Sepsis + AKI + bradycardia + home beta blocker or CCB = BRASH syndrome.
Anand Swaminathan, MD (@emswami) from ResusX:ReUnion:
This isn't an OD — their kidneys just stopped clearing the drug. Standard pressors won't work. What's your next move at the bedside? Comment below.👇
SOHO trial in NEJM:
🏙️ Multicenter RCT comparing high-flow nasal cannula vs. low-flow oxygen among patients with acute hypoxemic respiratory failure (mostly pneumonia)
🏙️ Inclusion criteria required a respiratory rate >25 and substantial hypoxemia (P/F <200)
🏙️ No difference in the primary endpoint of mortality (not surprising, the mortality endpoint is nearly always neutral in modern RCTs evaluating the nuances of supportive care).
🏙️ HFNC reduced the rate of intubation and increased the number of ventilator-free days.
🏙️ No significant signals of harm from HFNC.
This is similar to the FLORALI trial (by the same group of investigators). However, FLORALI showed *improvement* in mortality, whereas the current study didn't.
Why do these studies disagree about mortality?
The FLORALI trial found no mortality difference between HFNC versus conventional oxygen among ALL PATIENTS. However, it DID find a mortality difference in the *subgroup* of patients with P/F <200.
So this is a classic tale in critical care - a subgroup analysis from one trial subsequently fails to replicate. (At least, in terms of the mortality benefit.)
But chasing mortality in these trials is a fool's errand. Overall, the SOHO trial still supports the use of HFNC in acute hypoxemic respiratory failure (in terms of reduced intubation and improved ventilator-free days).
Using HFNC for sick pneumonia patients is already standard care, so I don't see this changing practice very much. Keep calm and HFNC on. 🌬️
Valproic acid is great for refractory agitated delirium.
🏆 Especially useful in patients with explosive/aggressive behavior in the context of a personality disorder (often exacerbated by delirium).
Candidates for VPA:
✅ Not pregnant
✅ No severe liver dz or history of hyperammonemia
✅ No major drug-drug interactions with VPA
✅ Didn't respond to antipsychotics +/- alpha-2 agonists (dexmedetomidine). This isn't a hard requirement, but generally VPA isn't usually a front-line agent.
Advantages of VPA:
👍 Cardiovascular stability
👍 Low risk of airway compromise (only mildly sedating)
👍 Antiseizure activity (e.g., can be used for sz prophylaxis in an agitated patient)
👍 Can be given IV or PO (1:1 conversion with immediate-release formulations)
👍 EM/ICU folks should be knowledgable and comfortable within it already
Disadvantages of VPA:
👎 Dosing requires a little more thought than most agents. For patients on this for more than a few days you want to check a VPA trough and adjust it using the Fraser equation (to account for albumin).
👎 Can cause a lot of side-effects (but most of these are due to *chronic* VPA, rather than just a few days of therapy)
Dosing
🎯 My preference is to use the same dosing regimen as for status epilepticus (40 mg/kg load max 3 grams, then 15 mg/kg/day in divided doses). You can up-titrate as needed while following VPA troughs if ineffective (max dose of 45 mg/kg/day).
🎯 Many studies have reported starting lower and up-titrating, but this delays its efficacy for 2-3 days.
🎯 Using more frequent doses (e.g., q6hr rather than q8hr) may avoid toxic peak levels while maintaining adequate trough levels.
This isn't an option I use a ton, but it's a terrific tool to have in your toolbox for agitated delirium that isn't responding to usual front-line treatments.
⚠️ VPA should be weaned off prior to hospital discharge (unless the patient is seen by psychiatry and they are intentionally recommending VPA as chronic outpatient therapy for bipolar disorder etc - which would be uncommon).
(more discussion on VPA pharmacology in the IBCC chapter on status epilepticus)
Recent article on this in NeuroCritical care here:
Proposal: for complex patients (eg ICU) we should *always* get CBC w/ differential (not plain CBC)
- Same amount of blood
- Run by the same machine (it usually CHECKS the differential & just dumps the data!)
- Trivial cost difference
- Can be helpful (eg Eos 2/2 drug, NLR)
What do tactile fremitus and OR fires have in common? Why we keep doing things that don't make sense: radial art lines, NPO after midnight, Trendelenberg position, etc?
Checkout my new blog post about Ritual and Reason in Medicine.
https://t.co/JJ3dUDzozK
every single RCT involving a care bundle:
"we did a buncha stuff, something worked, we're not sure what worked or why it worked, good luck implementing this weird bunch of stuff, byeeeee"
writing pet peeve: insanely broad ranges on percentages
don't write "5-50%" - this phraseology lacks any clear meaning
either find a reasonably accurate number, or don't use numbers at all (e.g. "commonly" would work just fine)
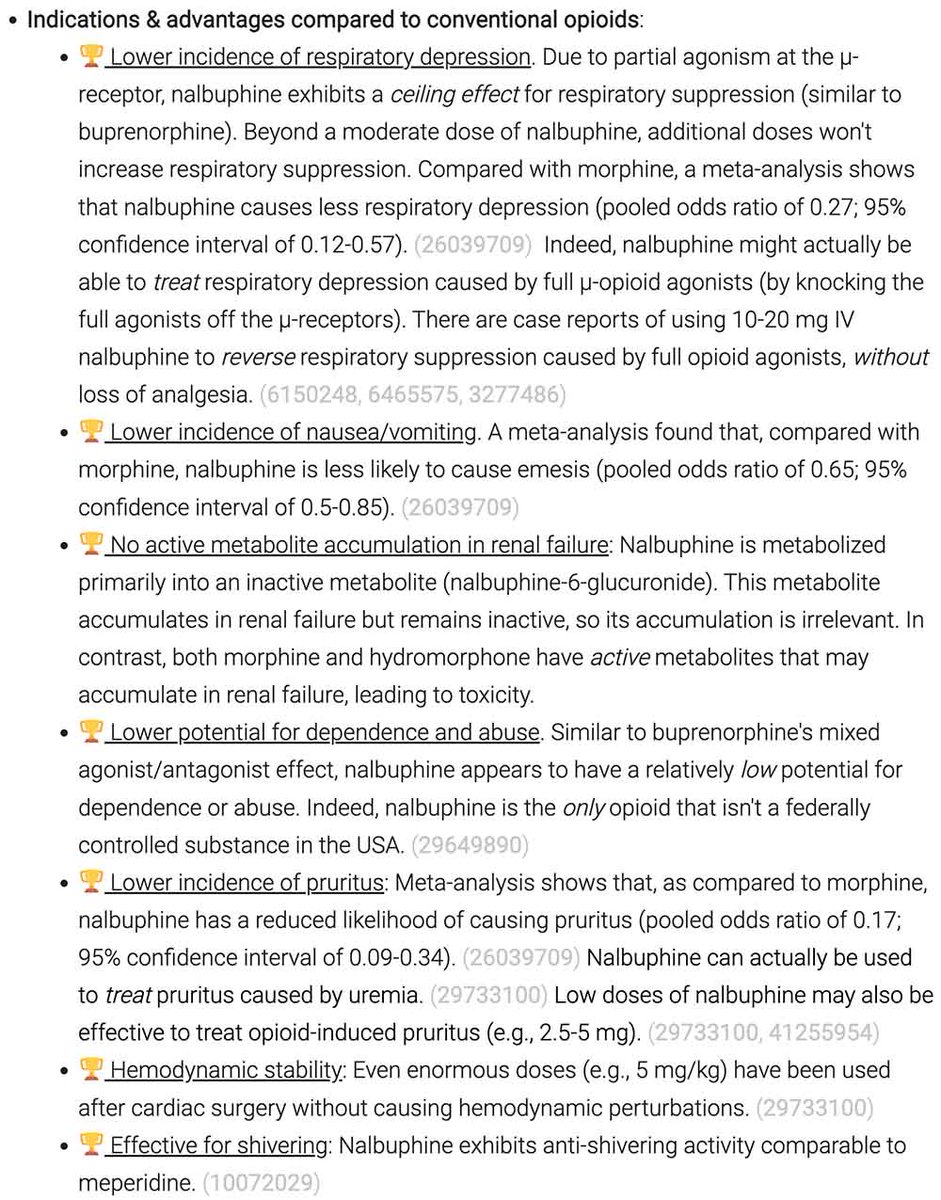
note to self: use more IV nalbuphine
it's supported by robust theoretical & clinical evidence
I'm pretty sure the only reason we don't use it more often is due to our training and habits (not EBM)
especially useful in patients with tenuous respiratory drive
EMCrit Wee - An Airway Discussion with Jonathan St George of the Protected Airway Collaborative
Informal chat on the DAS guidelines and a bunch of other airway stuff.
https://t.co/IPwjrU8fk0
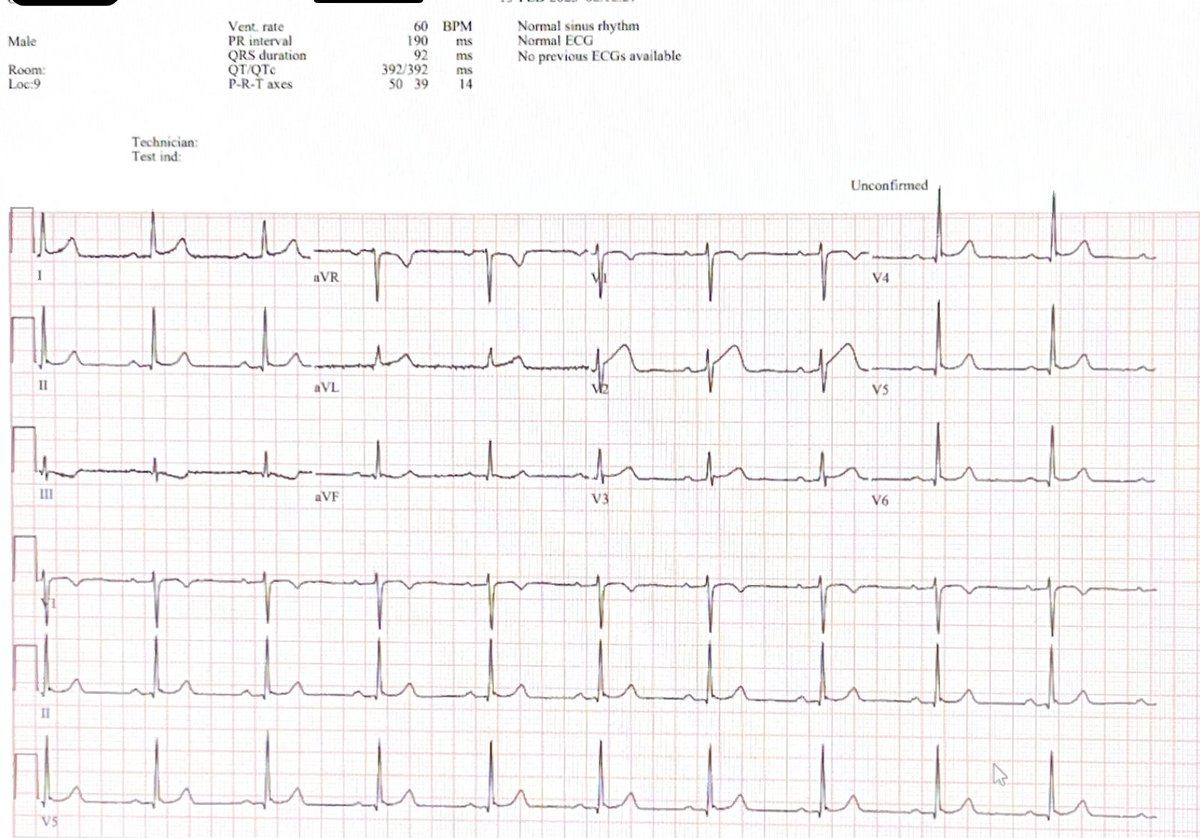
33yo M w/2 hrs of CP; computer and AI called it normal. But good old-fashioned HI (human intelligence) called it positive. Kudos to Dr. Mohammad Assiri, dx'd South African Flag sign, 100% D1 blockage, life saved! #foamed
recent encounter:
patient family: “Your team reminds us of the Pitt… We know you’re doing everything you can and we trust you.”
the Pitt explains how medicine works to the public (eg interns and students are an integral component of care)
congrats to Wyle N et al 🐐
medicine is great at creating unnecessary problems to subsequently solve.
medicine: we gonna force you to renew your zoloft script every month for the rest of your life
also medicine: WOW we can get a robot to sign the refill requests, THIS IS AMAZING
antiseizure meds has a PK/PD profile similar to beta-lactam antibiotics:
-efficacy relates to the trough
-toxicity relates to the peak
so benefit/risk ratio is maximized with smaller, frequent dosing
hard to do outside the hospital re: adherence
but easy for inpatients
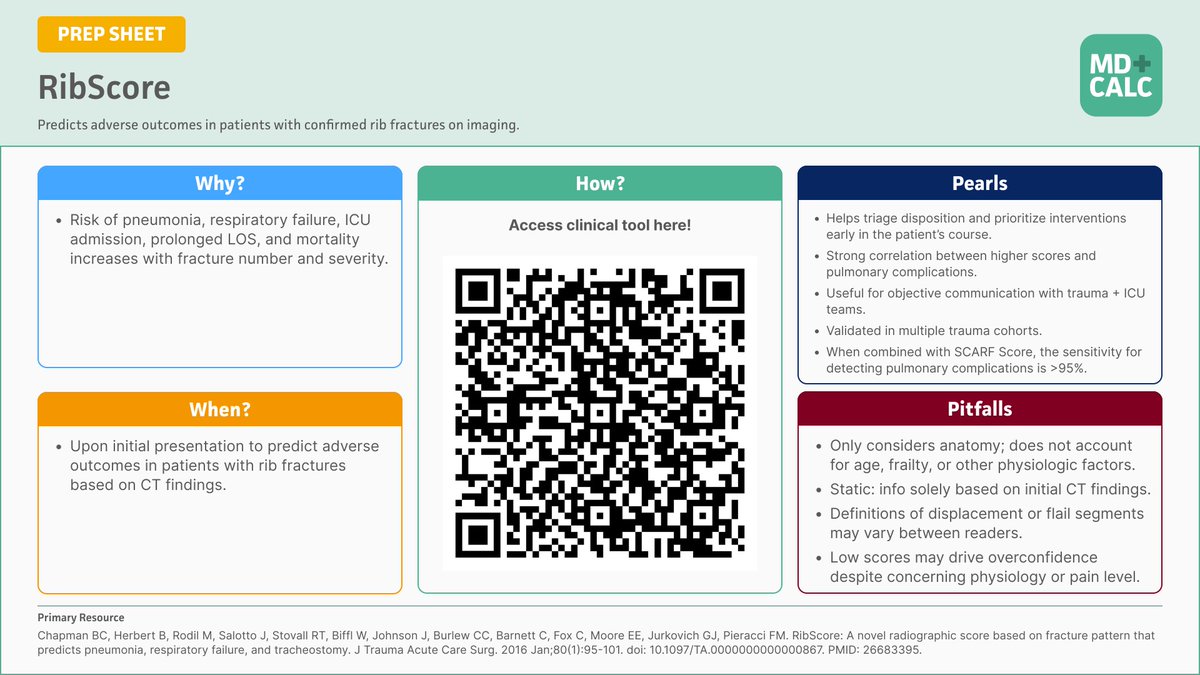
🫁 New on REBEL EM
Rib fractures ≠ benign. Using RibScore + SCARF improves prediction of respiratory decline—>95% sensitivity when combined.
📖 https://t.co/5YZqsBKQtr
By Dr Eric Steinberg | Reviewed by @Marco_Propersi & @MRamzyDO#FOAMed#MedEd#Trauma#RibFracture
serious question:
has there ever been a high-quality RCT that demonstrated clinically meaningful benefits from pulse-dose steroid (e.g., 500-1000 mg/day methylprednisolone) as compared to a moderate dose of steroid (e.g., 1-2 mg/kg/day prednisone)?
for *any* disease?