This ridiculous statistic keeps appearing: medical errors are the third leading cause of death.
It is a powerful narrative that has spawned a massive quality-control bureaucracy.
It is also completely wrong.
Taking care of sick patients is not like flying an airplane. Pilots fly machines that have been maintained and cleared for takeoff. Doctors often take over when the plane is already on fire and heading toward a mountain.
Also, not every airplane is destined to crash. Yet, every patient is destined to die eventually.
When reviewers judge bad outcomes backward, they routinely classify the brutal, inevitable tradeoffs of medicine as preventable errors. Critically ill patients have more interventions and higher mortality. That does not mean an adverse event killed them, or that a new bureaucratic rule would have saved them.
The two papers often cited, one by the Institute of Medicine, another by Marty Makary, have substantial flaws. They often struggled to determine whether an adverse event actually caused the death. Shojania and Dixon-Woods, writing in BMJ Quality & Safety, criticized the “third leading cause” claim for exactly this reason. They argued that the estimate combined prior studies too simplistically, failed to follow accepted standards for quantitative synthesis, and did not adequately address whether the adverse events detected by review tools actually contributed to death.
In my latest essay, I explore how the exaggeration of preventable error has actively harmed patient care. The safety movement did not stop at identifying clear, recurring failures. It became a governing philosophy that gave administrators a moral language to control the clinical encounter.
Today, physicians spend hundreds of hours a year feeding quality metrics, hospitals game the data to manage their mortality statistics, and independent practices are crushed under the fixed costs of compliance.
When the metric becomes the target, institutions optimize for the metric. In some cases, like the push to reduce hospital readmissions, that optimization has actually caused more patients to die.
The honest path to patient safety begins by admitting that medical care involves dangerous tradeoffs, not deterministic guarantees. Read the full essay in the reply below.
This is a terrible idea.
Free primary care for all sounds great until you remember that free never means free.
It means the bill moves from the exam room to taxes and new bureaucracy hired to ration what politicians just promised was unlimited.
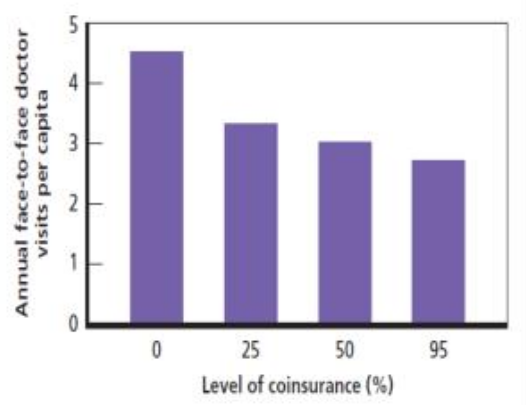
If car insurance covered tires at zero cost, demand would explode. People who truly needed tires would wait behind people getting upgrades because why not, it is free. Then the government would demand forms, approvals, documentation, denials, appeals, and entire departments to manage the mess.
More primary care visits do not automatically mean better health just as free tires don’t reduce car accidents. More spending does not automatically mean better care. And making primary care “free” does not make doctors, nurses, clinic space, time, or judgment magically materialize out of the ether.
It just removes price signals, politicizes what counts as essential, invites every interest group to lobby for inclusion, and leaves patients and physicians trapped under another layer of central planning.
If you want universal access for primary care, which I do, then just people the money. Primary care visits are cheap and the median American will spend less on those than on food. We have food stamps for the latter, so let’s make a type of food stamps for healthcare. Let patients and doctors decide what care is actually worth it for that individual instead of creating yet another government promise that doesn’t work out.
It's a little concerning that the head of a major health policy think tank treats the idea of "free primary care" as an accounting problem.
He fails to even acknowledge the second-order effects when you make a scarce resource "free" at the point of sale.
We have multiple studies (RAND, Oregon) and real-world examples (Canada) that show an increase in demand for healthcare when prices drop.
Nothing about this proposal increases supply, so you're inviting shortages.
So you'll need to manage utilization. That will require a bureaucracy. Now you're running a relatively cheap service (primary care visits) through a massive government bureaucracy which determines price, utilization, and access. This will increase the cost of the service, increase administrative burden for both doctor and patient, and decrease the overall quality.
And, of course, the people it's meant to help will be worse off. Those with connections or resources will circumvent the system. They'll pay cash for direct primary care (if that's still allowed) or use connections to jump in line.
Primary care needs more supply, more competition, and more direct patient physician relationships.
Not another layer of third party control dressed up as compassion.
Larry should know this.
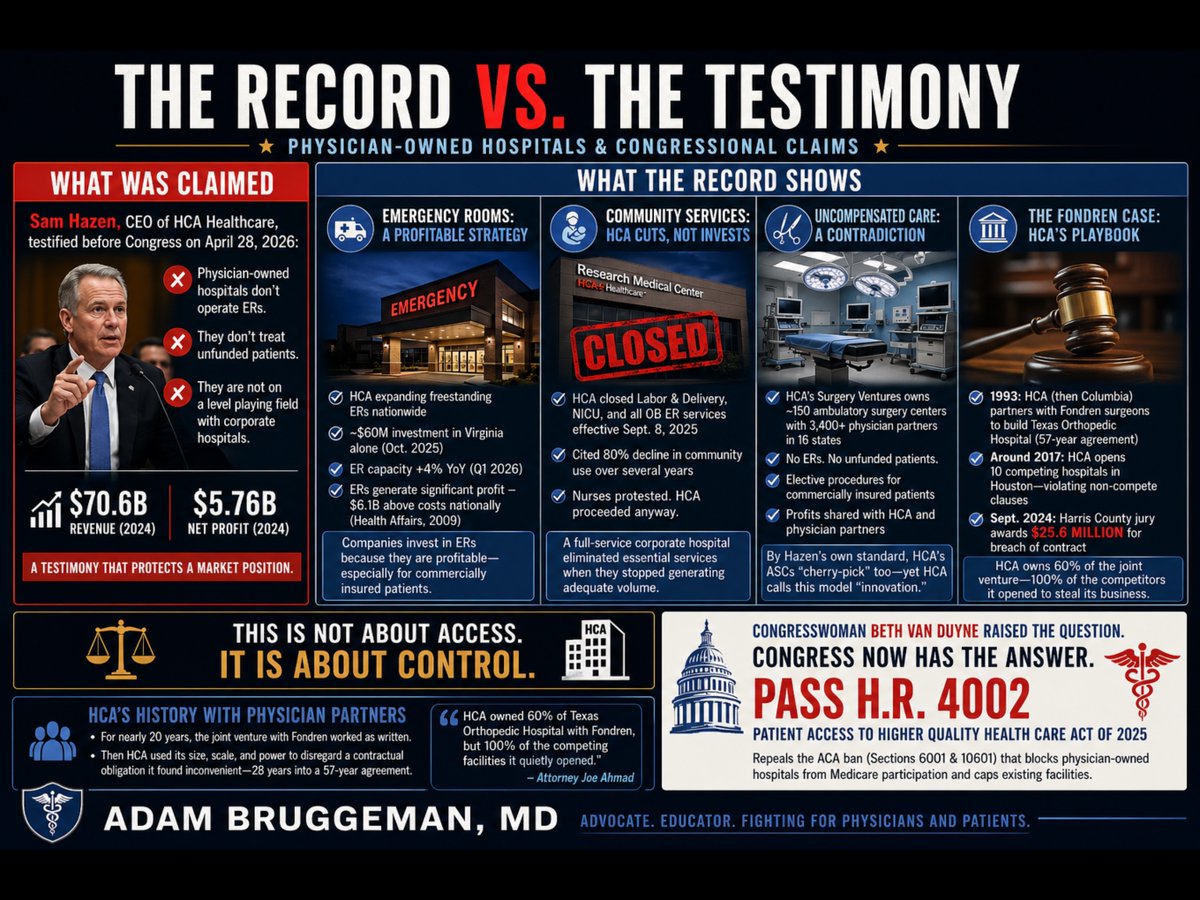
Yesterday, Sam Hazen, CEO of HCA Healthcare, sat before the House Ways and Means Committee and argued that physician-owned hospitals are not on a level playing field with corporate hospitals because they lack functioning emergency rooms and do not treat unfunded patients. Hazen delivered this argument while representing a company that posted $70.6 billion in revenue and $5.76 billion in net profit in 2024. He was not offering a neutral observation about healthcare access. He was protecting a market position.
Congresswoman Van Duyne did not let the testimony pass unchallenged. She pointed directly to HCA's own Research Medical Center in Kansas City, Missouri, which closed its labor and delivery unit, its neonatal intensive care unit, and all associated obstetrics emergency services effective September 8, 2025. HCA cited an 80 percent decline in community use of those services over several years as its justification. Nurses at the facility publicly protested the planned shutdowns and called on HCA to reverse course. HCA proceeded anyway. That is a full-service corporate hospital making a purely financial decision to eliminate essential community services when they stopped generating adequate volume. The same CEO who told Congress that physician-owned hospitals fail community obligations made that decision.
The emergency room argument deserves particular scrutiny. Mr. Hazen's implication is that operating an ER is a financial burden that justifies the premium reimbursement HCA collects across its outpatient system. The capital record contradicts that framing entirely. In January 2024, Hazen personally told HCA investors that the company's freestanding emergency room capacity would "grow consistently" in 2024 and 2025 to meet rising patient demand. In October 2025, HCA committed nearly $60 million to construct three new freestanding emergency rooms in Virginia alone, expanding its footprint there from eight to eleven standalone ER facilities. HCA has simultaneously been opening freestanding ERs in South Carolina, Florida, and throughout its other markets. In the first quarter of 2026, HCA reported that its emergency room capacity grew 4 percent year-over-year. A peer-reviewed analysis published in Health Affairs found that hospital emergency department revenue exceeded costs by $6.1 billion nationally as far back as 2009, a margin of 7.8 percent overall, with privately insured ED patients generating $17 billion in profit. Companies do not invest tens of millions of dollars in freestanding emergency infrastructure because that infrastructure is a burden. They expand aggressively into emergency care because it is profitable, particularly for commercially insured patients. When physician-owned hospitals choose not to operate ERs, they are not avoiding a community obligation. They are declining to compete in HCA's most profitable and most aggressively expanded service line.
The uncompensated care argument carries an equally significant contradiction. Through its Surgery Ventures division, HCA jointly owns and operates approximately 150 ambulatory surgery centers with more than 3,400 physician partners across 16 states. Those ambulatory surgery centers have no emergency rooms. They do not accept unfunded patients. They perform elective procedures on commercially insured patients and return profits to both HCA and its physician co-owners. By the precise standard Mr. Hazen applied to physician-owned hospitals before the Ways and Means Committee, his own company's Surgery Ventures facilities are doing exactly what he described as an unfair advantage. The distinction HCA is actually drawing is not between facilities that serve whole communities and those that do not. It is between facilities that HCA controls and those that it does not. When physicians own a hospital independently, HCA calls it cherry-picking. When HCA installs those same physicians as partners in ASCs under its corporate umbrella, it calls it innovative care delivery.
The history of how HCA treats physician partners outside of its direct control is documented in a Harris County, Texas courtroom. Fondren Orthopedic Ltd., a group of orthopedic surgeons, entered a limited partnership with what was then Columbia Hospital Corporation in 1993 to jointly own and operate Texas Orthopedic Hospital in Houston. The agreement ran for 57 years. For roughly two decades it functioned as written. Around 2017, HCA, which had assumed Columbia's position, began employing orthopedic surgeons at competing facilities across the Houston area, ultimately opening 10 competing hospitals offering the same services as the joint venture, in direct violation of the non-compete provisions of the partnership agreement. Simultaneously, HCA invoked those same non-compete clauses against the Fondren physicians, blocking them from doing what HCA was openly doing. In September 2024, a Harris County jury returned a verdict of $25.6 million against HCA for breach of contract. Lead attorney Joe Ahmad stated publicly that HCA owned 60 percent of Texas Orthopedic Hospital with Fondren, but 100 percent of the competing facilities it quietly opened to redirect patients away from their jointly held hospital. The jury found that HCA had the size, the scale, and the power to disregard a contractual obligation it found inconvenient, approximately 28 years into a 57-year agreement.
The legislative response is already written. H.R. 4002, the Patient Access to Higher Quality Health Care Act of 2025, introduced by Congresswoman Van Duyne and Congressman Henry Cuellar (D-TX-28), would repeal Sections 6001 of the Affordable Care Act, which banned new physician-owned hospitals from Medicare participation in 2010 and capped existing facilities at their March 2010 capacity. That ban was not derived from patient outcome data. It was a lobbying achievement. The evidence accumulated in the 15 years since passage shows that physician-led facilities consistently deliver care at lower cost with higher patient satisfaction than large corporate systems.
Thank you @RepBethVanDuyne for being a champion for patients, physicians, and communities!
The widening gap between "licensed" and "actually practicing" is the biggest driver of physician shortages.
Doctors are increasingly taking early retirement and/or leaving the field for non-clinical work because the practice of medicine has become so miserable.
This goes hand in hand with the death of independent practice.
Doctors who are employees have no reason to keep practicing if they have other means of financial independence. Doctors who have built practices and invested in their community, on the other hand, do continue to practice.
Restore independent physician practices to fix the doctor "shortage."
Maxim for my physician colleagues about the present state of healthcare:
Nobody's coming to help us. Act accordingly.
Grow.
Build.
Evolve.
Your patients need you to be more than just doctors.
We were trained to focus on singular effort, not scale. Take a page out of that playbook and learn to harness the power of systemic leverage. If we don't the system will continue to rend the profession limb from limb.
(It would also help if we didn't consistently kneecap each other.)
Let me help rephrase for you Bernie.
Need a loan for college so you can party for a semester and drop out? Taxpayers will loan you money for it.
Need an SBA loan for your business ? Taxpayers will guarantee it.
For a house ? Taxpayers will guarantee it. And local gov will give you money for your first down payment !
Get sick or are in an accident and you can’t afford your deductible, insurance company denied prescribed care or are uninsured ?
You are on your own 😤
Let me add Bernie, the one debt not a single one of us will ever pay off till the day we die ? Our health insurance premiums
And before you go in and on about single payer, ask @claudeai to take a look at your proposed Single Payer legislation.
You want the Sec of HHS to run it. You can’t have a political appointee run an apolitical position
And you expect every provider and doctor to accept whatever rate is set by Medicare. Big hospitals don’t know their costs. They couldn’t do a BOM for any procedure. They have negligible transparency.
If they don’t know their costs, and you don’t know their costs, how is it possible for taxpayers, caregivers and patients to get a fair deal ?
And the concept of “every other country does it “ ignores the fact that they all converted decades and decades ago, long before you and your peers allowed the extreme vertical integration we face now.
Which leads to the question. @BernieSanders , why have you not advocated for the Break Up Big Medicine Bill ?
Want to know the craziest part about insurance company Pre Authorization Denials ?
The insurance company defines the network of providers the patient can use
When they deny care, they are effectively saying "we don't trust the judgement of the doctors we require you to use" 🤯🤯🤯
“I hope I've demonstrated that you can face anything, you can face the end of your days, you can face hell with dignity. Fight, girls, and hold your heads high. Billie and Georgia, you are my heart, you are my everything. Goodnight. I love you.
Eric Dane leaves his daughters — and the world — with one final message in Famous Last Words.
2026 Medicare PFS: Independent Physicians Hit Harder Than Employed Docs—Fueling Consolidation
As we wrap up PFS week, here’s the through-line from what we’ve covered so far.
Monday:
The 3.26% conversion factor bump is temporary. There’s still no MEI-linked inflation fix, a new –2.5% “efficiency” cut to work RVUs, and practice-expense/site-of-service changes that widen payment gaps.
Tuesday:
The efficiency adjustment is deeply flawed. It ignores rising patient complexity, double-counts prior “efficiency” trims, and disproportionately targets procedural work RVUs (for example, many spine codes down 2–3%).
Wednesday:
CMS reallocated indirect practice expense in facility settings to 50%, further undervaluing office-based care. The same epidural pays roughly $250 in an independent office versus $750+ in a hospital outpatient department, rewarding hospital ownership and site shifts.
Today:
The uneven toll. Independent practices absorb the full impact of these changes, while employed physicians feel only part of it. Here’s how that plays out in the real world.
Employed Physicians
Most employed physicians are paid primarily on work RVUs. For them, the main hit is the –2.5% efficiency adjustment on procedures and surgeries. They generally do not experience practice-expense or site-of-service effects, because hospitals bill facility fees separately under OPPS. Recall that those payments receive annual MEI updates unlike physician fees.
The result for many employed physicians is relative stability, often buffered by hospital subsidies or compensation adjustments.
Independent Physicians
Independent practices are hit from every direction:
• work RVU cuts
• practice-expense reductions
• site-of-service differentials
For facility-based work common in spine and orthopedics, many codes see 2%–11% per-code reductions, translating to an overall payment decline of roughly 4%. Independent physicians can’t subsidize losses the way large health systems can. They have to survive on undervalued office rates while competing against hospital-owned practices paid at far higher total levels.
Examples (facility settings, non-QP CF):
• CPT 63047 (lumbar laminectomy): –2.69%
• CPT 63048 (additional segment): –8.49%
• CPT 27130 (total hip arthroplasty): –7.75%
Independent procedural specialists are hit hardest because higher facility volume means larger practice-expense losses. That pressure pushes more independents to sell or close.
The outcome is predictable. Independent practices disappear. Hospital employment expands (now 70%+ of physicians, per AMA data). Competition declines. Insurers negotiate with a few dominant systems. Costs rise. Access erodes. Patients wait longer for specialized care.
If policy continues to favor employment over independence, the question becomes simple: how do we preserve independent practice and patient choice?
“The happiness of your life depends upon the quality of your thoughts” Marcus Aurelius is trying to convey that a person’s happiness is determined primarily by how they think, not by external circumstances.
The nature, discipline, and moral quality of one’s thoughts shape how events are perceived and experienced. If thoughts are rational, virtuous, and well-ordered, life feels content and stable; if thoughts are negative, irrational, or uncontrolled, life feels unhappy regardless of outward conditions. According to him, happiness is an internal state governed by the mind, and improving one’s thoughts improves one’s life
@DrDiGiorgio I remember rotating on NSG as an ortho intern and the junior NSG resident carried 3 pagers, including the consult pager (AKA “the gimp”). Those things went off constantly and nobody envied that resident
One person's personal bias doesn't mean 24h shifts aren't useful. Just to counter this, I'm extremely grateful for my 24h shifts in medical school and residency. It absolutely helped me prepare, honed my ability to traige while exhausted, and made me a better doctor.
Oh, and 1-2x pages per hour is extremely low. Many neurosurgery residents get paged every 90 seconds for 24 hours straight. After that experience, there is literally no middle of the night phone call that a neurosurgeon can't handle.
You missed a few key facts.
1. physicians are underpaid under Medicaid and this results in physicians having to limit the number of Medicaid patients if they want to stay independent.
Why would Medicaid underpay the doctors and harm the patients?
2. Medicaid is full of non-medical programs and in MN 14 of those have been involved with an estimated $ 9 billiion fraud! We need to remove all non-medical programs from Medicaid.
3. Up to 90% of Medicaid is funded by the Federal government and the states manage the program.
This has led to massive fraud and we need to make Medicaid a federal program only.
4. There is massive fraud in Medicaid, and Centene has paid $1 billion in fines for overcharging the Medicaid program for drugs, but they are still allowed to participate in the program.
We need to simplify the program, pay physicians at commercial rates to allow them to care for these patients who deserve the best care.
President Trump has secured most-favored-nation pricing from 11 major pharmaceutical companies for Medicaid, and this will be very beneficial.
In fact, Eliquis will be free under Medicaid.
Before writing pieces like this, I recommend you talk with physicians who work with Medicaid patients like @DrDiGiorgio
Talking to independent physicians, it's obvious that the big insurance carriers are doing to them, what their PBMs are doing to independent pharmacies.
They deny, underpay, slow pay, clawback, and create administrative mazes, knowing their victims don't have the time or resources to fight.
Why ? By putting financial pressures on physicians and pharmacies, it makes them more likely to sell their businesses to them , close their doors, or refer the business to their captive pharmacy or provider. All benefitting the biggest insurance companies
We need to ditch the concept of "claims" and make every delivery of medications or care as a billable event that must, by law, be paid on a timely basis , with interest charges for any delays. If the physician or pharmacy doesn't deliver , the carrier has plenty of legal options already. As does the patient.
This is not an efficient market. This is the big guy abusing the little guy. It needs to change to better the care we get in this country
Breaking News: Independent doctors get a new advocacy group as skepticism of health giants grows
Today we launch a new group focused on the issues that matter to patients and the independent physician community.
We’re fighting for
• Physician Autonomy
• Fair Reimbursement
• Fixing the No Surprises Act
• Protecting practices against consolidation
Independent doctors deserve a voice. Now we have one. If you believe in independent medicine and the ways it will help to fix our healthcare system, join us today. It’s time to take back our healthcare system.
Read our @statnews exclusive story at
https://t.co/TEvZUFaco3
@IndeMedAction
Since both Michael DeBakey and burnout have come up recently, here are DeBakey’s thoughts on it (starting at ~29:00).
DeBakey said he “doesn’t make a distinction” between work and free time, and that he “doesn’t see the need for taking a vacation”. 🤔😬
https://t.co/GOMgHruMYH