Ejercicio & prueba de esfuerzo en el Sx de Brugada. 🏃♂️🫀⚡️
🔹 El momento clave no es el ejercicio, sino la recuperación. Solo ~1% de los pacientes desarrolla patrón tipo 1 durante el esfuerzo, mientras que hasta 25.5% lo manifiesta en la fase de recuperación, cuando ocurre el rebote vagal tras el retiro del estímulo simpático. 🤔🏃♂️⏱️
🔹 La recuperación temprana (primeros 2-3 minutos) es la ventana más importante. Es aquí donde pueden aparecer el patrón tipo 1 de Brugada, elevación del ST/J-point, extrasístoles ventriculares, TV o FV en pacientes de alto riesgo. 🧐⚠️⚡️
🔹 Se asociaron con mayor riesgo de eventos arrítmicos: Aumento del ST durante la recuperación, extrasístoles ventriculares entre 1.5 y 3 minutos de recuperación, recuperación rápida de la FC (marcador de hiperactividad vagal), prolongación de la pendiente ascendente de la onda S en ejercicio máximo. 👨⚕️📝
📄🆓️⤵️ State-Of-The-Art Review 2026 @JACCJournals 👌🏻💯
https://t.co/pKL8FJz2HZ
https://t.co/4PnV0aMMfn
🫀MINOCA is finally entering the era of precision medicine.
The PROMISE trial is the first randomized study showing that a structured diagnostic approach with mechanism targeted therapy improves outcomes in patients with myocardial infarction and non obstructive coronary arteries (MINOCA).
The most important finding was not mortality.
It was diagnostic clarity.
Using OCT, vasoreactivity testing, CMR, and embolic evaluation, investigators identified the underlying mechanism in 80% of patients and reclassified the initial diagnosis in 75.5%.
The most frequent mechanisms were:
• Epicardial spasm: 35.6%
• Plaque instability: 22.2%
• SCAD: 13.3%
This matters because MINOCA is not one disease.
Treating vasospasm, embolism, SCAD, and plaque rupture with the same empirical post MI regimen may be ineffective or even harmful. The paper specifically highlights that beta blockers may worsen vasospastic disease, while antiplatelet therapy alone may be inadequate in coronary embolism.
The intervention improved Seattle Angina Questionnaire scores by +9.38 points, exceeding the clinically meaningful threshold.
One major message from this trial: MINOCA should no longer be considered a “diagnosis.”
It is a working syndrome that demands phenotyping.
Future ACS pathways may increasingly incorporate:
• routine CMR
• intracoronary imaging
• vasoreactivity testing
• mechanism specific therapy
This is likely the beginning of a major paradigm shift in ischemic heart disease.
Reference 📚
Montone RA et al. Stratified treatment of myocardial infarction with non obstructive coronary arteries: the PROMISE trial. European Heart Journal. 2026;47:1456–1466. https://t.co/5vXc6Qy8Q9
EKG: patrones de sobrecarga sistólica & diastólica. ⚡️🫀💢
🔵La sobrecarga sistólica se pone de manifiesto en el VD por presencia de onda R alta en V1 con onda T negativa asimétrica, mientras que la sobrecarga diastólica se presenta como patrón rsR' con T negativa asimétrica en V1.
🔵En el caso del VI, la sobrecarga sistólica se registra como una onda R alta con onda T negativa y asimétrica en V5-V6, y la sobrecarga diastólica como presencia de qR de gran voltaje con T positiva alta y picuda en V5-V6.
🔹️Actualmente se considera que independientemente de la cardiopatía de base la imagen electrocardiográfica de sobrecarga diastólica suele corresponder a fases ligeras o moderadas de crecimiento ventricular y la imagen de sobrecarga sistólica suele aparecer en fases más avanzadas de crecimiento ventricular.
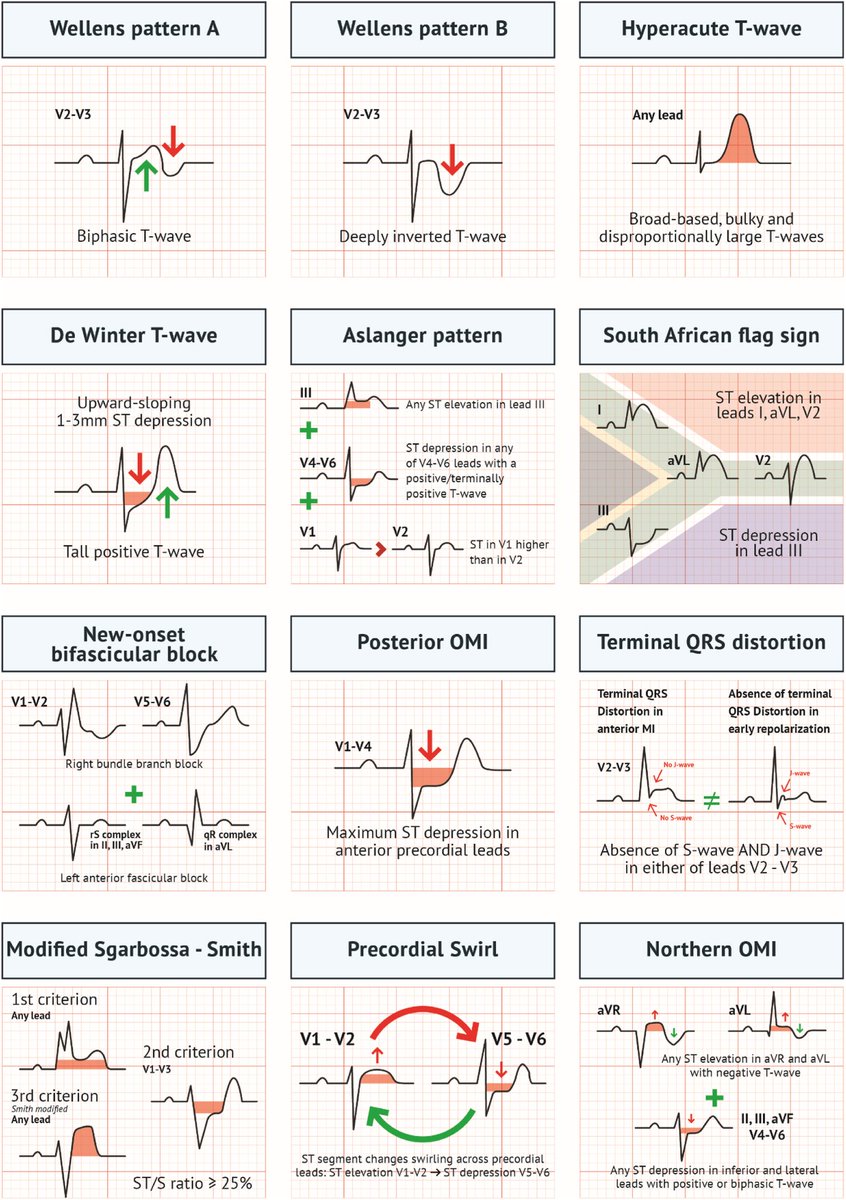
Acute MI is not always STEMI.
A major 2025 review highlights why relying only on classic STEMI criteria can miss dangerous coronary occlusions.
A thread on OMI (Occlusion Myocardial Infarction): 🧵
💊 Practical algorithm for diuretic resistance in acute HF from #HeartFailure26— this is the slide to save!
Start: Furosemide 120-160 mg
↓ Still congested?
Add Chlortalidone 12.5-50 mg/24h
↓ Still congested?
Tailor to the problem:
• Metabolic alkalosis → Acetazolamide 120-500 mg/24h
• Hyponatremia → Tolvaptan 15-50 mg/24h
• rLVEF + hypopotassemia → MRA 25-100 mg/24h
And running through the whole algorithm:
➕ Add iSGLT2 throughout
➕ Add sacubitril/valsartan if LVEF <49%
➕ Consider parenteral route if oral absorption is the issue
Clean. Practical. Evidence-based. 💯
(Adapted from de la Espriella R et al. Nefrologia 2021)
#CardioTwitter #HeartFailure #Cardiology #Diuretics #HFrEF
Myocardial Performance Index (Tei Index)= Interesting one 😍
The Tei Index, named after Dr. Chuwa Tei is a Doppler-based, noninvasive measure of global ventricular function, combining both systolic & diastolic performance.
How it’s measured:
⬜ Obtained using pulsed and continuous wave Doppler of mitral inflow (A4C view) and LV outflow (A5C view).
⬜ Key time intervals are measured:
a. IVCT ➡️ Isovolumetric Contraction Time
b. IVRT ➡️Isovolumetric Relaxation Time
c. ET ➡️ Ejection Time
Formula:
Tei Index = (IVCT + IVRT) / ET
or
Tei Index = (a - b) / b
a = time from mitral valve closure to opening
b = aortic ejection time
Normal Values:
LV Tei Index: ≤ 0.40
RV Tei Index: ≤ 0.43
Interpretation:
🔵 Higher Tei Index = Worsening ventricular function
🔵 Sensitive for detecting early dysfunction, even when LVEF is preserved.
Clinical Significance:
- Helpful in evaluating cardiomyopathies, heart failure, congenital heart disease, and transplant rejection.
- Valuable in both pediatric and adult cardiology.
(Ref: Bulwer BE & Solomon SD. In Essential Echocardiography: A Companion to Braunwald’s Heart Disease. Elsevier, 2019)
CMR LGE patterns in myocarditis — know the difference. 🧵
Cardiac MRI is your most powerful non-invasive tool. But LGE location varies dramatically by subtype:
🔴 Giant Cell (GCM) — Multifocal, patchy LGE with septal involvement + “Hook sign”
🟠 ICI-related — LGE can be absent at presentation; no specific pattern, often mid-myocardial
🟡 Allergic/Eosinophilic — Circumferential or multifocal subendocardial LGE; may extend transmurally
🔵 Systemic IMIDs — Patch, mostly subepicardial; mid-wall LGE often basal-lateral
🟣 Pathogenic DSP — Extensive circumferential, ring-like LGE; septal involvement
💡 Key pearl: ICI-myocarditis can be CMR-negative early — don’t let a normal LGE falsely reassure. EMB remains the gold standard.
#Cardiology #CardiacMRI #Myocarditis #LGE #MedEd #MedTwitter