A case of ischemic MR.If there is a 90% lesion in mid part of dominant LCX with other vessels normal,what is the management option?(A) CABG with MV repair (B) PTCA to LCX and watch regression of MR (C)PTCA to LCX followed by Mitra clip later (D) CABG with mitral valve replacement
A case of ischemic MR.If there is a 90% lesion in mid part of dominant LCX with other vessels normal,what is the management option?(A) CABG with MV repair (B) PTCA to LCX and watch regression of MR (C)PTCA to LCX followed by Mitra clip later (D) CABG with mitral valve replacement
A low-cost and expert-driven medical technology is being used in rural areas in Australia!
The machine is operated by a sonographer remotely (using a gaming controller) and helps perform an ultrasound examination.
Doctor shortages shouldn't mean that patients have to travel more (sometimes for no medical reason), but to use technologies that can extend the reach of medical care.
This is a perfect example of that!
Proximal CAP AMBIGUITY even in the presence of a STENT .. ISR CTO ..
Nature finds a way , the epicardial collaterals have formed just around the stented segment just like a moneyplant grows over a thread trail ..
Important question
Should we even open this CTO , which in all possibilities have 25% chances of reocclusion over less than 10 years , or just give medical therapy a chance now since we know these bridging epicardial collaterals are resistant to atherosclerosis and will never close down antegrade flow ..
#CTO #Cardio_X #CardioTwitter
#cardiology
#Sharing is learning
Mistakes are powerful but costlier teachers.
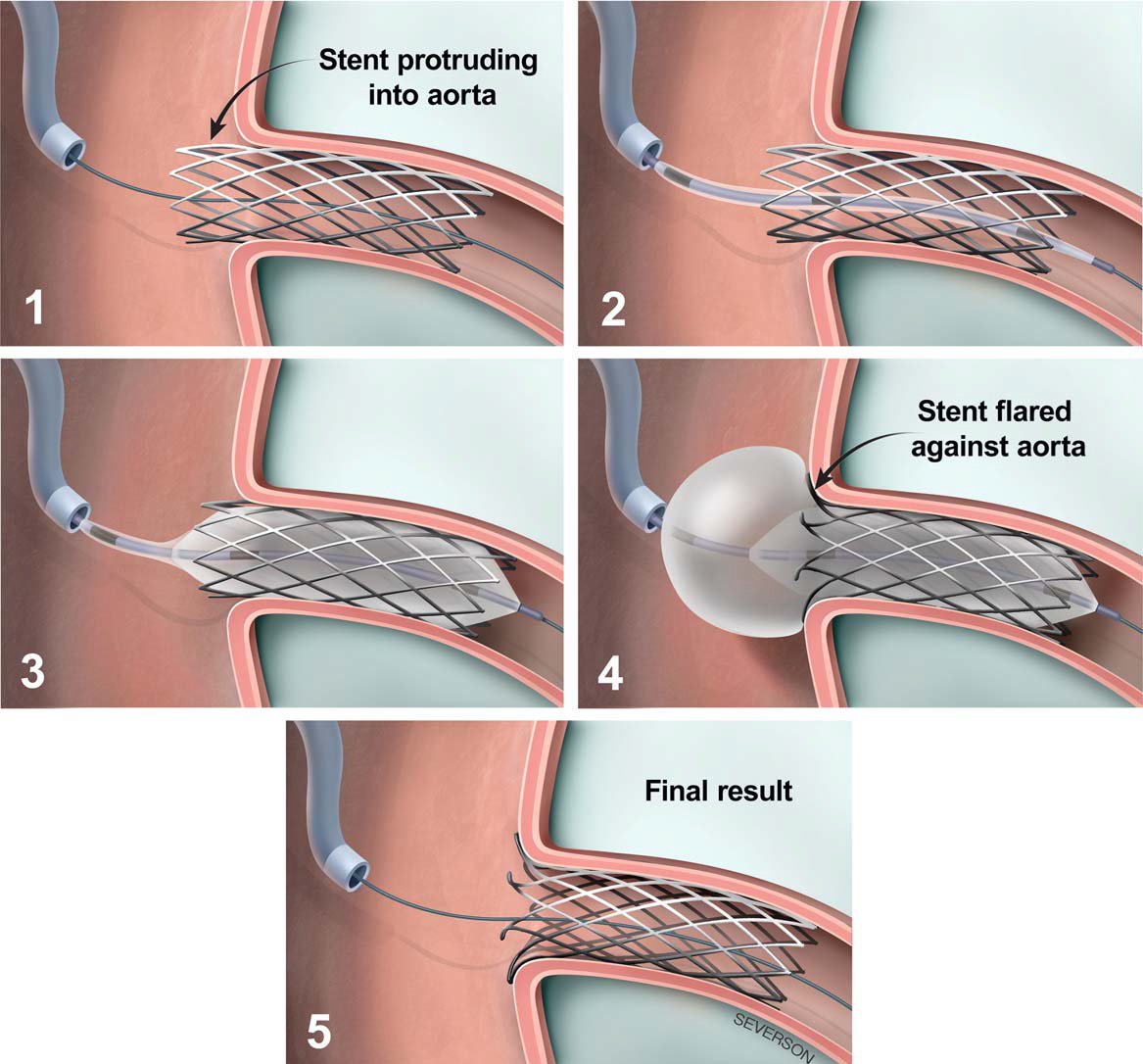
Why it was happened ?
It was a chance or certain??Prevention?
Following strict protocols can prevent the majority of embolizations. Rules are safeguards, not barriers—double-check before any device release.
Life is precious.
I follow some protocols—what do you all follow? Share your insights! #SafetyFirst #LearnFromMistakes
Run of the mill case , real world scenario ..
IWMI , CHB , poor hemodynamics at this time of CAG video .. BP in 80's ..
Q. What next is considered the next best line of treatment here , as u wud do it in ur practice ?
1. Its either a distal edge dissection of IMH , Just Cover with Another DES quickly ..
2. May be spasm , increase inotropes and give NTG via MC or ruptured balloon ..
3. image it and try to assess what is happening and then treat accordingly ..
#cardiotwitter #medtwitter
Why I love cardiology.Straight from the cath lab right now and a big thanks to Almighty straight from my heart. From nothing, no flow, no BP, low saturation intubated, poor pt couldn’t afford even an IABP balloon, IC adrenaline for severe no reflow and adrenaline surge for myself