“We did the hardest thing in the history of American health care. We got the majority of American doctors to all voluntarily adopt a single technology platform.”
NBC News on how that happened, what U.S. physicians actually do with OpenEvidence, and how partnerships with NEJM, JAMA, NCCN, and Wiley make it possible.
We're proud to announce our partnership with @EvidenceOpen.
OpenEvidence is the most widely used AI-based clinical decision support tool across the United States. Under this partnership, the Academy will share its Preferred Practice Patterns® and other clinical guidelines with OpenEvidence for incorporation into its training libraries and report on output for quality and consistency.
We encourage our members to share their experiences with the OpenEvidence tool, including observations about performance and recommendations for improvements, using a feedback form that is available from the Academy’s OpenEvidence page.
Read: https://t.co/7t0htiy1bE
#Ophthalmology #EyeCare #MedicalAI #EvidenceBasedMedicine #AAO #OpenEvidence
Ophthalmology is a field where the right answer lives three layers down. Not “treat glaucoma,” but which target pressure, for which optic nerve, given which visual field trend, in a patient who can’t tolerate first-line drops.
Starting today, the American Academy of Ophthalmology’s Preferred Practice Patterns are integrated into OpenEvidence. Decades of subspecialty judgment from the world’s largest eye physician and surgeon association, now cited and searchable alongside peer-reviewed literature.
When an ophthalmologist asks a question at the point of care, the @aao_ophth authoritative guidance is right there in the answer, every claim cited back to the source.
AI is not replacing doctors.
It is helping us catch what might otherwise be missed and make better decisions, faster.
Tools like this are already saving and improving lives.
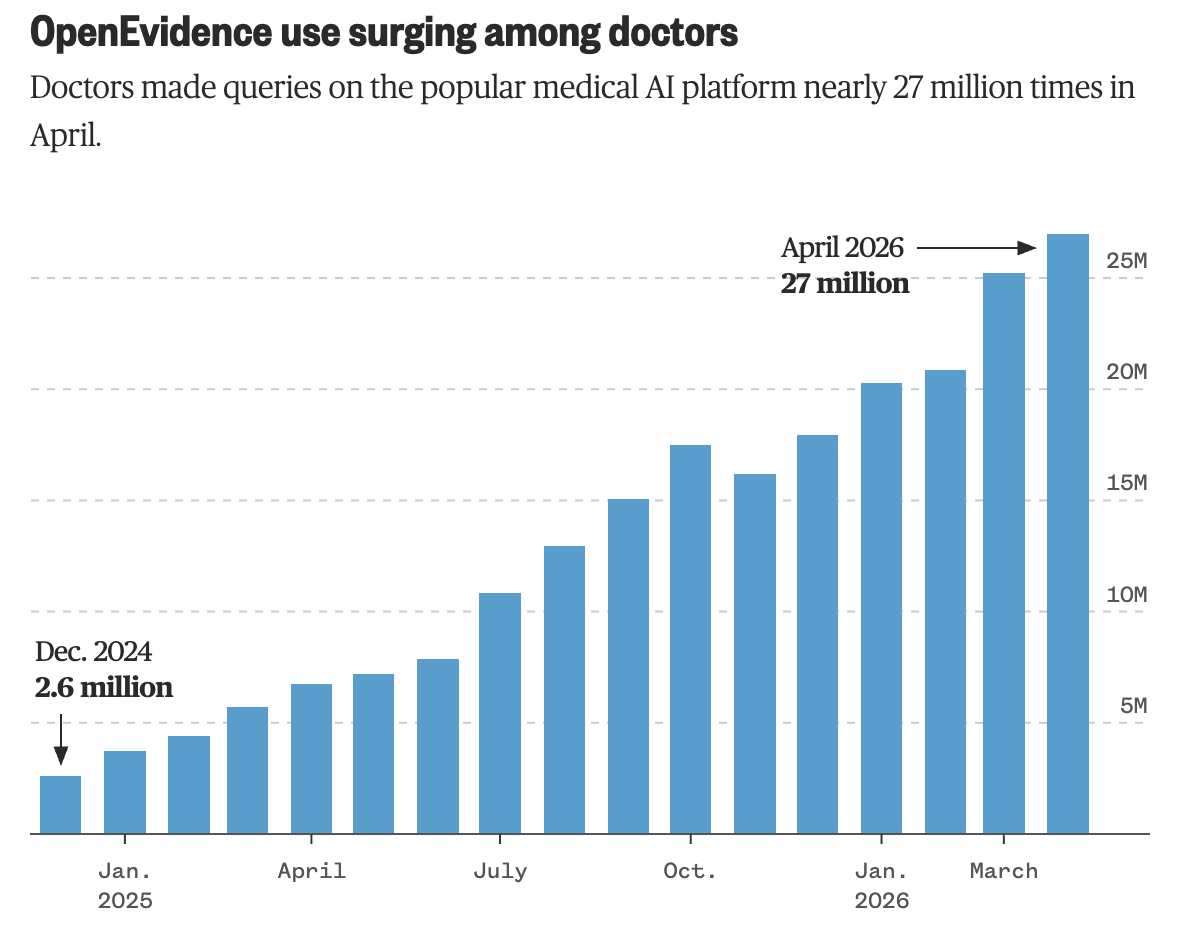
Last summer an ER doctor at Mount Sinai watched two med students and a resident pull up OpenEvidence mid-shift on a hard case. He assumed they were unusual. Then the health system found that a third of its 9,000 physicians were already using it.
That's how OpenEvidence spread. Doctors found it, tried it on real cases, and told the doctors next to them. The hospitals are now formalizing what their clinicians already do.
@SteveLohr piece in today’s New York Times follows that thread out to a small hospital in Alaska, where Dr. Barbara Creighton uses it on complex cases she’d otherwise send to a paid specialist consult. She calls it “like having a bunch of specialists in your pocket.”
The hype around medical AI usually skips the part doctors care about most, which is what the tool is for. Daniel Nadler summed it up in one line: “It’s not an oracle, it’s a tool. Knowledge and knowledge workers still matter.”
"It’s not an oracle, it’s a tool. . . . Knowledge and knowledge workers still matter."- Daniel Nadler, chief executive of OpenEvidence
https://t.co/sQP2c5mXrP
Thanks for the careful reporting, Steve. A doctor in Fairbanks getting specialist-level answers she’d otherwise pay to consult out shows why physicians are adopting OpenEvidence on their own. Most of medicine happens outside the big academic centers, and that’s where the gap is widest.
👇 Drs. @AmiBhattMD & @ankeetbhatt explore the impact of large language models (LLM) on CV care, share a practical framework for navigating LLMs, highlight important components to engineer an effective clinical prompt, & more. https://t.co/KcZ5qmX45u
#ACCInnovation@EvidenceOpen
The second Cleveland Clinic AI Summit is on August 28, something to look forward to when summer ends.
Hosted by @jamecancerdoc, with speakers from Stanford, Google Health, Mayo, Harvard, and major health systems. Dr. Travis Zack, OpenEvidence CMO, will be speaking.
We are hosting the second @ClevelandClinic Artificial Intelligence Healthcare Conference for all Healthcare team members - from Medical Students to Executives - August 28th @ClevelandClinic. Please see the all star speakers list from @Google to @Stanford https://t.co/6uBQmlvecN
@NEJM_AI “The answer might actually change.”
@NEJM_AI conversation with OpenEvidence CMO, Dr. Travis Zack, on why clinical AI needs time-aware evidence retrieval, not just fluent answers.
“The answer is not the important part.” In the latest episode of the NEJM AI Grand Rounds podcast, Dr. Travis Zack of @EvidenceOpen challenges how we measure both clinicians and AI. Hear more from Dr. Zack in the full episode: https://t.co/JzRDRlIqx6
@katy_beckermann Sharp real-world test case. The germline/somatic testing question is where physicians pause to verify the criteria. Glad it's useful in clinic.
Point-of-care AI that cites the guideline, and quick access to the literature. Useful in a busy clinic.
🏥 ASCO guidelines + flowcharts now embedded in @EvidenceOpen
📋 Peer-reviewed evidence + direct ASCO source link alongside each response
Practice prompt: "Which patients with prostate cancer should have germline and somatic genomic testing per ASCO guidelines?"
💡Delivers NCCN and ASCO guideline recommendations with ease of use for your quick clinical question
@ASCO #ASCO26 #AIinMedicine
ASCO 2026 wraps today. RAS(ON) in pancreatic. PD-1 bispecifics in lung. Cell therapy moving to community. Four days of practice-changing data, presented by oncologists who will see patients again tomorrow.
Translation was the theme of the meeting: from the podium in Chicago to the patient in the exam room. The harder half of that work happens after Chicago. That’s the half OpenEvidence is built for.
Dr. @SamyuktaMD on what we’re doing in oncology. #ASCO26