Tümör biyolojisini öğrenmemizle birlikte günlük pratiğimiz çok daha değişecek. Ancak bu tür kombinasyonların hangi hastalık grubunda en yararlı olduğunun ortaya konularak her hasta grubuna özel tedavi dizayn edilmesi yani precision onkoloji prensiplerine göre çalışmaların dizayn edilmesi gerekir. Belzutifanın ilk onayı VHL mutant grupta iken sonraki çalışmaları her hastaya verelim şekline dönüşmüştür. İlacın fiyatını da göz önüne alırsak ……….. ilaç firmalarının bu yaklaşımı sağlık sistemlerinin performans bazlı ödeme sistemine geçmesini teşvik edecektir. Yani işe yarayan tedavi ödenmeli gibi
“Same trial. Two regulators. Two completely different conclusions.”
Why did the US FDA Oncologic Drugs Advisory Committee (ODAC) hesitate… while the European Medicines Agency Committee for Medicinal Products for Human Use (CHMP) moved toward approval?
This isn’t just about camizestrant.
It’s about a much bigger question in oncology:
👉 Should we act when molecular resistance appears?
OR
👉 Wait until radiologic progression becomes visible?
🇺🇸 FDA/ODAC: “Is the evidence mature enough?”
🇪🇺 EMA/CHMP: “Why wait for scans to worsen?”
SERENA-6 may become a defining moment for ctDNA-guided precision oncology.
#BreastCancer #SERENA6 #Camizestrant #ctDNA #PrecisionOncology #ESR1 #Oncology #MedEd #MVOnco
Bu çalışmada önemli olan mekanizmaların ortaya konularak kombinasyonun etkili olmasıydı. Yem l nokta her kanser değişen biyolojik yapısına özel olarak tedavi edilmelidir. Bu mantığı ortaya koydu. Zaten Dr. Barbacid çalışmasında tek ajan daraxonasib yeterince erkili değildi. Kombinasyon başarıya ulaşmıştı.
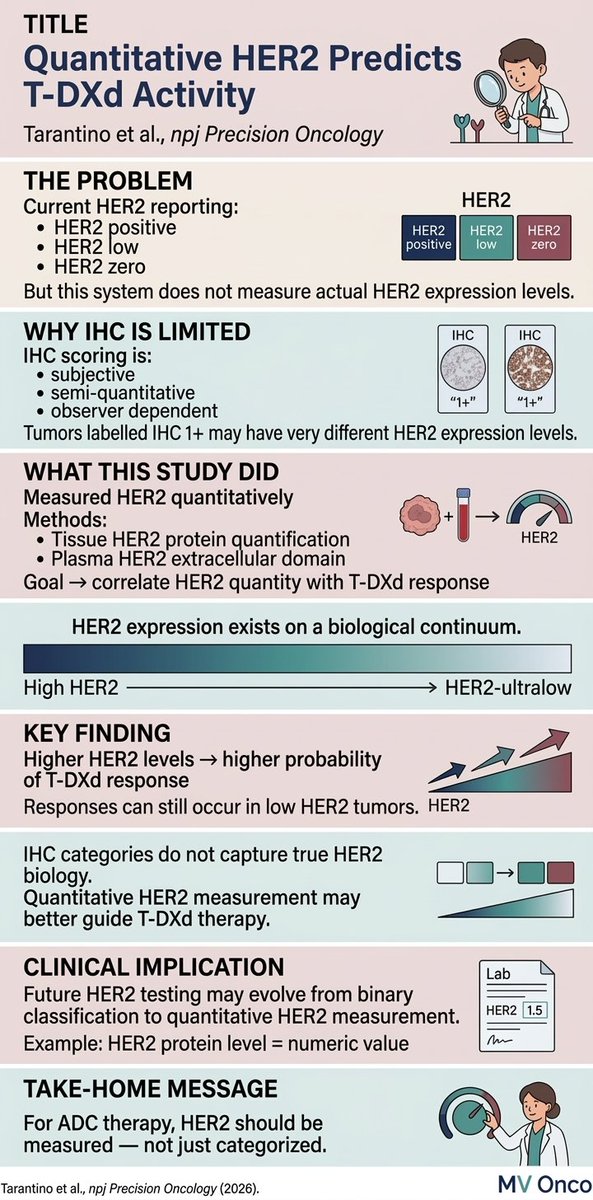
HER2 isn’t binary — it’s a continuum.
Quantitative HER2 levels correlate with activity of trastuzumab deruxtecan, highlighting the limitations of traditional IHC categories.
Perhaps the future of HER2 testing is measurement, not classification.
#MVOnco#BreastCancer#ADC
@footbalista_ Fenerbahçeli olmak çok zor. Oyuncular hatta iyi oyuncular bile kaldıramıyor artık. Bence sanatçı taraflarını takdir edelim orada kalsınlar. Fenerbahçe galatasaray ile ilgili konularda rasyonel kayboluyor halüsinasyonlar başlıyor
New data shows ultra-low-dose nivolumab (20mg) outperforms standard chemo in advanced cancers. It extended life, cut severe side effects by nearly 20%, and protected QoL.
Less can be more.
@ASCO@JCO_ASCO@OncoAlert
We’re excited to announce Tezer Kutluk (@mtkutluk) as a speaker at Global OncoThon 2026, organized by OncoDaily in collaboration with the Union for International Cancer Control (@uicc).
On this important day, Tezer Kutluk will join global experts, advocates, and changemakers to support a worldwide conversation and collective action against cancer.
February 4, 2026 – World Cancer Day
Live on OncoDaily TV
Join us and be part of this global movement amplifying voices and impact in cancer care.
https://t.co/9xV5Cd0zRP
#OncoDaily #Oncology #Cancer #Health #Medicine #OncoThon #GlobalOncoThon2026 #WorldCancerDay #UnitedByUnique
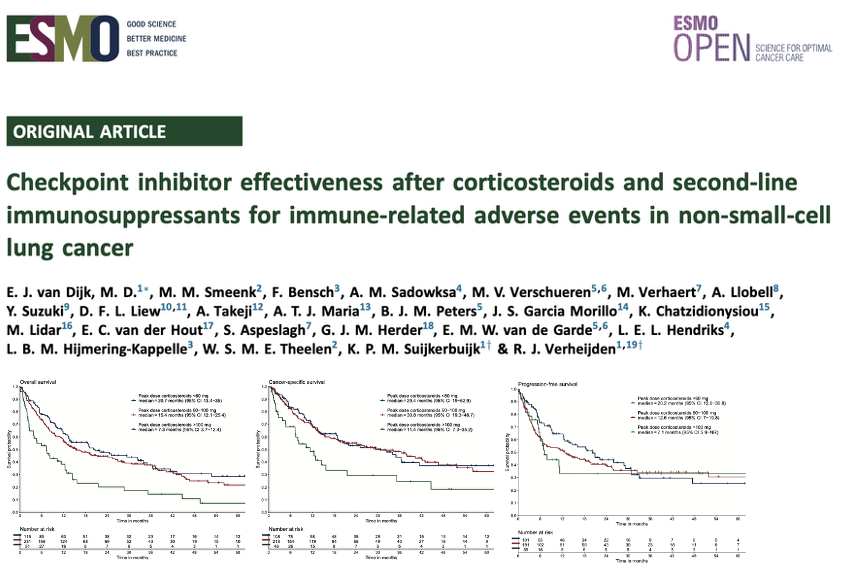
Checkpoint inhibitor effectiveness after corticosteroids and second-line immunosuppressants for irAEs in NSCLC in @ESMO_Open. High steroid peak dose associated with reduced survival, but not cumulative dose/2nd line immunesuppression. https://t.co/36GhbzCHlc
ASCENT trials in breast cancer = not 1 trial, it’s a whole PROGRAM 🧬🔥
Same drug (Trodelvy = sacituzumab govitecan), different disease settings. Here’s the clean map 👇
🧪 ASCENT (classic, Phase 3)
🌍 Later-line mTNBC (heavily pretreated)
⚔️ SG vs physician’s choice chemo
✅ Landmark trial that established SG as standard later-line option in mTNBC 📉🏆
🧪 ASCENT-03 (Phase 3)
🥇 1st-line advanced TNBC when IO not an option (PD-L1 negative or special scenario)
⚔️ SG vs physician’s choice chemo
✅ Improved PFS in frontline setting 🥇📈
🧪 ASCENT-04 / KEYNOTE-D19 (Phase 3)
🥇 1st-line PD-L1+ metastatic TNBC
⚔️ SG + pembrolizumab vs chemo + pembrolizumab
✅ PFS benefit with the ADC + IO combo 💉🤝🛡️
🧪 ASCENT-05 / OptimICE-RD (Phase 3)
🎗️ Early-stage TNBC with residual disease after neoadjuvant therapy + surgery
⚔️ SG + pembrolizumab vs physician’s choice adjuvant therapy
🎯 Goal = cut recurrence risk in “highest-risk” early TNBC 🔥🧬
✨ Takeaway:
ASCENT = Trodelvy across the TNBC timeline
Late-line ➝ first-line ➝ IO-combo ➝ post-neoadjuvant residual disease
🔖 Save this for boards + clinic + tumor board memory.
📖 Full paper in comment ⬇️
#OncoTwitter #MedTwitter #BreastCancer #TNBC @OncoAlert@myesmo@esmo_open@asco@stolaney1@PTarantinoMD