Mexican Neurologist , Parkinson et al ... “To hell with circumstances; I create opportunities". Neuróloga adscrita a @NeurologiaHU . Opinions my own. 🧠
Spirituality and neurological diseases like Parkinson’s and Alzheimer's. Could faith, meaning and purpose shape how folks cope and heal? Spirituality refers to how individuals search for meaning, purpose and connection, whether through religion, nature, relationships or personal beliefs. Indu Subramanian and colleagues describe in a new paper in Neurology Clinical Practice how spirituality can play a powerful role in neurologic disease care, including Parkinson’s disease, and how health care providers can better address it as part of whole person care.
Key points:
– Spirituality helps folks w/ neurologic disease cope w/ uncertainty, disability and identity changes by providing meaning, hope and emotional resilience.
– Many patients want their health care providers to ask about spirituality, however these discussions frequently do not happen because of lack of training, time and comfort.
– Simple screening questions and integrating spiritual practices such as prayer, meditation or community engagement may improve quality of life and strengthen the therapeutic relationship.
My take: This paper reminds us that Parkinson’s disease is not just about dopamine or brain circuits. It is about identity, purpose and meaning. When health care providers acknowledge spirituality, they help folks feel seen as whole human beings. In my experience, these conversations frequently deepen trust and improve care. We do not need to have all the answers. Sometimes simply listening and being present is the most powerful intervention.
Here are 5 points that resonated w/ me:
1- Spirituality can help folks make sense of many neurological disease (Parkinson’s, Alzheimer's and beyond) and can help folks cope w/ uncertainty and loss.
2- Many folks want their health care providers to ask about what gives them strength and meaning.
3- Addressing spirituality can improve quality of life, emotional well being and satisfaction w/ care.
4- Health care providers do not need to be spiritual experts, simple questions and active listening can help.
5- Whole person care including physical, emotional and spiritual health may be essential to living well w/ Parkinson’s.
https://t.co/66kxOTAq1K @ParkinsonDotOrg@GreenJournal@FixelInstitute
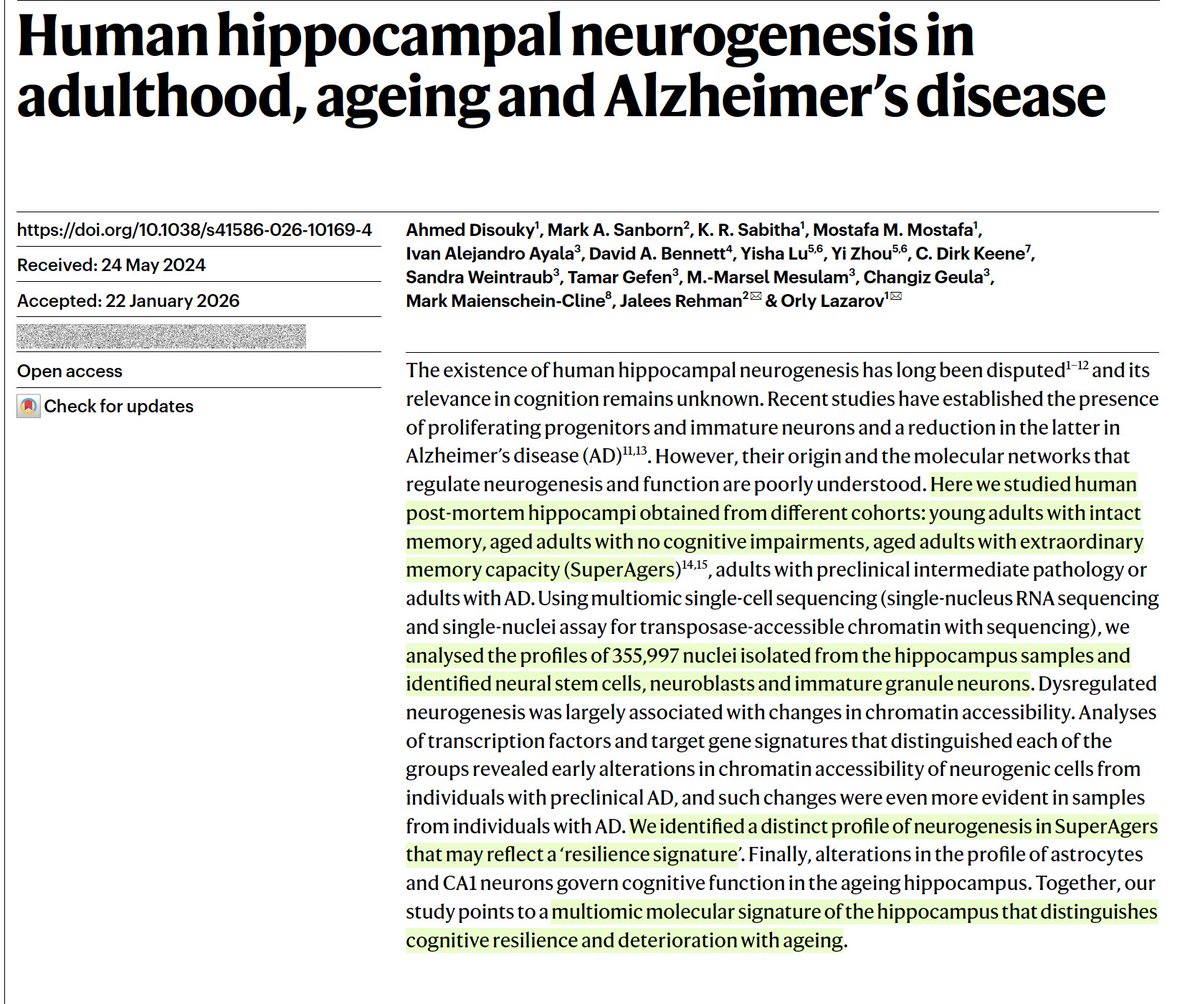
New @Nature
The brains of Super Agers produce more neurons than people some 40 years younger, a neurogenesis resilient signature linked to exceptional cognitive health and memory skills
https://t.co/tNB0dTea2F
👨⚕️👩⚕️🧠Esta tarde llevamos a cabo la reunión de la Asamblea General del @ConMexNeuro.
🥼Se evaluaron los procesos que llevamos a cabo, así como las estrategias que se implementarán para garantizar la excelencia neurológica en nuestro país.
En este marco llevamos a cabo nuestra reunión y desahogamos diversos puntos para dar cumplimiento al plan de trabajo establecido por la Mesa Directiva.
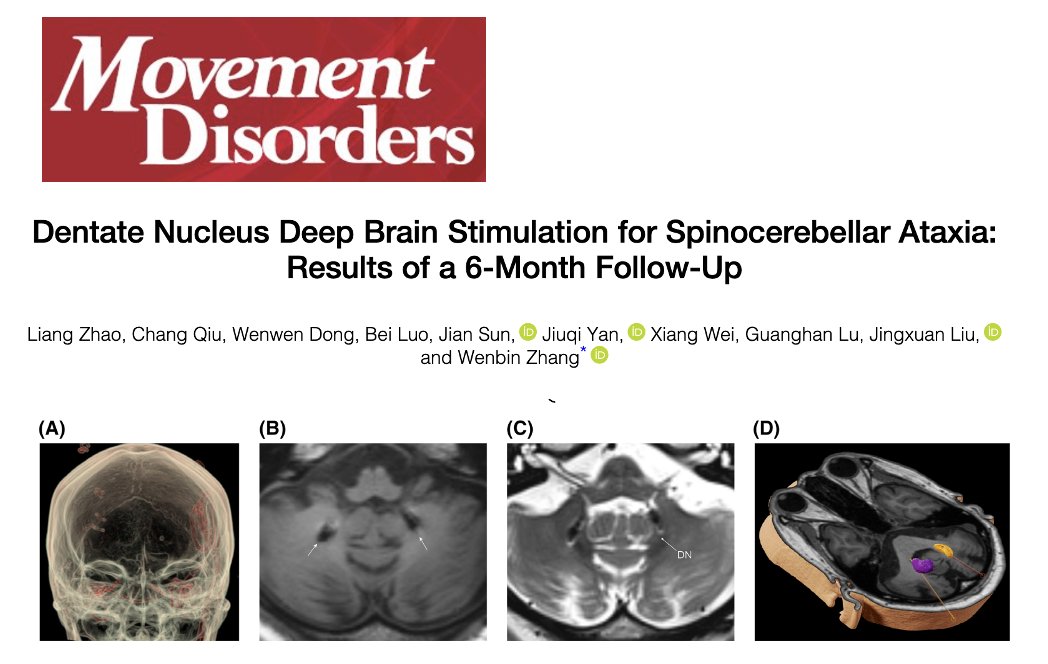
Could dentate nucleus DBS be applied to treat spinocerebellar ataxia (SCA)? Dentate nucleus is one of the key cerebellar output stations that helps shape coordinated movement by sending refined motor signals upstream in the brain. Zhao and colleagues describe in a new paper in Movement Disorders that dentate nucleus deep brain stimulation delivered meaningful improvement to folks living w/ spinocerebellar ataxia at 6 months of follow up.
Key Points:
- Bilateral dentate nucleus DBS in six folks w/ various genetic subtypes of spinocerebellar ataxia (SCA 1, 3, 21) led to significant improvements in gait and coordination by 6 months.
- SARA and ICARS scores improved by 43 percent and 51 percent.
- Iterative programming identified sweet spots where lower frequencies seemed to stabilize gait and higher frequencies suppressed tremor.
- Higher frequencies could induce worsening of gait.
My take: We are now beginning to unlock our understanding of cerebellar function. We are entering an excited era where neuromodulation for cerebellar dysfunction is becoming more and more possible. Here are 5 points that resonated w/ me about this article:
1- Spinocerebellar ataxia frequently affects gait balance speech and coordination and this diagnosis makes everyday tasks challenging for many folks. 2- The cerebellum is the brain’s movement calibrator and the dentate nucleus acts like its main output station, sending refined signals to improve movement. 3- Deep brain stimulation of 'dentate' cerebellar relay revealed early promise in improving walking stability, hand control and posture, however this was a very small group of folks. 4- Benefits emerged gradually as stimulation settings were fine tuned. The authors highlighted the importance of careful programming w/ experienced health care providers. 5- This therapy is still experimental and remember that benefits could be diminished over time w/ disease progression.
https://t.co/1AUasZSveQ #parkinson @NAF_Ataxia@AtaxiaUK@Ataxia_and_Me@ParkinsonDotOrg@movedisorder@SfNtweets@DBSThinkTank
La Mesa Directiva del @ConMexNeuro felicita y da la bienvenida a nuestros tres nuevos concejales:
- Dr. Juan Fernando Góngora Rivera
- Dra. Araceli Reyes Cuayahuitl
- Dr. Guillermo Vargas López
Su labor y profesionalismo contribuirá en fortalecer nuestras funciones. Enhorabuena
🚨📢Presentaremos Convocatorias para los exámenes de Certificación y Recertificación 2026 para las especialidades en:
- Neurología Adultos
- Neurología Pediátrica
- Medicina del sueño
- Terapia Endovascular Neurológica
✅🥼🧠💻 Consúltalas aquí: https://t.co/hsVOCQJ1Zp
Our article on Miryachit published today. A culturally determined startle syndrome with links to shamanism in the Saami nation. Like jumpers and latah it is getting less common with globalisation
https://t.co/Npd8SmPmrS
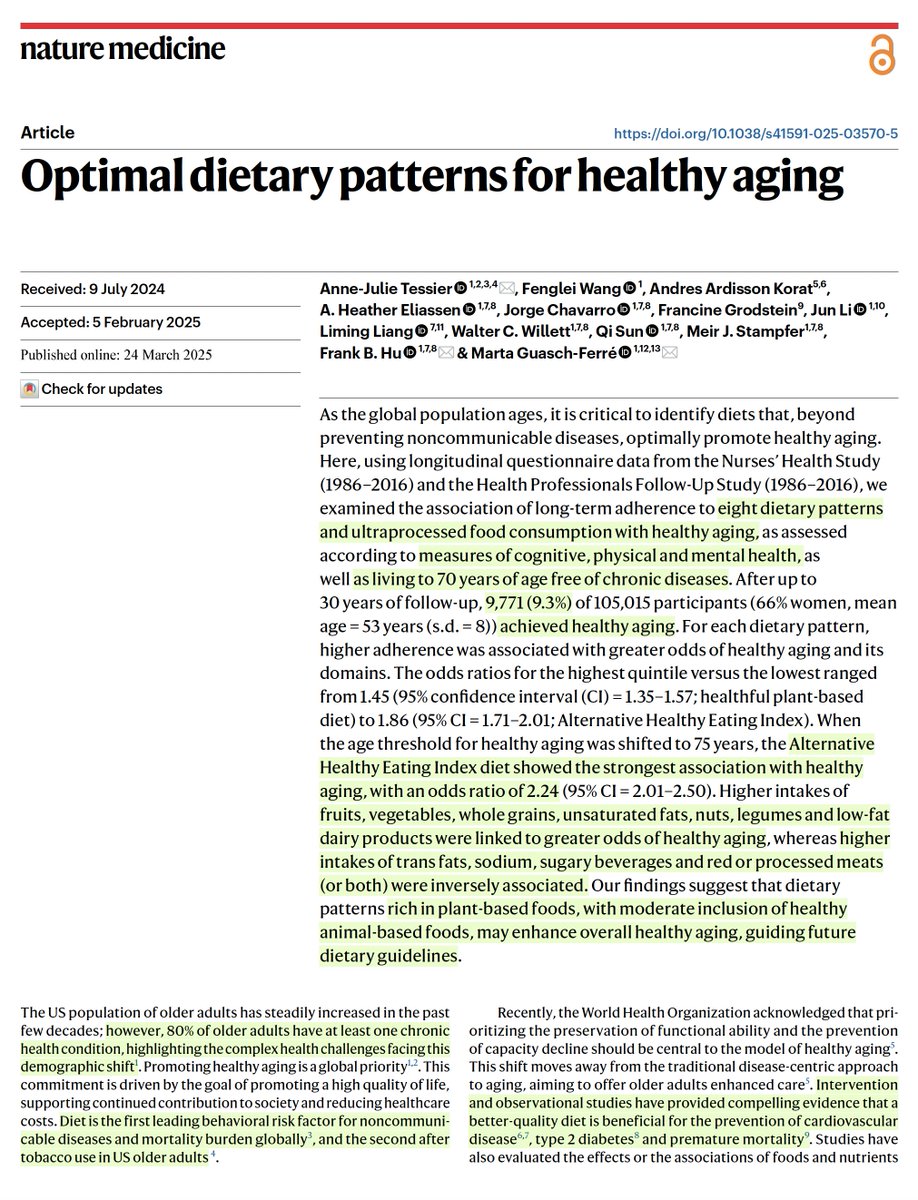
Of >105,000 participants with 30-year follow-up, only 9.3% achieved healthy aging (age 70, w/o any chronic diseases). Their diet was significantly associated with this outcome🧵 @NatureMedicine
Case of Pure Agraphia in Kana and Romaji Without Sensorimotor Deficits After a Small Infarct of the Posterior Limb of the Internal Capsule
https://t.co/OKfPmWIrRF
#NeuroX
Up to 60% of patients with schizophrenia have prominent or predominant negative symptoms that are clinically relevant and need treatment (Correll & Schooler, 2020).
Despite their impact, they are often misdiagnosed and resistant to standard treatments.
Here’s what you need to know about their neurobiology, functional impact, and treatment strategies. 🧵👇
Where is the evidence on treatments for Parkinson's disease motor fluctuations? How do we choose? Remember – ense et aratro – sometimes we choose the sword, but in Parkinson's, over time the plow is usually the better strategy. de Bie and colleagues do an evidence-based review in the journal Movement Disorders.
Key Points:
-What is a motor fluctuation?
- Here is a greatest hits list (7): 1- alternating periods of good movement control referred to as on, and poor movement control referred to as off. 2- wearing-off, 3- sudden shifts between on and off, 4- delayed onset of doses working, 5- dose failure, 6- freezing, and 7-dyskinesia.
- The International Parkinson and Movement Disorder Society (MDS) Evidence Based Medicine in Movement Disorders Committee updated recommendations based on all available research studies.
- 102 studies met criteria.
- Efficacious: levodopa extended release, pramipexole immediate release and extended release, ropinirole immediate release, rotigotine, opicapone, safinamide, and bilateral subthalamic nucleus deep brain stimulation (DBS).
- Likely efficacious: continuous intestinal levodopa infusion, continuous subcutaneous levodopa, continuous subcutaneous apomorphine, ropinirole prolonged release, ropinirole patch, entacapone, rasagiline, istradefylline, amantadine extended release, zonisamide, bilateral globus pallidus DBS, and pallidotomy.
My take: Parkinson's, in my opinion, is the most complex disease in clinical medicine. Though it is nice to see these evidence-based reviews, we should keep our eye on the 'ball.' The ball is dynamic, and in Parkinson's will fluctuate over time, and especially with disease progression. We need to listen carefully to the persons with disease. We need to pay attention to the timing of dosages and realize that more is not always better. We need to choose the 'cocktail of the day' for medications, and realize the mixture will change over time. We need to know when to pull the trigger for DBS, focused ultrasound or pumps, and also to not forget that exercise and multi-disciplinary therapies, as well as diet and sleep, can also help. Zonisamide is not used much in Western countries, and perhaps we should consider this choice more often? Remember, despite where the level of evidence is at the moment, we are pretty sure that GPi DBS is currently the best overall therapy for dyskinesia, and especially for brittle dyskinesia. Remember – ense et aratro – sometimes we choose the sword, but in Parkinson's over time the plow is the better strategy.
https://t.co/RKItYrzLPP #Parkinsons @ParkinsonDotOrg@FixelInstitute@MDJ_Journal
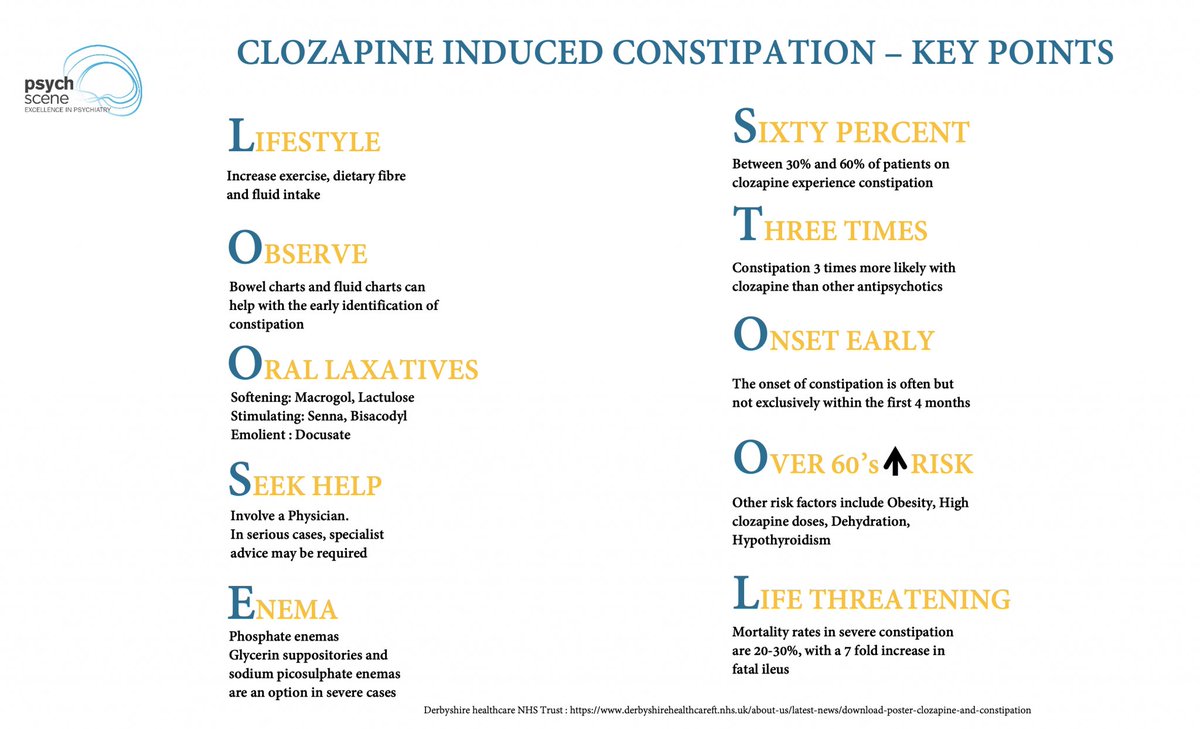
Clozapine-induced constipation (CIC) is more fatal than agranulocytosis but remains under-recognised.
Studies suggest up to 60% of patients may develop it, and severe cases have an estimated 30% mortality rate.
Here’s what psychiatrists need to know about its pathophysiology, prevention, management, and recognising clinical deterioration. 🧵👇