Semua Piala Dunia memiliki cerita mimpi, di Piala Dunua 2026 tampaknya itu adalah milik Tanjung Verde .. Pertama kali lolos, poin perdana, goal perdana dan akhirnya lolos dari penyisihan grup. Silahkan cubit, karena ini bukan mimpi. #fifaworldcup2026
Terakhir ketemu tim Eropa di Piala Dunia, yaitu melawan Spanyol, skor 5-1.... Di WC 2026, bertemu tim Eropa lain skor sama.... Hup Hup Holland #OnsOranje#WC2026#fifaworldcup 2026
In necessariis unitas, in non-necessariis libertas, in utrisque caritas ;
In essentials, unity ; in non-essentials, liberty, in all things, charity (love)
(9/9). This thread has just a few of the cardiac arrest advances on the horizon (or that are ready for prime time). I know I've missed a ton - I would love to hear from all my X colleagues ...
what's new for cardiac arrest in 2025?!
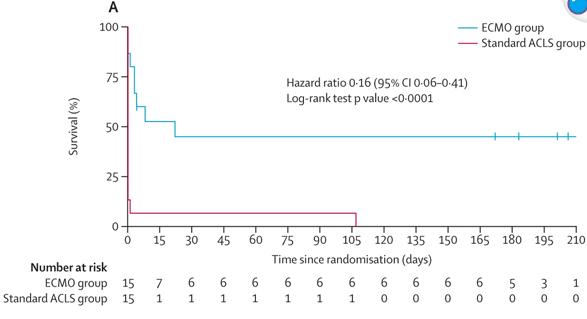
(8/x) #7: ECPR with VA-ECMO
There is increasing evidence that for select patients with refractory cardiac arrest ECPR using VA-ECMO improves evidence.
The catch, unless you are one of the incredibly high performing center that does this routinely, the logistics (and probably outcomes) are not as good as top centers that do this routinely.
Think of it for:
1. Young patients with cardiac arrest from a reversible cause (think PE or MI)
2. Activate early (often takes a while to go on pump)
3. Need a 'system of care' --> getting them on ECMO is just the beginning. What next?
Have personally seen some amazing saves of patients who have had refractory cardiac arrest, one for more than 80 minutes of CPR with totally neurologically in tact survival.
(6/x) #5: Esmolol for refractory VF
The strength of evidence for this isn't strong (recent SRMA suggestive of potential benefit however very weak quality of evidence - https://t.co/4VugiIUNdA) , however, in refractory VF patients esmolol can be considered as part of the cocktail.
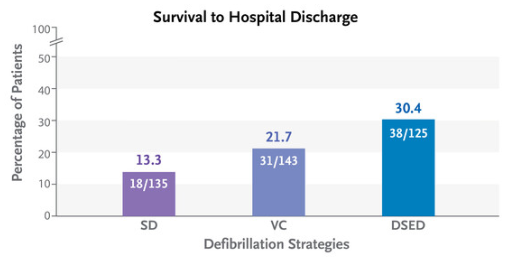
(5/x) #4: Vector change defibrillation
Normal pad placement for defibrillation is typically anterior-lateral.
Turns out that simply changing the pads to be anterior -posterior (think cardioversion) will improve survival to hospital discharge! (DOSE-VF RCT!)
Dual sequential defibrillation (two defibs) also improved survival but logistically is so much harder to coordinate in many centers.
I try to go anterior-posterior whenever I have the chance!
Study below is DOSE-VF RCT in @NEJM
(4/x) #3: TEE to improve CPR quality and identify reversible causes
This is my favorite enhancement to cardiac arrest care that I think is ready for prime-time in the right centers.
TEE can:
1. Reposition CPR (in 50% of cases is done in wrong location over LVOT/aorta)
2. Identify cause of arrest
3. Identify fine Vfib or other arrythmia
4. Guide procedures (ECMO, pacemakers etc.)
@FTeranMD and @ResusTEEproject are changing the landscape of this with a huge international registry of patients.
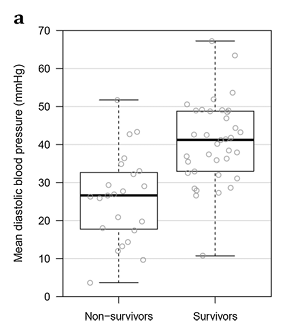
(3/x) #2: Arterial Line monitoring of CPR quality
This is a bit of a double edge sword.
Having arterial pressure monitoring for CPR is fantastic for:
1. Monitoring for ROSC --> reduce pulse check duration
2. Monitoring CPR quality --> diastolic BP (DBP) less than 30mmHg may be less correlated with ROSC
3. Theoretically can be used to titrate vasoactive medications
4. Distinguish between PEA and pseudoPEA
Out of these, number 1 and 4 are the most useful for me. Manually checking for pulses in cardiac arrest is notoriously inaccurate (even among skilled providers).
The problem? Placing arterial lines in cardiac arrest is hard (even for experienced clinicians!). Here are some tips:
1. Best operator available
2. Make sure you are going for common femoral (people sometimes go too low in cardiac arrest)
3. Have someone stabilize the pelvis manually (this reduces motion of the legs) ****
4. Ultrasound guided is a must (you will likely be venous blind because the vein is huge and artery is small in cardiac arrest)
Biggest error is becoming task focused on the access. Placing an arterial line is great when there are lots of skilled hands around, but when I'm a solo code team leader don't have the bandwidth to do myself.
PMID: 27107688 (animals although human data for this too)
(2/X) #1: ETCO2 monitoring intra-arrest
For some clinicians ETCO2 use in cardiac arrest is routine - for many others -- it is not available (or being used). It is easy to use and very useful.
Read more: https://t.co/82NSG7KBuu
The theory behind using ETCO2 in cardiac arrest is that to produce CO2 and exhale it (End tidal CO2), you need to have perfusion to the lungs. Thus, assuming the patient isn't being horribly overventilated, the ETCO2 seen in cardiac arrest is a reflection of the amount of perfusion making it to the lungs (surrogate of CPR quality).
If the value is <10mmHg, this is either a bad prognosis or CPR isn't effective
10-20mmHg - common during cardiac arrest and not super reassuring
20+ high quality CPR and when even higher, potential ROSC.
Intra-arrest - if I see a CO2 of 25mmHg with one provider then 10mmHg with the next, I look at rate, depth, recoil, and position of CPR (see tip 3 - LVOT or aorta compression?)
Post arrest, I find it very useful too. When a patient is post arrest and their ETCO2 is 50, if I start seeing it drop to 40....30...25 I know the patient is likely about to re-arrest and can intervene, even when the blood pressure is "OK". The pressure might be maintained because of high SVR from the epinephrine etc.
There is a lot more nuance to ETCO2 in cardiac arrest, however, so check out the post linked above as ETCO2 can tell you even more about CPR quality.
(1/x) High quality CPR, early defibrillation, and treating the underlying cause saves lives in cardiac arrest, but what else can we do?
Here are 7 advanced therapies for cardiac arrest👇
A🧵
Caution: Bleeding edge - evidence 'light' zone.