A 30yo male with known LQTS on Nadolol travels to high altitude(3399mts).On his 4th day complains of lightheadedness and syncope of few seconds. Short bursts of this(B) are registered. Never underestimate the effects of high altitude on the cardiovascular system.
A 30yo male with known LQTS on Nadolol travels to high altitude(3399mts).On his 4th day complains of lightheadedness and syncope of few seconds. Short bursts of this(B) are registered. Never underestimate the effects of high altitude on the cardiovascular system.
How do you differentiate the athlete's heart from underlying cardiovascular disease? 🫀🏃
New EAPC/EACVI Clinical Consensus Statement provides practical guidance on exercise imaging from stress echocardiography to advanced multimodality imaging—to improve diagnosis, risk stratification, sports eligibility, and exercise prescription in athletes.
Read more: https://t.co/hvlueCObzc
#SportsCardiology #CardiovascularImaging #ExerciseImaging
@EJPCEiC@AboyansV@SilCastelletti@PTBuketAkinci@PeroneFrancesco@SMosteoru@TimKambic #EJPC
Building on the First Definition of Heart Failure, the Second Definition refines HF staging with sharper stage criteria, emphasizing early detection and individualized risk reduction and introduces the universal classification of HF causes, with explicit acknowledgment of geographic variation in HF risk and outcomes. https://t.co/YDuE4stb5s
This updated document provides a unified, internationally harmonized framework intended to standardize terminology. It addresses changes in disease manifestations, diagnostic strategies, and understanding of pathophysiology.
✍🏼 @MinnowWalsh@KarenSliwa@amibanerjee1@BiykemB@akshaydesaimd@DukeHFDoc@MKIttlesonMD@lamcardio@WilfriedMullens@NutritionHF
🫀 SPORTS CARDIOLOGY: what every cardiologist should know
New review just out 👉
Exercise is medicine… but not always harmless.
⚠️ Key message:
Sudden cardiac death (SCD) in athletes is rare (~1:50,000) but often the first manifestation of underlying disease
🔍 What really matters in practice?
1. Screening works (but not perfectly)
✔️ ECG-based screening can reduce SCD by up to 90%
❗ Still misses ~20% of conditions (e.g. coronary disease, fibrosis)
2. Athlete’s heart ≠ cardiomyopathy
The biggest challenge is NOT finding disease…
👉 it’s not overcalling disease
Physiological adaptations can mimic:
HCM
DCM
ARVC
LV non-compaction
➡️ Requires multimodality approach (ECG + imaging + exercise + genetics)
3. Red flags you should never ignore 🚩
Exertional syncope
Chest pain
Family history of SCD
Abnormal ECG (TWI lateral, ST depression, Q waves)
4. CMR is your best friend
👉 Especially when ECG is abnormal
👉 Detects fibrosis and subtle cardiomyopathy
(Yes… this aligns perfectly with what we see in ACM/arrhythmogenic phenotypes 👀)
5. Exercise prescription is evolving
❌ Old approach: “stop sport”
✅ New approach: shared decision-making
Some key points:
ARVC / desmosomal variants → avoid high-intensity exercise
Low-risk HCM/DCM → may still participate
Myocarditis → no sport for ≥3 months
6. The new frontier: master athletes 🏃♂️
↑ atrial fibrillation (3–5x)
↑ coronary calcium
↑ myocardial fibrosis
👉 Long-term effects still unclear
🧠 Take-home message
Sports cardiology is not about restricting athletes.
It’s about:
✔️ Identifying risk
✔️ Avoiding misdiagnosis
✔️ Enabling safe exercise
💡 My reflection:
This is exactly where imaging + genetics + phenotype integration becomes critical — especially in early/arrhythmogenic cardiomyopathies.
https://t.co/bQFlrEKZnS
Among patients with anterior myocardial infarction, adding low-dose rivaroxaban to dual antiplatelet therapy did not significantly reduce left ventricular thrombus formation at 1 month but increased minor bleeding.
https://t.co/lSxD7zhy3L
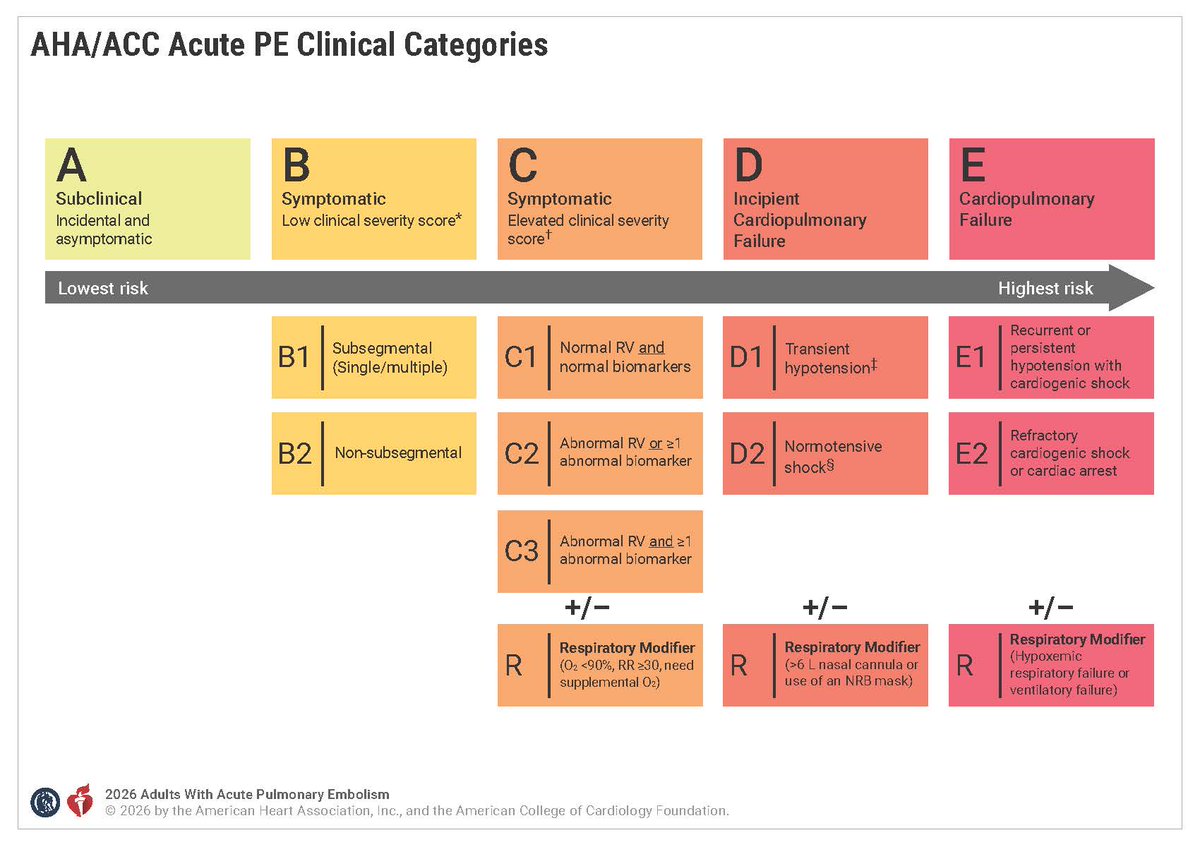
The 🆕 ACC/AHA Guideline for the Evaluation & Management of Acute Pulmonary Embolism (PE) in Adults is a de novo document offering comprehensive, evidence‑based recommendations for the evaluation, management & follow‑up of adults w/ acute PE.
Read more: https://t.co/koqYhnZVIz
⭕Ya disponible la nueva traducción al español de la Guía ESC 2025 sobre el manejo de la miocarditis y la pericarditis.
Descargártela:
https://t.co/ixDITXlAvr
@rafaelglezm@ICardiacaSEC@Smirabet1
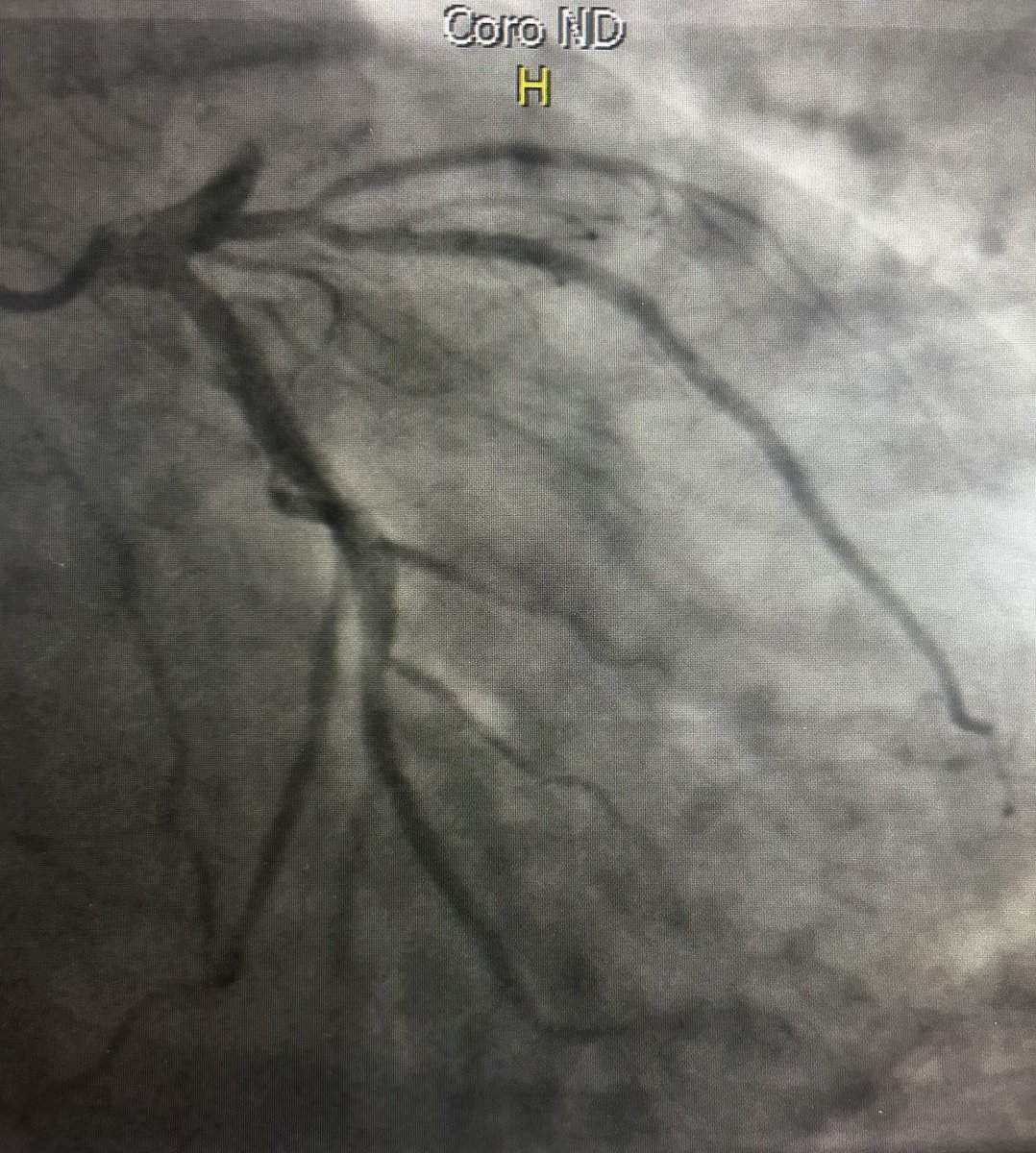
How often have you encountered simultaneous acute thrombosis of proximal RCA and LAD. 57yo M. Exercises regularly. No risk factors. Sudden onset of chest pain/syncope while motorcycling and at the top of a hill. Thoughts? @torresviera@DrRajeshG1@mmamas1973@Hragy@mandeep_mayo
🧵 Golden Thread: Dr Nishimura’s Stepwise Approach to Right Heart Catheterization - IVC / RA Entry
Step 1: Start in the IVC → RA
Advance & turn away from the hepatic veins. Obtain a venous sat early to exclude a major left-to-right shunt.
#ICSC2026
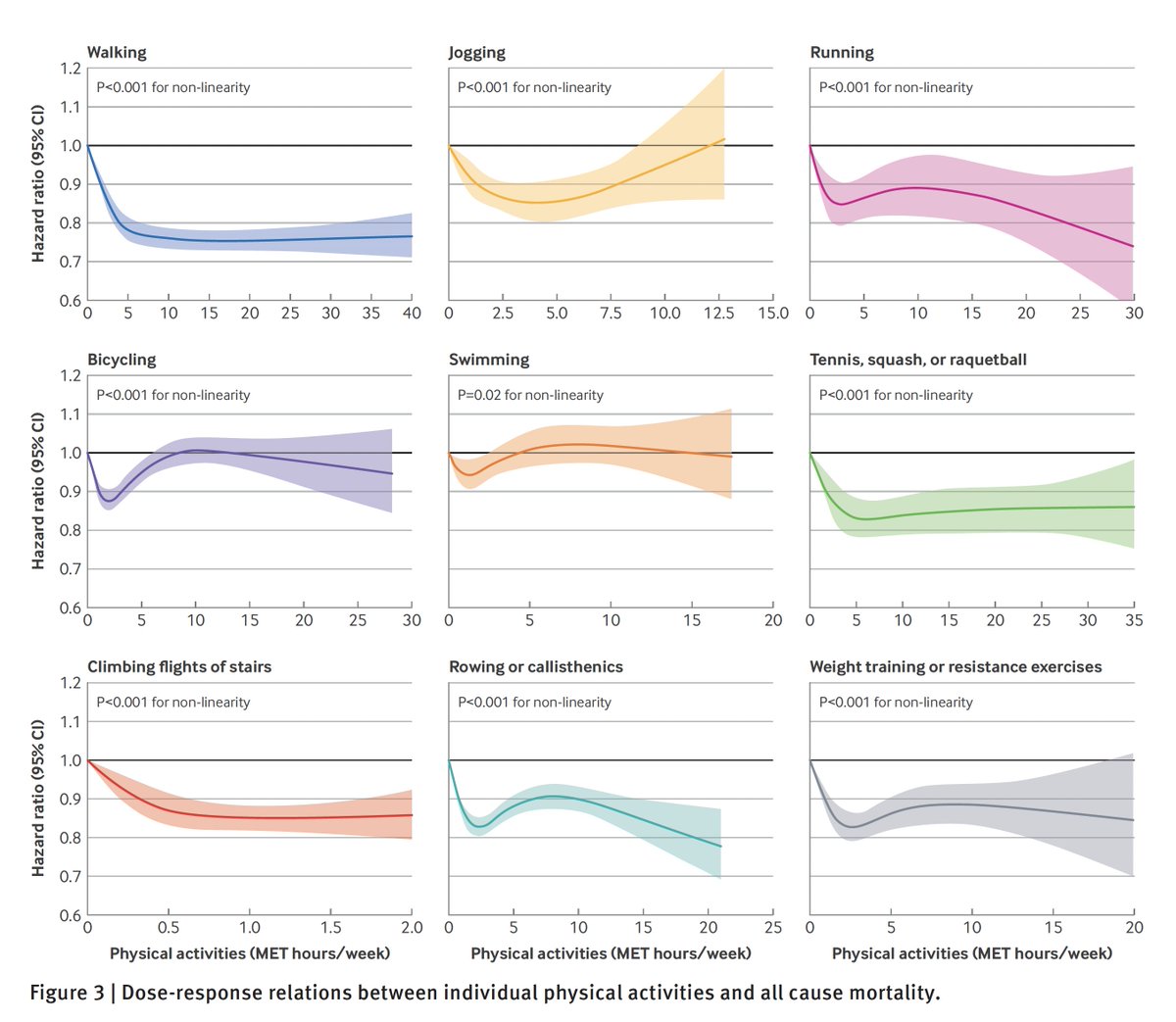
Physical activity and the reduction of all-cause mortality, from 2 very large prospective cohorts
1. The relationship is non-linear, suggesting a threshold effect for many types of exercise as seen below
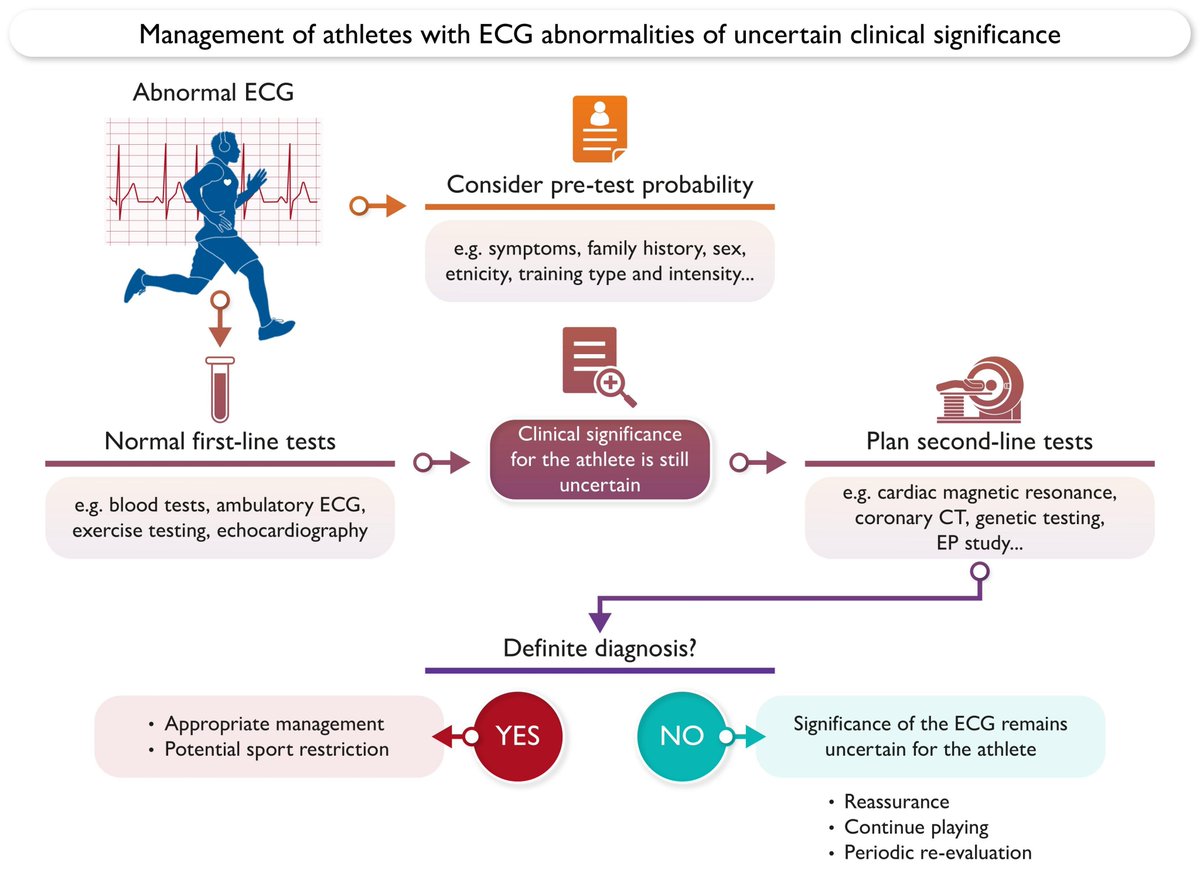
Abnormal electrocardiogram findings in athletes: A consensus statement of the European Association of Preventive Cardiology of the European Society of Cardiology
https://t.co/q2EdJPKWH5
#ECG#SCD#SportsCardiology
Get this: Coffee suppressed atrial fibrillation!
Unexpected results for recurrence from a randomized trial in participants after cardioversion from AF
#AHA25@JAMA_current ☕️ https://t.co/70dPI2R84C