We like to find what we believe. My #cathlab highlights from #CAD 2024 European GL:
#radialfirst Class 1A: the end of ‘femoralists”!
#FFR Class 1A in intermediate lesions: the end of 1 angio=1 stent!
#IVUS/#OCT Class 1A for complex #PCI : the end of ‘I don’t need imaging’ guys!
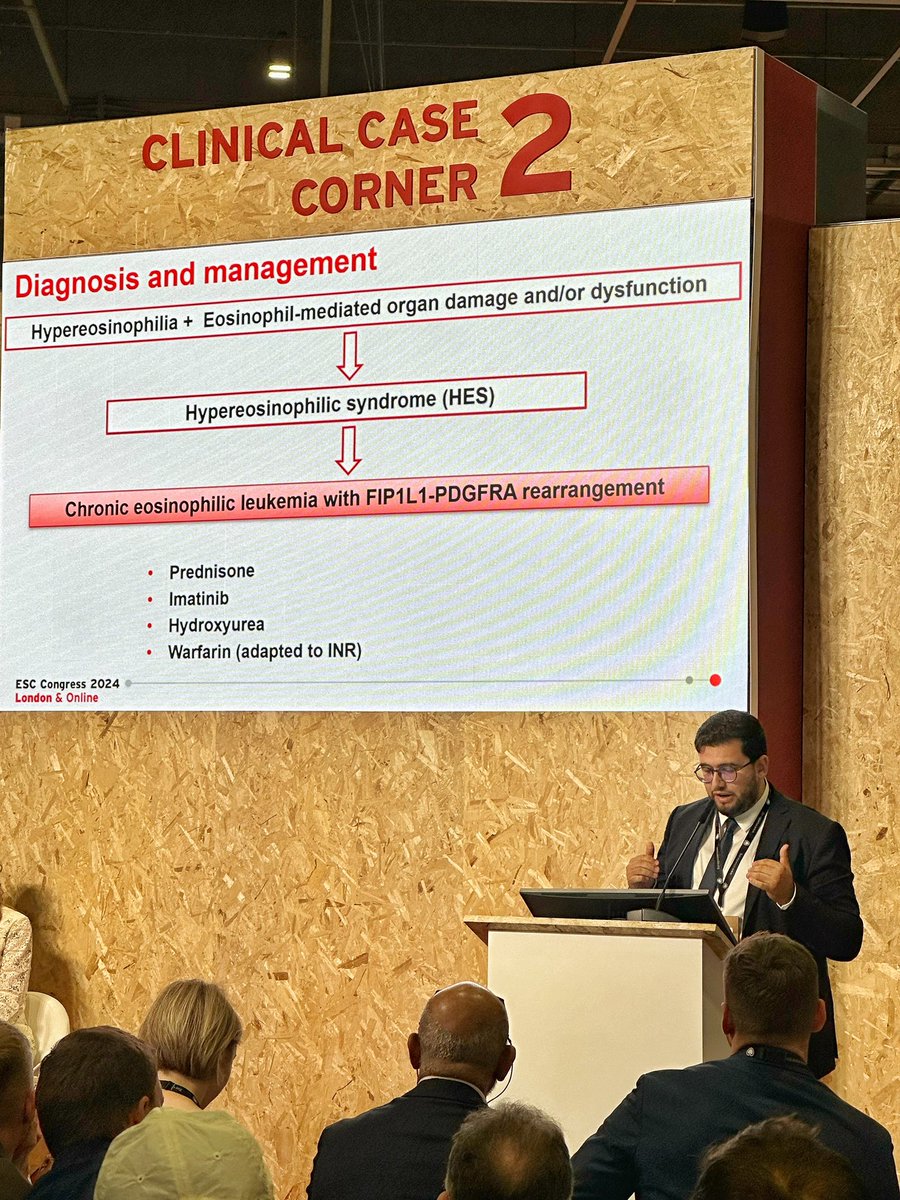
Grateful for the chance to present my research at ESC Congress 2024 in London. I learned so much from the incredible sessions and discussions with fellow experts. @escardio#ESCCongress2024#ESCCongress
@DrRajeshG1 This is a common scenario in our practice. To facilitate wire passage, having the patient take a deep breath and pulling down the arm can be very effective. Otherwise, we consider changing the access route.
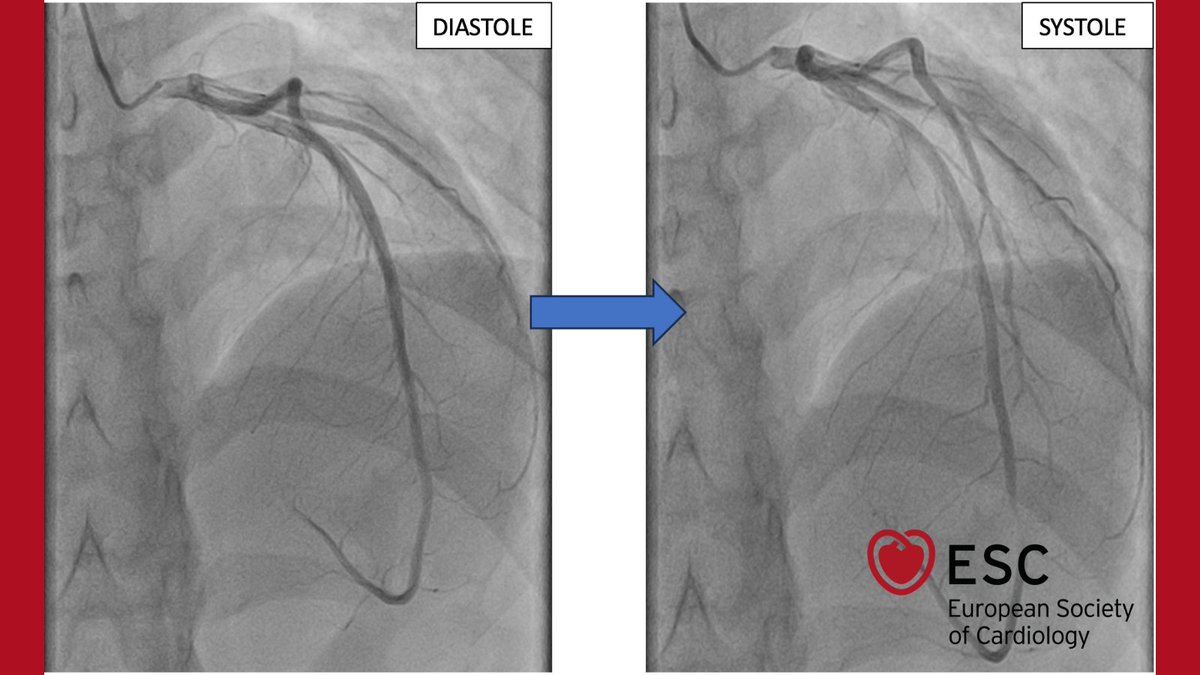
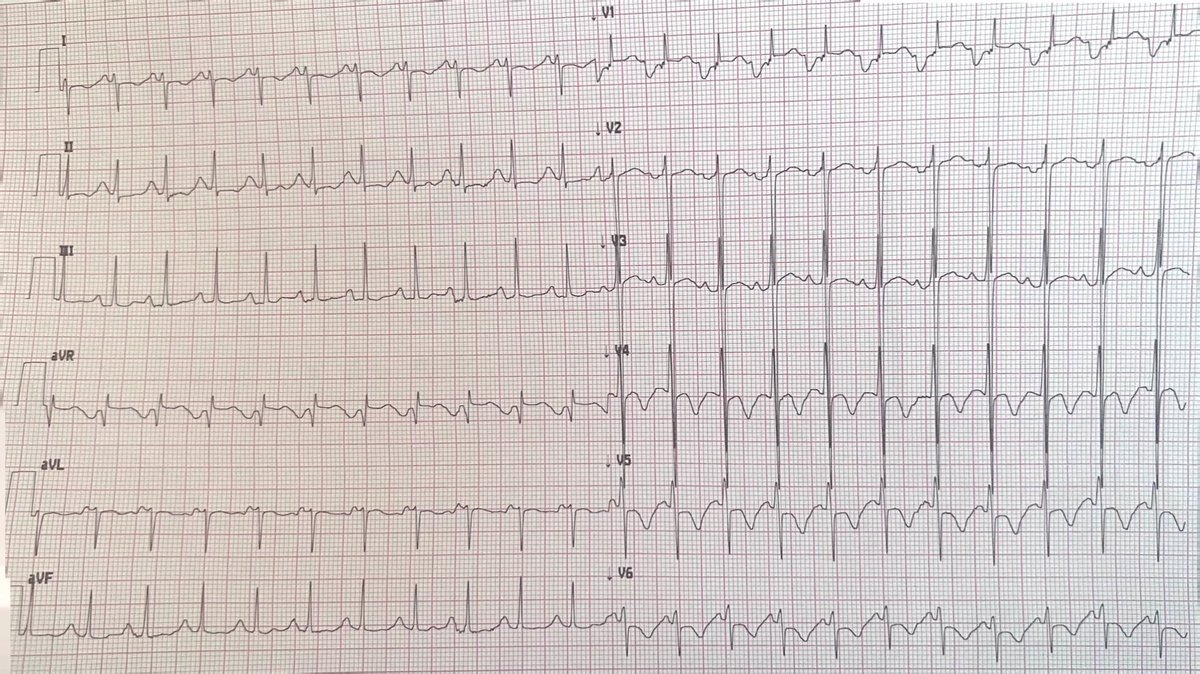
#ImageOfTheWeek by Raid Faraj, Nouhaila Lahmouch and Jamila Zarzur, from the Cardiology B department, Ibn Sina university hospital, Mohammed V university, Rabat, Morocco, sent this question:
A 26-year-old male, with a history of anabolic steroid use, presents with chest pain. What anomaly is identified on coronary angiography? https://t.co/tfm0aTIkBm
#cardioed #ESCYoung #cardiology
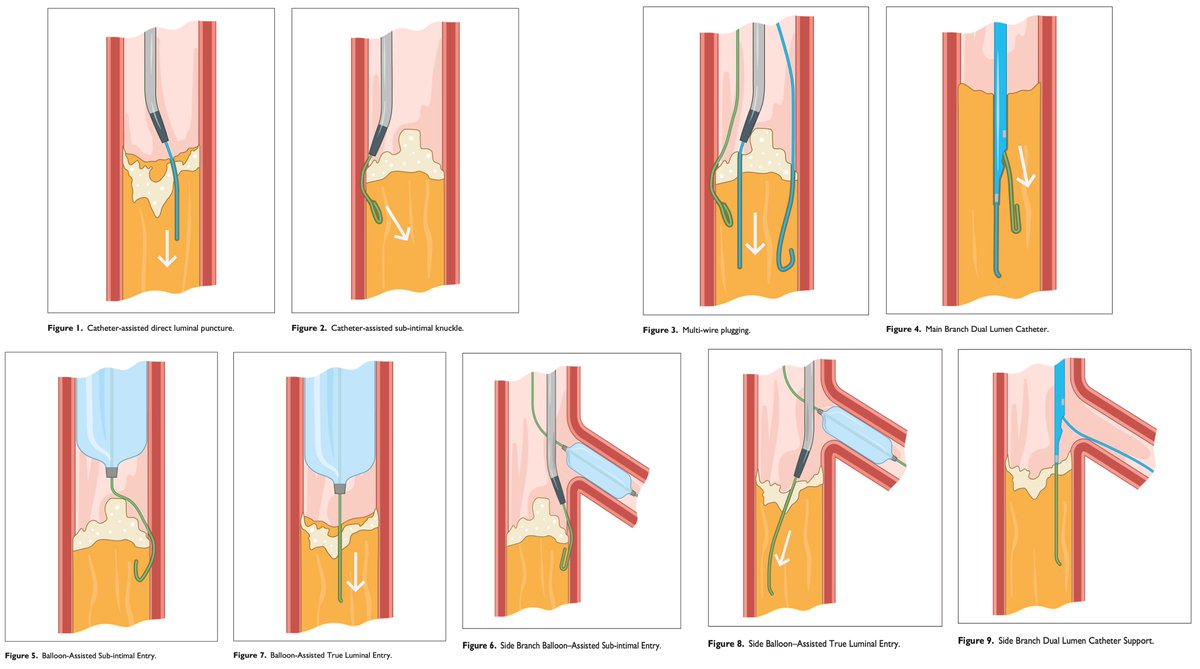
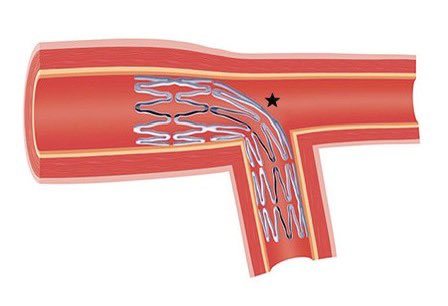
@FBardooli@jedicath IMHO, Culotte may not be the ideal choice for wide-angle bifurcations for which ⬆️ stent distortion to accommodate the SB (LCx) is required.
⬆️ distortion can result in stent under expansion, malapposition, and eventually ISR.
@Ryvetsprog
@EuroInterventio 2022;18:e273-e291
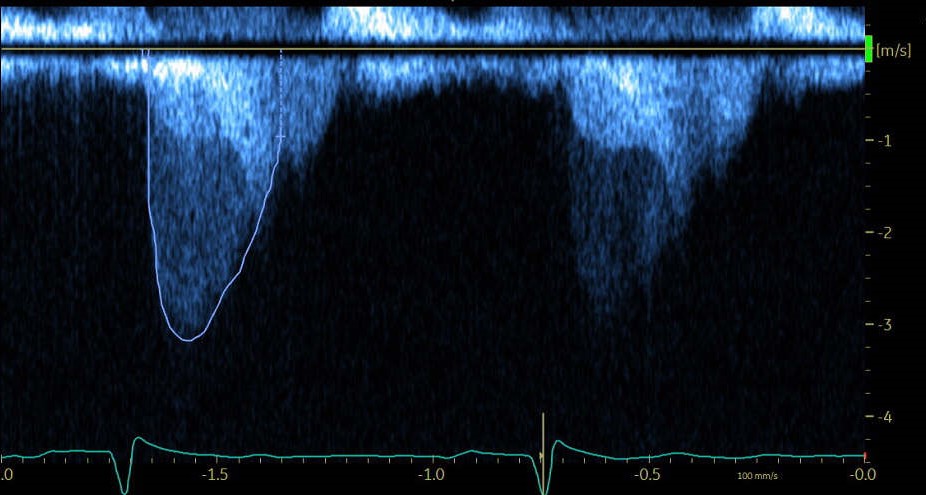
@DrRajeshG1@mandeep_mayo@echotalk@Ahmed43101178 That's what we thought. We will proceed with a cardiac MRI. I still have some questions:
- How can we have such an elevated mitral gradient even if the LA is huge + diastolic dysfunction due to LVH?- How can the RV function be good even if the sPAP is extremely high?
Thank you 🙏🏻
@mandeep_mayo@DrRajeshG1@echotalk@Ahmed43101178 We've confirmed that there is no hypertension. It might be the coexistence of RHD and HCM. We will proceed with a cardiac MRI.
Thank you for your answer 🙏🏻