s still blaring?
📚 Fact: Pain signals don’t care if you “touched” a nerve. Surgical trauma triggers pain in connected pathways. Blocks interrupt these signals before they even start.
🛑 Excuse #7: "Joint replacement patients don’t feel pain after surgery"
😂That’s like claiming marathon runners don’t get thirsty at the finish line.
📚 Fact: Capsule, ligaments, and periosteum still fire pain signals. Blocks prevent severe rebound once spinal or GA wears off.
📏 Excuse #8: "This is not what we follow, so don’t give"
🛠That’s like refusing power tools because your grandfather used a hammer.
📚 Fact: Medicine evolves - protocols must follow evidence, not nostalgia. Evidence-based practice means using techniques proven to improve safety, comfort, and recovery.
⚡ Excuse #9: "Block can cause permanent neuropathy - not my surgery"
🔌That’s like blaming the electrician for the lights going out when you bulldozed the building.
📚 Fact: Permanent nerve injury from blocks is extremely rare (0.02–0.04%), often less than surgical or positioning-related injury. Proper technique and ultrasound guidance make blocks safer than most surgical retractors.
📜 Excuse #10: "Blocks are just a modern fad - we’ve managed patients for centuries without them"
⏳That’s like rejecting washing hands in surgery because “we managed without it in the 1800s.”
📚 Fact: Modern analgesia is about progress - fewer opioids, faster recovery, better function. History is for learning, not for limiting.
🎯 The Real Harm of a Block Ban
🤕 Unnecessary pain → slower rehab, higher opioids
💊 Opioid side effects → nausea, constipation, respiratory depression
🏥 Longer stays → more cost, fewer beds
🦵 Poor rehab participation → worse function
😔 Lower satisfaction → and they remember
💡 Bottom Line:
🎯Local anesthetics are the Swiss Army knife of perioperative care — analgesic, antimicrobial, anti-inflammatory, anti-edema, neuroprotective.
🎯Refusing them because of myths is like banning umbrellas because “rain helps plants grow.”
Yours (block) faithfully,
Dr. Local A. Nesthetic 🪄💉
🌧️ It's raining $NOTs and $DOGS!
Want a shot at sharing 5,000,000 $DOGS and 500,000 $NOT?
Simply:
🔸Follow & RT
🔸Fill in this survey form https://t.co/tJqyH2iDlx
#Binance Futures is thrilled to launch a giveaway with a total prize pool of 42,000 $BB up for grabs!
To enter:
🔸Make your first Futures trade
🔸Refer your friends to trade Futures
🔸Complete airdrop tasks to win up to 100 $BB
Join Now ➡️ https://t.co/H3YLM9gZ8y
"Spinal Showdown: Thoracic vs. Lumbar - What You Need to Know!"
#MedicalComparison#SpineHealth#SpinalAnesthesia#NeuraxialAnesthesia#SegmentalSpinalAnesthesia#ThoracicVsLumarNeuraxials#SpinalSafety#MedTwitter
My 10 Points:
A. PROS AND CONS
1. Thoracic spinal anesthesia
Pros:
a. Indications: Suitable for thorax, breast, and upper abdomen surgeries.
b. Less hypotension: Due to the higher injection level.
c. Obstetric suitability: For certain obstetric procedures like cesarean sections.
d. Lower volume requirement: Less required LA volume potentially reduces systemic toxicity risk.
e. It can explored in deformed or post-instrumented lumbar spines, especially for below umbilicus surgeries.
f. Suitable for segmental spinal anesthesia without involving lower roots.
Cons:
a. Limited anesthesia spread: Coverage is not as effective as lumbar spinal anesthesia.
b. Limited suitability: Not suitable for some lower abdominal, pelvic or lower extremity surgeries.
c. Risk of complications: Like PDPH and nerve damage, albeit rare.
d. Technical challenge: Requires precise injection technique due to smaller interlaminar spaces and angulated spinous processes.
e. Risk of spinal cord injury with untrained hands.
2. Lumbar spinal anesthesia:
Pros:
a. Indications: Surgeries below the umbilicus, including lower abdominal surgeries and lower limb procedures.
b. Technically easy: Due to the larger size of the lumbar spinal canal, wider interlaminar spaces, and less angulated spinous processes.
c. Offers flexibility in adjusting the level of anesthesia by selecting the appropriate lumbar interspace for injection.
d. Effective for surgeries requiring prolonged anesthesia, such as major orthopedic procedures.
Cons:
a. Increased risk of hypotension due to a larger volume of LA required and lower injection level.
b. Higher risk of complications such as PDPH and nerve damage compared to thoracic spinal anesthesia.
c. Not suitable for surgeries involving the upper abdomen.
d. Relatively contraindicated in deformed and post-instrumented spine.
e. Not suitable for segmental spinal anesthesia.
B. KNOW THE TARGET- EXITING NERVE ROOT
3. Thoracic Nerve Roots:
a. The thoracic nerve roots are smaller in diameter than the lumbar because thoracic nerves primarily handle sensory functions for the trunk and abdomen, with less motor function.
b. Consequently, compression or injury to these smaller thoracic nerve roots may lead to symptoms like chest or abdominal pain, numbness, or weakness, albeit potentially less severe due to their smaller size.
4. Lumbar Nerve Roots:
a. The lumbar nerve roots are thicker than the thoracic because lumbar nerves serve significant sensory and motor functions, controlling movement and sensation in the lower body.
b. This larger diameter can exacerbate symptoms in cases of compression or injury, potentially leading to more pronounced issues like leg pain, weakness, or numbness, commonly associated with conditions such as disc herniation or spinal stenosis.
C. CSF HOMEOSTASIS
5. CSF Volumes:
· The total volume in normal adults is 90-200 ml.
· 20% in ventricles and 80% in subarachnoid space.
· 50% Intracranial and 50% Extracranial.
· Total CSF volume in Spine = 81 ± 13 mL
Cervical - 19 ± 4 mL
Thoracic - 38 ± 8 mL
Lumbosacral - 25 ± 7 mL
· Average 5 ml of CSF/vertebral level with high individual variability.
6. CSF Pressure:
CSF pressure varies slightly depending on the spinal level when measured in the sitting position, with the pressure typically being lower in the lumbar region compared to the thoracic and cervical regions.
· Cervical region: 8 to 20 mmHg.
· Lumbar region: 6 to 15 mmHg.
· Thoracic region: 7 to 18 mmHg.
D. WHY IS PDPH LESS COMMON IN THORACIC SA?
7. Anatomical/physiological factors:
a. Less CSF pressure fluctuation between sitting and supine positions reduces the likelihood of CSF leakage and PDPH.
b. Lower CSF volume in the thoracic region minimizes the amount lost in case of dural puncture, reducing the risk of PDPH.
c. Reduced mobility in the thoracic spine lowers stress on the dural puncture site, decreasing the risk of CSF leakage and PDPH.
d. Thinner dura mater in the thoracic region is less prone to tearing, further reducing the risk of CSF leakage.
e. The thoracic spinal canal is narrower, making accidental punctures less likely to affect the dura mater and cause cerebrospinal fluid leakage.
E. WHY IS THINNER DURA LESS PRONE TO TEARING?
8. The dura mater is the tough outermost membrane covering the brain and spinal cord, and its thickness can vary depending on the region of the spine.
a. Greater elasticity: Thinner dura has more elasticity, flexing and deforming under stress instead of tearing outright, which absorbs mechanical forces and lowers the risk of tearing.
b. Less tissue to traverse: Thinner dura requires less force for penetration, reducing the likelihood of inadvertent tearing.
c. Less resistance to needle insertion: Thinner dura offers less resistance to spinal needle insertion, reducing frictional forces and the risk of tearing.
d. Lower structural stress: Thinner structures experience lower internal stresses, decreasing the risk of tears due to mechanical strain.
e. Faster healing: Thinner tissues often heal faster, reducing the risk of complications such as CSF leaks.
9. Why less paresthesia during thoracic spinal anesthesia?
a. Thoracic spinal nerves are thinner than those in the lumbar region, so they are less likely to be stimulated during needle insertion, reducing the likelihood of paresthesia.
b. Different nerve distribution: The lumbar nerves are larger and more densely packed than the thoracic nerves, so there is a higher chance of accidentally stimulating a nerve root, leading to paresthesia.
c. The thoracic spine is less mobile than the lumbar spine, making it easier to accurately insert the spinal needle without inadvertently contacting nerve roots, decreasing the likelihood of paresthesia.
d. The dura mater in the thoracic region is thinner than the lumbar region, making it less likely to impinge on nerve roots during needle insertion, reducing the risk of nerve stimulation and subsequent paresthesia.
e. Different Patient Positioning: During lumbar spinal anesthesia, the sitting position can place more stress on nerve roots and increase the likelihood of paresthesia. In contrast, the lateral decubitus or prone position during thoracic spinal anesthesia can provide better access to the spinal space with less nerve interference.
10. SAFETY:
a. Both thoracic and lumbar spinal anesthesia can be safe and effective when performed correctly by experienced practitioners.
b. However, lumbar spinal anesthesia may carry a slightly lower risk of complications due to anatomical differences.
c. As with any medical procedure, careful patient selection, proper technique, and close monitoring are essential to minimize risks and ensure patient safety.
Why TKA are more painful than THA?
#TKA#TKR#TKAPain#THA#THR#THAPain#RAinJointSx#MedTwitter#TKAvsTHA
My 10 Points:
1. More *Soft tissues* around Hip joint, to accommodate post surgical edema. It also support the hip joint by creating protective *Cushion* around joint.
2. Less soft tissues around knee joint, So postsurgical endema causes *tight compartment* around knee joint, stretching many painful structure.
3. Knee joint is more *complexly innervated* than Hip Joint. So, more nerves are involved in pain transmission.
4. Knee *surgery* is more complex than hip involving precise cutting of bones in various axes.
5. *Implant design* of TKA has many components increasing it's complexity. Multiple components subject to more wear & Tear.
6. *Weight bearing points* of hip joint involve only superior portion of acetabulum and posterosuperior portion of head of femur. So actual contact area during weight bearing is less, making it less painful during mobilisation.
7. During *weight bearing* all the interarticular surface of femur and tibia are involved. More contact area, more pain.
8. During *routine activities* , lots of movements occur in knee joint at various axes unlike Hip joint.
9. Entire weight of the body directly comes on the knee joint and equally distributed over all components. *Counter force* from the ground again gets focused on the knee joint, increasing it's *strain* .
10. *Post cementing inflammation* reaction is more in TKA due to use of cement on all femoral, tibial and patellar components. Also, more exposed articular surfaces compared to Hip joint.