some says #POCUS answers (to the basic #FICE#CUSIC#FAMUS questions) are binary: yes/no.
but imo there must be 3:
- yes
- no
- i don’t know
3rd is not cool, but absolutely valid and most importantly: safe
May Airway of the Month:
https://t.co/pKmvr8ti4Z
the tube misses by a millimeter — but the problem may have started before tube passage.
This month: suboptimal VL view, arytenoid engagement, and the key reset:
Back up → suction → optimize laryngoscopy → reattempt.
#FOAMed #Airway #EmergencyMedicine
How the blood goes round sounds simple. It isn’t.
• Pressure does not drive flow.
• Preload is not a driver of cardiac output.
• Equations and graphs describe a system without explaining what controls it.
• Flow is governed by two constraints: delivery and acceptance.
Now free to read for a limited time:
Energy, flow and pressure in the cardiovascular system: a narrative review of how the circulation works
Link in reply 👇
https://t.co/1Oa5uJkOGH.
🫀POCUS is no longer just a bedside imaging tool.
It is becoming real time physiological intelligence.
This excellent 2026 review highlights how modern POCUS is expanding into:
• ultrasound guided regional anesthesia
• shock and cardiac arrest management
• AI assisted imaging
• advanced diagnostics
• governance and medicolegal practice
Some of the most provocative concepts: • “Occult VF” detectable only on echocardiography during cardiac arrest
• Ultrasound guided CPR compression positioning
• AI assisted lung ultrasound acquisition by nonexperts
• Handheld devices approaching cart based diagnostic performance
One important medicolegal message: several lawsuits involved failure to perform POCUS when clinically indicated.
The future of emergency and critical care medicine will likely depend on clinicians capable of integrating: physiology + imaging + AI + rapid bedside decision making.
POCUS is not anymore an “optional skill” but “core clinical infrastructure.”
Mani N, Rao S, Kim DJ. Point-of-care ultrasound in the modern era of emergency medicine: a narrative review of the recent literature. Curr Opin Crit Care. 2026. doi:10.1097/MCC.0000000000001358
🫁COPD ventilation is not ARDS ventilation.
In acute COPD exacerbation, the enemy is often not alveolar collapse. It is expiratory flow limitation, dynamic hyperinflation, intrinsic PEEP, respiratory muscle overload, and CO₂ retention.
Recent PubMed indexed literature from 2023 to 2026 reinforces a practical message: in acute hypercapnic COPD exacerbation, NIV remains the first line ventilatory strategy when there is respiratory acidosis, increased work of breathing, and no immediate contraindication (Farmer et al., 2024; Mein & Ferrera, 2025). HFNC may be useful in selected patients, especially when NIV is not tolerated, but recent meta analysis suggests higher treatment failure and crossover to NIV, so it should not replace NIV as default support in acidotic AECOPD (Qin et al., 2025).
The invasive ventilation strategy is different from hypoxemic lung disease.
For the intubated COPD patient, the goal is not to normalize PaCO₂ quickly. The goal is to reduce dynamic hyperinflation.
That means:
Low respiratory rate
Long expiratory time
Modest tidal volume, usually around 6 to 8 mL/kg predicted body weight
Avoidance of excessive minute ventilation
Permissive hypercapnia when pH is acceptable
Monitoring plateau pressure, driving pressure, auto PEEP, expiratory flow, and hemodynamics
PEEP is the controversial part.
External PEEP can help when the patient is spontaneously triggering, because it reduces the inspiratory threshold load caused by intrinsic PEEP. In this context, carefully applied external PEEP may improve synchrony, reduce work of breathing, and facilitate assisted ventilation (Jubran, 2024).
But in controlled ventilation without spontaneous effort, excessive external PEEP may worsen hyperinflation, raise plateau pressure, reduce venous return, increase RV afterload, and precipitate hypotension. Here, low PEEP or minimal PEEP may be safer unless oxygenation requires more support.
A practical bedside rule:
If the COPD patient is triggering and fighting auto PEEP, external PEEP may help.
If the COPD patient is passive, hypotensive, hyperinflated, and not oxygenation limited, high PEEP may harm.
The ventilator question is not:
“How much PEEP does COPD need?”
It is:
Is PEEP unloading the patient, or inflating the trap?
#COPD #CriticalCare #ICU #MechanicalVentilation #NIV #AutoPEEP #Hypercapnia #RespiratoryFailure #VentilatorManagement #IntensiveCare
References📚
*Farmer, M. J. S. Chest, 165(6), 1473–1483. https://t.co/ZgblBs1ZZK
*Jubran, A. Current Opinion in Critical Care, 30(1), 89–96. https://t.co/JKkchvgKDj
*Mein, S. A. CHEST Critical Care, 3(1), 100107. https://t.co/tO69w9ahnl
*Qin, J., Annals of Intensive Care, 15, 64. https://t.co/ay4Wgxbpai
Haemodynamic equations are useful. But they also mislead.
Take:
CO = HR × SV
CO ≈ (MAP − RAP) / SVR
Both are mathematically true. But they can make the variables they contain look like the controllers of output.
Often they are not.
In the intact circulation, these equations describe the resolved state of the system. They do not, by themselves, tell you what is supplying energy, what is constraining flow, or what is actually limiting output.
That is one of the central themes of our review:
Energy, flow and pressure in the cardiovascular system: a narrative review of how the circulation works.
https://t.co/L19bsDCzr6
We did it!!!
Completed the Vogalonga 2026 with our 3 boys! I am incredibly proud of them and my wife!
Thank you very much for all the donations for @SandcrossSchool .
https://t.co/IPx62cLdKh
Also huge thanks for our tour leader Tamas Kakas! We’ll come again ;)
Fundraising for Friends of Sandcross Charity!
Our family of five will participate in a 30km kayaking regatta
We are raising funds for the boys’ school: @SandcrossSchool to improve their outdoor learning space.
Please consider supporting our goal!
Link in the next post:
🫀🤓Pressure does not move blood. Energy does.
This outstanding review challenges one of the most deeply rooted concepts in haemodynamic management: the idea that pressure variables are the primary drivers of circulation. Instead, the authors propose a physiology framework where the heart supplies energy, the vasculature defines constraints, and pressures merely reflect system state.
Several concepts deserve special attention for critical care clinicians:
• Mean systemic pressure does not “drive” flow
• Right atrial pressure is a dependent variable, not a therapeutic target
• Venous return depends on inflow acceptance and inlet impedance
• Raising pressure without improving flow may worsen congestion
• Shock should be interpreted as either impaired venous delivery or impaired cardiac acceptance
Clinically, this framework helps explain why:
• CVP-guided fluid loading often fails
• Vasopressors may normalize MAP without restoring perfusion
• Congestion can coexist with preserved arterial pressure
• Flow responsiveness matters more than static pressure targets
One of the strongest messages of the paper is simple but powerful:
“Pressure is not perfusion.”
For intensivists, anesthesiologists, and cardiogenic shock teams, this review is worth reading in full. It reconnects bedside haemodynamics with first-principles physiology.
Miller A, Anaesthesia. 2026. https://t.co/ejjvREUe7c
🫀Valvular cardiogenic shock is probably one of the most underrecognized phenotypes of shock in modern cardiac critical care.
What makes this paper particularly important is that it reframes severe valve disease:
not as chronic structural cardiology, but as acute hemodynamic catastrophe.
The physiology is brutal.
Unlike classic ischemic CS, VCS often combines:
🫀 abrupt preload overload
🫀 severe afterload mismatch
🫀 elevated filling pressures
🫀 pulmonary edema
🫀 impaired forward flow
🫀 rapidly collapsing ventriculo arterial coupling
And unlike MI related shock: 📌 many of these patients still have relatively preserved LVEF.
Which means: normal or “acceptable” EF does NOT exclude severe shock physiology.
One of the most fascinating findings: 📌 the aortic valve was the most commonly involved valve.
Especially: • aortic stenosis • acute aortic regurgitation
And outcomes differed substantially by lesion type.
Patients with:
⚠️ stenotic lesions had the worst survival
⚠️ regurgitant lesions performed better
⚠️ mixed lesions remained intermediate
Severe AS in shock creates:
• fixed forward flow obstruction
• catecholamine inefficiency
• coronary hypoperfusion
• profound ventriculo arterial uncoupling
while acute regurgitant lesions may still preserve some forward stroke volume if rapidly corrected.
Another extremely important message:
📌 definitive intervention mattered enormously.
Compared to medical therapy alone:
• surgery had the best survival
• percutaneous therapies were intermediate
• medical management had the worst outcomes
After multivariable adjustment: medical management alone was associated with nearly 4 times higher hazard of death at 1 year.
But this study suggests: ⚡ definitive therapy may be the only real survival strategy.
The paper also highlights something increasingly relevant for modern CICUs:
📌 prosthetic valve dysfunction accounted for almost one third of VCS cases.
With aging populations and expanding TAVR/bioprosthetic use: this phenotype will likely increase dramatically over the next decade.
From a hemodynamic perspective, VCS may require:
🩺 earlier invasive monitoring
🩺 advanced echocardiography
🩺 rapid valve team activation
🩺 individualized MCS strategy
🩺 faster transfer to high volume structural centers
The study also indirectly supports something many intensivists already suspect:
📌 timing is probably everything.
Delayed recognition likely converts salvageable hemodynamic collapse into irreversible multiorgan failure.
This is where future research should probably focus:
• shock phenotyping by valve lesion
• optimal MCS selection
• VA coupling analysis
• transcatheter rescue timing
• CICU to structural heart pathways
• predictive models for intervention candidacy
📖 Nair RM, JACC Advances. 2024;3(11):101303.
https://t.co/eo9wstNwiZ
🫁One of the most underappreciated complications of mechanical ventilation may not be inside the lung.
It may be inside the kidney.
This excellent review revisits a question many intensivists intuitively suspect at the bedside:
📌 can PEEP itself contribute to acute kidney injury?
The article moves beyond the simplistic “high vs low PEEP” debate and reframes the problem through physiology.
Not every kidney injury associated with ventilation is simply “shock related.”
The review proposes that:
🫁 lung recruitability
🫀 right ventricular loading
🩸 venous congestion
🧠 neurohormonal activation
🫁 transpulmonary pressure transmission
🩺 abdominal venous stasis
may all interact dynamically during mechanical ventilation.
One particularly important concept:
PEEP may impair renal function not only through reduced cardiac output, but also through venous congestion.
That changes the way we think about ventilator associated AKI.
The review highlights two distinct physiological scenarios:
1️⃣ Highly recruitable lungs
Higher PEEP increases lung volume and pleural pressure, potentially compressing the vena cava and impairing venous return.
2️⃣ Poorly recruitable lungs
Higher PEEP produces overdistension, elevated pulmonary vascular resistance, RV stress, and systemic venous congestion.
Different lungs.
Different mechanisms.
Potentially similar renal consequences.
Another major strength of this paper is the integration of:
• VExUS physiology
• renal venous Doppler
• abdominal congestion
• cardiorenal interactions
• Guytonian hemodynamics
• pulmonary vascular physiology
The figures are particularly educational for ICU clinicians trying to understand how intrathoracic pressure may propagate into systemic venous circulation and renal perfusion.
Importantly, the review does not conclude that “high PEEP is bad.”
Instead, it argues something much more nuanced:
📌 inappropriate PEEP for the individual lung may be harmful.
That distinction matters enormously.
The future probably lies in truly personalized PEEP:
🫁 recruitability based
🫀 RV aware
🩺 congestion monitored
🧠 physiology driven
rather than protocolized fixed tables alone.
For intensivists, this review is also a reminder that: oxygenation improvement does not automatically mean systemic benefit.
Sometimes the kidney is paying the hidden price for a “better” PaO₂.
📖 Benites et al. Critical Care (2025) 29:130 https://t.co/6XP5hYp45T
A lot of haemodynamic confusion comes from one basic error: treating descriptions of the system as if they were causes.
Pressure gradients, preload, RAP, afterload, Starling... all are useful, but often misread.
This review tries to put them back together into a coherent framework.
https://t.co/L19bsDCzr6
🫀In cardiogenic shock, we still focus heavily on MACROcirculation:
📉 blood pressure
📉 cardiac output
📉 LVEF
📉 vasopressor dose
But what if the real battle is happening deeper?
🩸 At the microcirculatory level.
This excellent ATS viewpoint highlights one of the most important evolving concepts in shock physiology:
⚠️ normalization of macrocirculation does not necessarily mean restoration of tissue perfusion.
Despite advances in cardiogenic shock management, mortality remains >40%.
Even more striking, up to 45% of deaths occur in patients with normalized cardiac index.
That disconnect may be explained by persistent:
🩸 microvascular dysfunction
🩸 impaired capillary perfusion
🩸 endothelial dysfunction
🩸 tissue hypoxia despite “acceptable” hemodynamics
The review reinforces that: Microcirculation is not a passive bystander.
It may be a central driver of:
• organ dysfunction
• lactate persistence
• shock progression
• mortality
Particularly interesting is the emphasis on simple bedside tools.
We often think microcirculation requires advanced devices, yet:
📌 capillary refill time (CRT)
📌 mottling
📌 ΔPCO₂
📌 lactate trends
still carry strong prognostic value.
A CRT >3 seconds at ICU admission was associated with worse outcomes, and combining CRT with the CardShock score achieved an impressive AUC of 0.93 for outcome prediction.
The article also reviews modern technologies:
🔬 handheld vital microscopy
🔬 sublingual microcirculation imaging
🔬 NIRS
🔬 laser Doppler assessment
bringing “real time” bedside microcirculatory monitoring closer to clinical practice.
One of the strongest physiological messages:
⚠️ Shock is not only about flow. It is about effective tissue level oxygen delivery.
The review beautifully summarizes the four major mechanisms of microvascular dysfunction:
• heterogeneity
• hemodilution
• congestion
• edema
Particularly relevant for intensivists:
📌 venous congestion itself may worsen microvascular flow
📌 elevated filling pressures impair driving pressure
📌 edema increases oxygen diffusion distance
This is highly relevant in:
• advanced heart failure
• VA ECMO
• mixed shock states
• fluid overloaded patients
Another important takeaway: Persistent microcirculatory dysfunction after VA ECMO initiation was associated with increased mortality, even when macrocirculation improved.
Perhaps the key message of this paper is:
🩸 Microcirculation should no longer be considered a secondary endpoint in cardiogenic shock.
It may become one of the most important physiological targets of the next decade.
📖 Merdji H, American Journal of Respiratory and Critical Care Medicine. 2026, 212(3), 410–413 https://t.co/81Zp3aj274.
Latest post on https://t.co/5dIBLwYhWN -
“Not Every Dilated IVC or Pulsatile Portal Vein Is Pathological”
#POCUS#Nephpearls#echofirst
🔗 https://t.co/p6zEzOhuel
https://t.co/IPx62cLdKh
Please spread the word, thank you in advance,
Benedek, Huba, Levente, Emese and Mat
(The trip is self funded, all donations will go to Friends of Sandcross)
Fundraising for Friends of Sandcross Charity!
Our family of five will participate in a 30km kayaking regatta
We are raising funds for the boys’ school: @SandcrossSchool to improve their outdoor learning space.
Please consider supporting our goal!
Link in the next post:
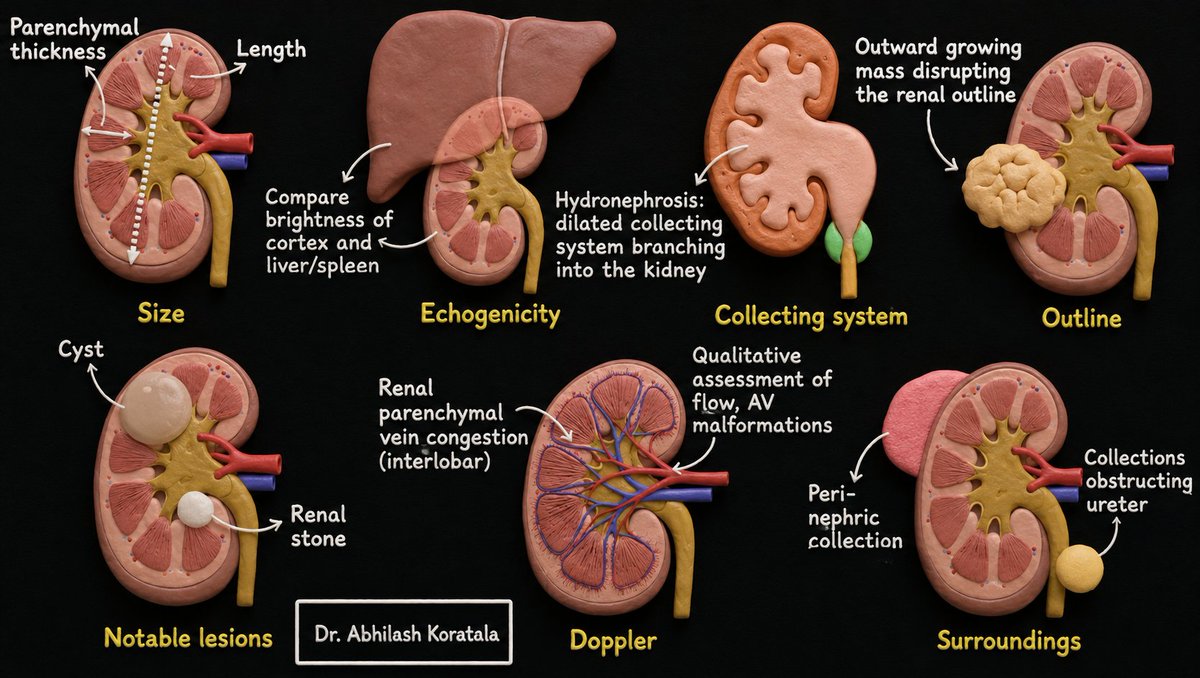
SECONDS checklist for systematically interpreting kidney #POCUS#Nephpearls#FOAMed
S – Size (renal length and cortical thickness)
E – cortical Echogenicity
C – Collecting system (hydronephrosis)
O – Outline (most masses grow outwards and disrupt the outline)
N – Notable lesions such as cysts and stones
D – Doppler (differentiate hydronephrosis and vascular structure, assess flow)
S – Surroundings (ascites, perinephric collections)