“Critical Conversations: Emergency Medicine Unfiltered” is a virtual podcast where we break down complex, often controversial, topics in emergency and critical care. Each episode features experts delving into real-world challenges and cutting-edge practices. In our upcoming episode, we’ll focus on environmental emergencies, particularly heat-related crises.
If you’re an expert with field experience or research in this area, we’d love to have your perspective on the show!
Let’s connect: [email protected]
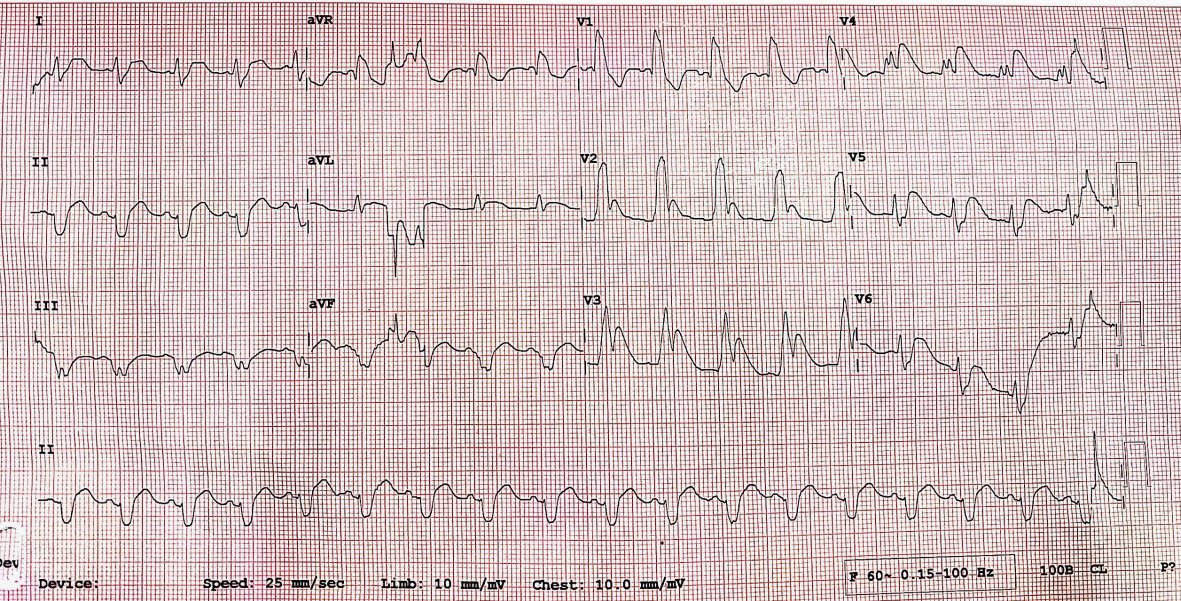
Sodium Channel–Mediated Ventricular Arrhythmia After Delphinium denudatum Ingestion Managed Conservatively in a Resource-Limited Setting | JACC: Case Reports https://t.co/MIinEj9bDj
Published in JACC! A rare toxin leading to PMVT, managed with Lidocaine.
It was a difficult airway in terms of anatomy as well as physiology. The patient was a middle-aged female with an anterior neck mass, short neck, morbidly obese, and obtunded. BP was 88/40mmHg with tachycardia of 120bpm. The anatomical aspect is very important here as the laryngeal complex was pushed to the left by the huge thyroid which made the laryngoscopy difficult.
A lady in her 60s, presented to ED with SOB for a few days and drowsiness for 1 day. No history of fever.
ABGs showed TIIRF with a CO2 of 91mmHg. I intubated her using C-MAC and Eschmann tracheal tube introducer in the ED.
P.S. - When she arrived in the Resus Room, I did the PoCUS Neck which showed an enlarged thyroid with increased vascularity.
@EM_RESUS@srrezaie@AirwayMxAcademy@JohnCSakles @dastrainees @cliffreid@precordialthump
@cliffreid Wow! The important part of this intubation was the position of the laryngeal complex as it was pushed towards the left due to huge thyroid. On the 1st laryngoscopy by a PGY5, she couldn't locate the epiglottis as she was going straight like in a normal patient.
@smithECGBlog@willyhfrick If this is an EKG of a young adult with exertional symptoms, then it's most likely HCM. It fulfills the voltage criteria for LVH + Qs in lateral leads.