🫀 The Most Dangerous Moment in the ICU May Last Less Than 60 Seconds
We often think of tracheal intubation as an airway procedure. Physiologically, it is a profound cardiovascular intervention.
Why Do ICU Patients Crash During Intubation?
The problem begins before the laryngoscope enters the mouth.
Many critically ill patients survive on a fragile compensatory state characterized by:
🔹 Endogenous catecholamine surge
🔹 Tachycardia
🔹 Vasoconstriction
🔹 Increased myocardial oxygen demand
What appears to be "stable" hemodynamics may actually represent physiological exhaustion.
The moment induction drugs are administered, this compensatory sympathetic drive disappears.
The result? A sudden reduction in:
• Systemic vascular resistance
• Cardiac output
• Coronary perfusion pressure
• Organ blood flow
This phenomenon has been termed adrenergic collapse.
Intubation Is a Hemodynamic Timeline
The authors propose viewing intubation as a sequence of cumulative threats rather than a single procedure:
1️⃣ Pre-induction adrenergic dependence
2️⃣ Sympatholysis after induction
3️⃣ Apnea, hypoxemia, hypercapnia, and acidosis
4️⃣ Transition to positive-pressure ventilation
5️⃣ Post-intubation ventilator and sedation effects
Each phase adds physiological stress.
Together, they can culminate in cardiovascular collapse.
The Propofol Question
One of the most clinically relevant findings is the growing evidence regarding induction agent selection.
In the INTUBE cohort, propofol was associated with a higher risk of cardiovascular collapse and was the only modifiable risk factor consistently identified.
The review therefore suggests:
✅ Ketamine
✅ Etomidate
as preferred induction agents in patients at risk of hemodynamic instability, while propofol should be used cautiously in shock states.
Positive Pressure Ventilation: The Forgotten Hemodynamic Challenge
Once the tube is secured, many clinicians relax.
The physiology is only beginning.
Positive-pressure ventilation:
🔹 Reduces venous return
🔹 Increases intrathoracic pressure
🔹 Raises right ventricular afterload
🔹 May precipitate right ventricular failure
This is particularly relevant in ARDS, pulmonary hypertension, pulmonary embolism, and severe hypoxemic respiratory failure.
Reference 📚
Kotani Y, Koroki T, Hayashi Y, Russotto V. The hemodynamics of tracheal intubation in critically ill patients: a narrative review. Journal of Intensive Care. 2026;14:42. DOI: 10.1186/s40560-026-00877-4.
Our reaction to any new study is either “I don’t believe it” or “I knew it”...
A NEJM trial in ICU pts w acute resp failure found that mucolytics (carbocisteine & hypertonic saline) don’t help. My ICU rounds line “mucolytics are useless” may need an update: “and possibly harmful”
Lung Volumes & Capacities: The Clinical Story Behind the Numbers
Most students memorize:
TV = 500 mL
FRC = RV + ERV
VC = IRV + TV + ERV
TLC = VC + RV
…and then forget why any of it matters.
The USMLE, ICU, anesthesia, ENT airway management, sleep medicine, pulmonary medicine, and emergency medicine all care about these numbers because they describe what the lungs are physically capable of doing.
Think of the lung as a reservoir.
TV = what you normally use
IRV = emergency reserve above normal
ERV = emergency reserve below normal
RV = untouchable reserve that keeps alveoli open
Everything else is built from these.
---
Case 1: The Healthy Medical Student
A 24-year-old MBBS student is sitting quietly studying.
He breathes normally.
Each breath:
≈ 500 mL
This is:
Tidal Volume (TV)
Definition:
Air entering and leaving lungs during quiet breathing.
Normal:
≈ 500 mL
≈ 6–8 mL/kg
Why this matters
Ventilators are initially set using tidal volume.
ARDS guidelines:
6 mL/kg ideal body weight.
Too high:
volutrauma
barotrauma
pneumothorax
Too low:
hypoventilation
hypercapnia
USMLE favorite:
> Tidal volume remains relatively preserved early in many lung diseases.
---
Case 2: The Athlete Sprinting for a Bus
Same student misses his bus.
Now he takes a huge deep breath.
The air he inhaled beyond normal inspiration is:
Inspiratory Reserve Volume (IRV)
Definition:
Extra air inhaled after normal inspiration.
This is your pulmonary "backup tank."
Why it matters
IRV falls in:
Pulmonary fibrosis
Severe obesity
Pregnancy
Kyphoscoliosis
Reason:
Lungs cannot expand properly.
USMLE clue:
"Difficulty taking a deep breath"
Think reduced IRV.
---
Case 3: COPD Smoker
65-year-old smoker.
He says:
> "Doctor, I can't empty my lungs."
This is not primarily an inspiration problem.
It's an expiration problem.
Air trapping occurs.
After normal expiration he still has excessive air left.
ERV decreases.
RV increases.
This is classic COPD physiology.
---
Expiratory Reserve Volume (ERV)
Definition:
Extra air that can be expired after normal expiration.
Normal person:
Can force out a lot more air.
COPD patient:
Already trapped.
Little reserve remains.
ERV decreases.
Real-world consequence
Difficult extubation.
Difficult anesthesia.
Postoperative hypoventilation.
---
Case 4: The Asthmatic in the ER
28-year-old arrives with severe wheeze.
Chest hyperinflated.
Prolonged expiration.
Air trapping.
Large amount of gas remains inside lungs after maximal expiration.
This is:
Residual Volume (RV)
Definition:
Air remaining after maximal expiration.
Physiological purpose:
Keeps alveoli from collapsing.
Without RV:
Every breath would require reopening millions of alveoli.
Energy cost would be enormous.
---
Why RV is clinically important
RV increases in:
Asthma
COPD
Bronchiolitis
RV decreases in:
Pulmonary fibrosis
USMLE pearl:
RV is one of the few volumes that cannot be measured by simple spirometry.
Because you cannot exhale it.
---
High-Yield Exam Question
Which lung volume cannot be measured directly by spirometry?
Answer:
Residual Volume
Therefore any capacity containing RV also cannot be measured directly.
---
Case 5: The Post-Thyroidectomy Patient
ENT correlation.
After thyroidectomy a patient develops bilateral RLN palsy.
Breathing becomes shallow.
Inspiratory effort weak.
The amount of air inhaled after normal expiration falls.
This is:
Inspiratory Capacity (IC)
IC = TV + IRV
Definition:
Maximum air inspired after normal expiration.
Clinical importance
Reduced in:
Vocal cord paralysis
Neuromuscular disease
Myasthenia gravis
Guillain-Barré syndrome
Patients often describe:
> "I can't take a satisfying breath."
1/2
THE CELL THAT GIVES ITSELF AWAY
A single megakaryocyte can give rise to 1,000–3,000 platelets.
But not all at once.
And not exactly one at a time.
It spends days becoming enormous.
Then, in its final act, it extends branching proplatelet processes into marrow sinusoids.
Geriatrics is an interesting branch, if your 80 year old patient with uncontrolled sugars want to eat mangoes, you don’t refer to literature and tell her not to eat mangoes. On the contrary, you use wisdom and try to find out how can you enable her to do that!
#Geriatrics#medX
Today's trainees pale in comparison
Dr Harrington, a fellow at WashU, thought ITP was due to a blood factor that caused destruction of platelets
To test hypothesis he took 500 cc 🩸 from a pt with ITP, injected it into himself, ended up hospitalized with severe thrombocytopenia
A patient comes back with a second stroke.
We immediately start looking for a culprit: carotid stenosis, atrial fibrillation, uncontrolled diabetes, resistant hypertension.
But we never ask a different question:
Did the stroke recur because the treatment failed, or because the treatment never truly reached the patient?
The medicines were prescribed, but later stopped. The BP machine was never bought. Follow-up was missed because the hospital was far away. Rehabilitation was recommended but inaccessible. The caregiver was exhausted. The patient never understood that stroke prevention is a lifelong commitment.
We spend a lot of time looking inside the artery.
Perhaps we should spend a little more time looking outside the hospital gate.
Because a perfect prescription does not prevent stroke.
A prescription that a patient can actually follow does.
Social Determinants of Health and Their Impacts on Stroke Prevention and Outcomes. #Neurotwitter #MedX, #Strokecare
It all comes down to a pharmacological concept called "Selective Toxicity"...the ability to kill the bug without killing the patient.
• Bacteria are independently living organisms. They have their own unique cellular machinery, like a cell wall, that human cells don't have. Because their biology is completely different from ours, we can easily design antibiotics that act like a targeted sniper. They destroy the bacteria while completely ignoring your healthy cells.
• Viruses are entirely different. They are obligate intracellular parasites. They don't have their own machinery to survive. When a virus enters your body, it physically invades your healthy cells and hijacks your own human DNA/RNA polymerases to multiply. Because the virus is using your cellular machinery, any drug designed to destroy it risks poisoning your own human cells in the process.
• "But wait, don't we have antivirals for things like HIV, Herpes or the Flu?"
Yes. But to make those, scientists spent decades and billions of dollars to find one unique viral enzyme (like reverse transcriptase or protease) that we could target without killing the host.
• For a mild, self-limiting infection, the only safe, highly targeted drug that can destroy the infected cells without wiping out the healthy ones is your own immune system.
👉Hi, I am Dr. Priyam. I break down complex medical science and advocate for Evidence-Based Medicine. Follow me for more clinical breakdowns.
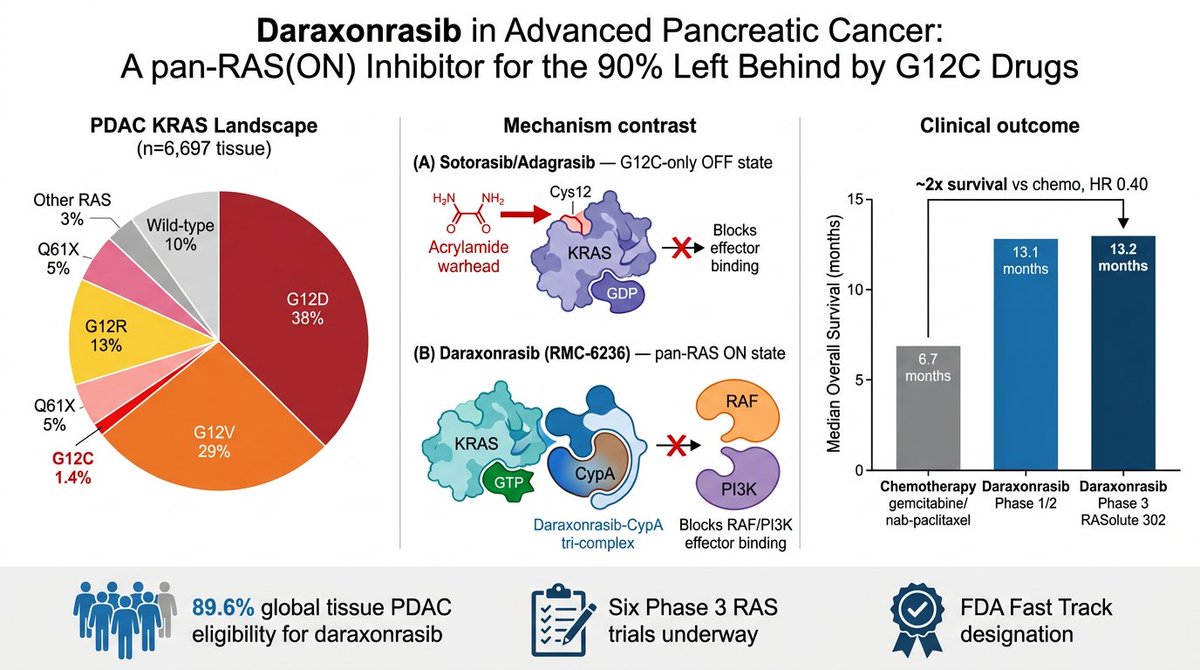
One of the most amazing things I’ve ever seen: a standing ovation for the full Daraxonrasib results
I feel inspired and energised, to put it mildly — we have a targeted therapy for pancreatic cancer now, and nothing is undruggable anymore
RAS finally getting drugged is one of the great stories in modern biology, and almost nobody outside oncology understands why it's such a big deal.
YOU'LL LEARN SOMETHING AWESOME TODAY.
i am going to keep this as understandable (and simple) as i can.
OPEN THE THREAD.
🧵
Let me trace the timeline here because nobody's connecting it.
Step 1: Scrape the entire internet. Every book, every article, every conversation, every piece of art, every forum post. Do it without asking. Do it without paying.
Step 2: Train a model on all of it. Call it "artificial intelligence."
Step 3: Go to BlackRock's Infrastructure Summit and announce: "We see a future where intelligence is a utility, like electricity or water, and people buy it from us on a meter."
Step 3 is where you sell people's own knowledge back to them. On a meter.
They took the collective output of human thought, compressed it into a model, and now they want to charge you by the token to access a version of what you and everyone you know already created.
One Reddit user put it perfectly: "They stole all this data from us, the people, our life's work, creativity, art, by devouring the internet and blowing through all copyright laws. Now they want to sell it back to us in the form of a utility."
Imagine if someone photocopied every book in the public library, burned the library down, and then opened a subscription service for the copies.
That's the metered intelligence business model.
And they're pitching it to infrastructure investors as though they invented water.
Topiramate vs. Candesartan: What the Data Shows.
Topiramate became one of the most prescribed migraine preventives for a reason that has little to do with efficacy: it causes weight loss. For a condition that disproportionately affects women, that side effect made topiramate acceptable in a way its actual profile doesn't justify.
The profile has a list of significant side effects. Cognitive impairment bad enough that patients call it "Dopamax." Memory loss, word-finding difficulty, kidney stones, osteoporosis, and metabolic acidosis. Birth defects, including cleft palate and low birth weight.
Migraines are most common in women between 18 and 44. Half of all pregnancies in the United States are unplanned. I think every woman of childbearing age prescribed topiramate must know about that risk before she fills the prescription. Many don't get this information.
I stopped using topiramate as a first or second choice years ago. A new study from the Leiden Headache Center confirms that this was the right choice.
They studied 661 migraine patients, comparing candesartan versus topiramate.
Within six months, 67% of topiramate patients had stopped taking it. For candesartan, 30%. That gap is tolerability in the real world. The 50% responder rate was also higher with candesartan: 47% vs 29% for topiramate.
Candesartan is a blood pressure medication in the ARB family. Beta blockers, the oldest preventive migraine drugs, also work through the cardiovascular system, but they slow the heart rate and make exercise harder. Candesartan does not do that, which matters for most patients.
Topiramate is FDA-approved for migraine prevention. Candesartan is not. By standard evidence-based logic, topiramate comes first. But two-thirds of patients stopped taking it within six months. FDA approval tells you which drugs have been studied in industry-funded trials. It does not tell you which drugs patients can tolerate, or which ones produce better outcomes when you follow real people over time. This study does that, and candesartan wins clearly.
The authors call for guidelines to be revised. Patients should not be steered toward a drug with this side effect profile simply because it has regulatory approval and candesartan does not.
54-year-old postmenopausal lady.
Persistent itching over skin.
“Sand/gritty” feeling in eyes.
LFT:
SGOT 40
SGPT 67
ALP 190
This is where many people stop at “fatty liver”.
But the pattern matters.
Middle-aged woman + cholestatic enzymes + sicca symptoms should immediately trigger another thought process:
Autoimmune liver disease?
Primary biliary cholangitis?
Sjögren’s overlap?
Pruritus can precede jaundice by YEARS.
Now the real work starts:
• Repeat complete LFT with GGT
• ANA, AMA-M2, ENA profile
• IgM levels
• Thyroid profile
• Ultrasound liver/biliary tree
• Evaluate dryness properly:
Schirmer test
Oral dryness
Parotid enlargement
Dental caries
Not every “itching + mild LFT elevation” is dermatology or fatty liver.
Sometimes the liver whispers before the autoimmune disease declares itself.
@docakx@IhabFathiSulima
Clinical quiz
🔸56 year old man was generally having a good time with his childhood friends. Spirits were high and they were reminiscing their old days. Jokes were cracked one after another, and he was laughing non-stop.
🔸Out of the blue, he collapsed on the sofa. When his friends tried to call him, he did not respond. His eyes were closed and he lied there motionless.
🔸His pulses were feeble, however, he was breathing. His friends panicked. One of them rushed to call a doctor, someone else tried sprinkling water on his face.
🔸After about a minute or so, they were relieved to see that he opened his eyes, regained consciousness and was able to move again. However, he didn't have any memory of the incident.
🔸This was the first such episode in his life. He had hypertension and his BP was well controlled on medications. He had no other illness.
❓What went wrong with this gentleman?
There are a lot of myths and untruths regarding IV thrombolysis (IVT) for acute ischemic stroke which I’ve been encountering frequently. Below is a thread discussing some of the more common ones.
#neurology#stroke#tPA#TNK#neuroX#MedEd#medschool#FOAMed