🔔 ¿Seguimos esperando a que la creatinina sérica suba para diagnosticar una Lesión Renal Aguda?
Llegamos tarde.
La línea de tiempo conceptual presentada en el #ERA26 demuestra que la creatinina y la caída del volumen urinario son marcadores de disfunci��n clínica tardía, no de daño temprano.
El estrés renal inicia mucho antes con la parada del ciclo celular, detectable inmediatamente tras el insulto mediante biomarcadores ultrasensibles como TIMP-2 e IGFBP7.
Cambiar nuestra mentalidad del diagnóstico funcional al molecular es imperativo para la nefroprotección crítica.
#Nefrología #MedicinaCrítica #ERA26 #AKI #NefroTwitter
#lesionrenalaguda #dañorenal #IRA #AKI
#ERA26
🚨Results of the study:
🍀HDx was non-inferior to OL-HDF for a composite cardiovascular outcome and showed similar safety and mortality profiles.
🍀HDx presents as an alternative to OL-HDF in settings where optimal convective dosing cannot be consistently achieved
One of the most awaited talks for this #ERA26
MOTheR HDx Study: A MOPR Study to Explore Morbidity and Mortality in Patients Dialyzed with Theranova HDx Compared with OL-HDF
🗣️ @DePsequera
Late breaking clinical trials 2:
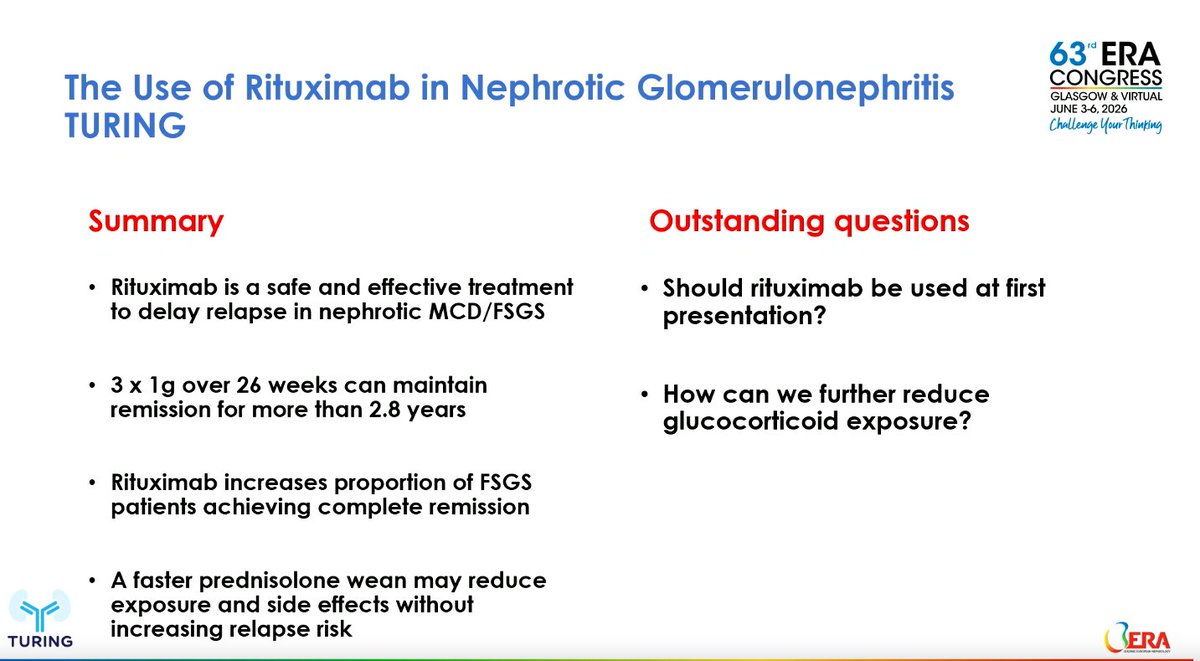
The Use of Rituximab In the treatment of Nephrotic Glomerulonephritis (TURING): a multicentre, double-blind, randomised, placebo-controlled trial
By Lisa Willcocks (Cambridge, UK) &
Megan Griffith @megan_griffith1 (London, UK)
#ERA26
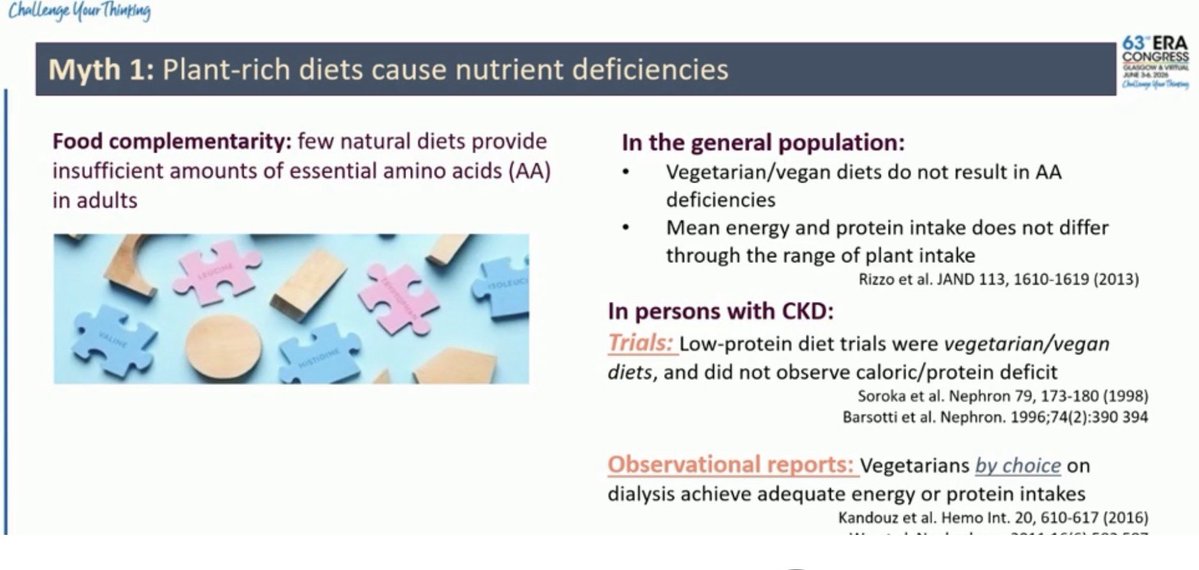
Starting strong with controversies in nephroprotection #ERA26@jjcarrero1 talking about potassium 🍌🥑
📍Plant-rich diets do not inherently cause protein deficiency in CKD.
Plant phosphorus is less absorbable, so plant-based diets may ⬇️ phosphate burden despite similar phosphorus intake
📍The evidence supporting routine restriction of fruits and vegetables to prevent hyperkalemia is weaker than traditionally believed
📍Focus on food quality and individual risk, not automatic avoidance of plant foods.
3/ Role of parietal epithelial cells
⏩ Parietal epithelial cells act as podocyte progenitors
⏩ Females generate more podocytes throughout life.
⏩ Estrogens drive podocyte regeneration
⚠️The proximal tubular phosphate transporter Npt2a may be more than a phosphate carrier‼️
💡In experimental AKI, Npt2a inhibition ➡️
📌restored mitochondrial fusion,
📌improved mitochondrial function and
📌attenuated kidney injury,
This highlights a novel Npt2a–Klf15–mitochondrial axis.
#ERA26 #AKI #KidneyResearch
🧵—Open your mind: New therapeutic opportunities in inherited kidney diseases
#ERA26@ERAKidney
1/🧵Overcoming Barriers in Rare Disease Drug Development
🗣️Speaker: Olivier Devuyst
1/ 💊 #ERA26
-Only a few rare genetic diseases have affordable treatment.
-Lysosomes are fundamental for cell cycling and promising targets for certain diseases.
Orgullosos de la participación activa de nuestra Unidad de Trasplante en el Congreso SET 2026.
📍Adjuntos y residentes compartiendo experiencia, aprendizaje e investigación en uno de los principales encuentros nacionales sobre trasplante💙����
#SET2026 #Trasplante #Nefrología
#POCUS#echofirst answer: 1️⃣ Subxiphoid short axis view at the aortic valve level 2️⃣ RVOT Doppler
RVOT Doppler is one of the most underused but high yield tools.
● Tracks RV stroke volume and cardiac output
SV = CSA × VTI
CO = SV × HR
VTI alone works well for serial trends
● Estimates pulmonary vascular resistance
PVR = (TRV ÷ RVOT VTI) × 10 + 0.16
● Screens for pulmonary hypertension even when TR jet is absent
AccT <105 ms suggests PH
AccT ≤60 to 80 ms raises concern for acute PE
● Waveform shape gives physiology
Parabolic is normal
Early peaking and notching suggest rising PVR and help phenotype disease
● Distinguishes acute PE from chronic PH using AccT and notching patterns
● Provides insight into RV pulmonary arterial coupling
RVOT VTI ÷ PASP as a simple coupling metric
● Useful in congenital heart disease
Grading RVOT obstruction and serial follow up after repair
● Tracks response to therapy noninvasively over time
CWD complements PW when velocities are high
● Grades pulmonic stenosis using peak velocity and gradients
Severe if peak gradient >64 mmHg or velocity >4 m/s
● Estimates pulmonary pressures from PR jet
mPAP = 4(V peak PR)² + RAP
PAEDP = 4(V end diastolic PR)² + RAP
● Identifies multi level RVOT obstruction
Double contour envelope suggests infundibular plus valvular disease
● Detects dynamic RVOT obstruction
Late peaking dagger shaped signal
● Enables global RV performance assessment
Tei index combining TR and RVOT flow
● Monitors conduit or bioprosthetic valve gradients over time
🤓 AKI in the ICU is not just kidney failure.
It is a hemodynamic and congestion failure.
🚨 Reality check
👉 AKI occurs in:
▪️ 13-36% of acute HF patients
▪️ Up to 80% in cardiogenic shock
👉 Dialysis needed in up to 13%
👉 Strongly linked to mortality
⚠️ The key mistake
We treat AKI as a creatinine problem
💥 But it is actually:
👉 A perfusion + congestion problem
🧬 Core physiology
Renal perfusion pressure = MAP - CVP - IAP - airway pressure
📌 The nephron needs ≈ 40 mmHg to function
🔥 So what kills the kidney?
Not just low pressure
But:
▪️ Venous congestion (↑CVP)
▪️ Fluid overload
▪️ Intra-abdominal hypertension
▪️ Low forward flow
🧩 Step-by-step mindset
1️⃣ Confirm congestion
👉 JVP, no fluid responsiveness, VExUS ≥1
2️⃣ Optimize hemodynamics
👉 Maintain MAP ≥65 mmHg
3️⃣ Decongest
👉 Diuretics = cornerstone
4️⃣ Escalate
👉 CRRT if failure
📌 It’s a flow-pressure-congestion algorithm
💊 Pharmacology reality
❌ “Renal-dose dopamine” → useless AND harmful
❌ No drug prevents AKI
✔️ Loop diuretics → first-line
✔️ Sequential nephron blockade if resistance
⚡ Diuretic resistance = turning point
👉 Think:
▪️ Gut edema → poor absorption
▪️ Hypoperfusion
▪️ Tubular dysfunction
👉 Solutions:
▪️ Higher doses
▪️ Combination therapy (thiazides, acetazolamide)
▪️ Consider hypertonic saline strategy
🚨 CRRT is NOT first-line
👉 Indications = AEIOU:
▪️ Acidosis
▪️ Electrolytes
▪️ Intoxication
▪️ Overload
▪️ Uremia
👉 Early CRRT?
❌ No mortality benefit
✔️ Wait-and-see + optimize first
🧠 Advanced insight
👉 The kidney fails more from:
✔️ Congestion than hypotension
✔️ Venous pressure than arterial pressure
🔥 Take-home
AKI management in ICU is:
✔️ Hemodynamic
✔️ Congestion-driven
✔️ Stepwise
🚨 Final message
👉 Don’t chase creatinine
👉 Don’t reflexively dialyze
Treat:
Perfusion + Decongestion + Time
📚 Riccardi et al.
European Heart Journal Acute Cardiovascular Care, 2025
https://t.co/OLnrbCQ8Y2
LESIÓN RENAL AGUDA EN CIRROSIS ‼️
📌LRA en cirrosis ( Criterios KDIGO) :
a) aumento de la creatinina sérica ≥0,3 mg/dl en 48 h o ≥50% del valor basal que se sabe o se presume que ocurrió en los 7 días anteriores y/o producción de orina ≤0,5 ml/kg durante ≥6 h
🔴 ¡Empezamos con el Módulo 1️⃣!
➡️ Fundamentos de la Hemodiálisis▪️Principios biofísicos▪️Composición del líquido de diálisis ▪️Acceso vascular @EmiliSanAlv@mf_slon@DePsequera@Florijaviesther👇
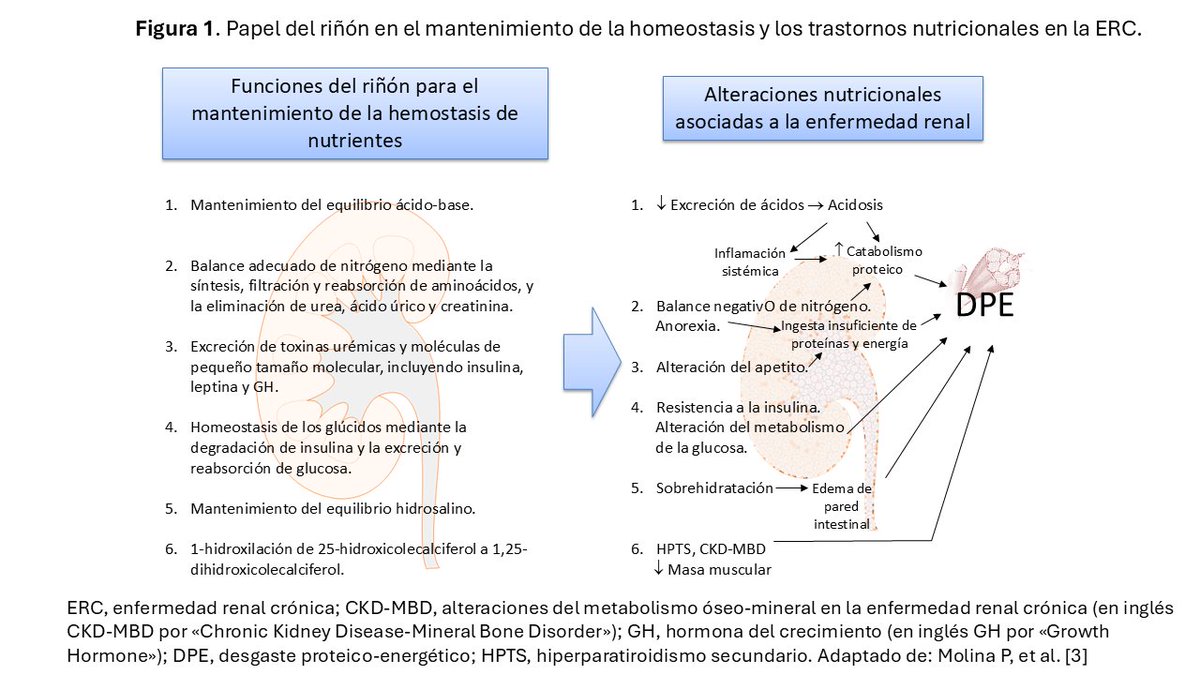
🔄 ACTUALIZADO en #Nefroaldía@nefroaldia
🥗 "Nutrición en Nefrología. Conceptos generales y estimación de los requerimientos nutricionales"
✍️ Por Pablo Molina @MolinaPab, Emma Huarte @emma_huarte y Macarena Arancibia
🔗 https://t.co/0HHR556aoT