Excited to share that this work is finally published.
Proud and grateful to share this milestone with the community.
Mitigating conduction disturbances in sutureless aortic valve surgery: A standardized anti-oversizing strategy… JTCVS Open https://t.co/bmELOQcvfC
.@gagobar96: "Antiguamente, la participación en deportes competitivos de pacientes con defectos complejos era algo anecdótico, pero las mejoras en el tratamiento han permitido que cada vez más personas con cardiopatía congénita puedan alcanzar estos niveles de manera segura". #BlogSEC @jovenesSEC https://t.co/S6aM74B5ur
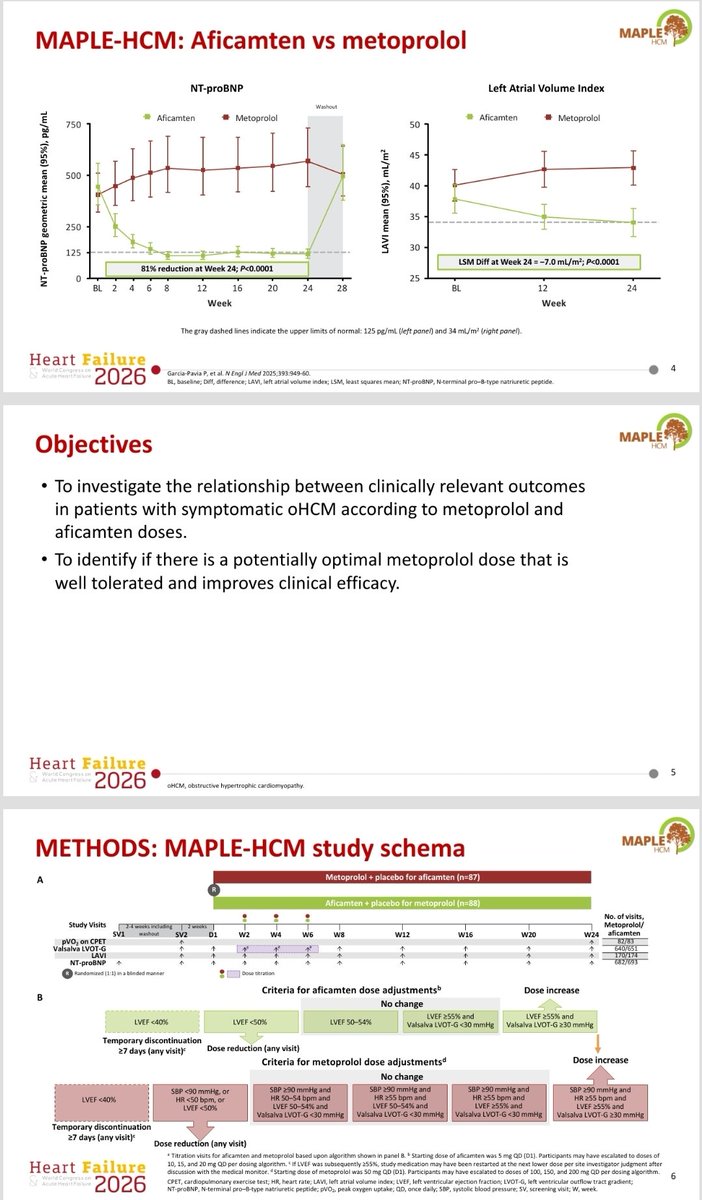
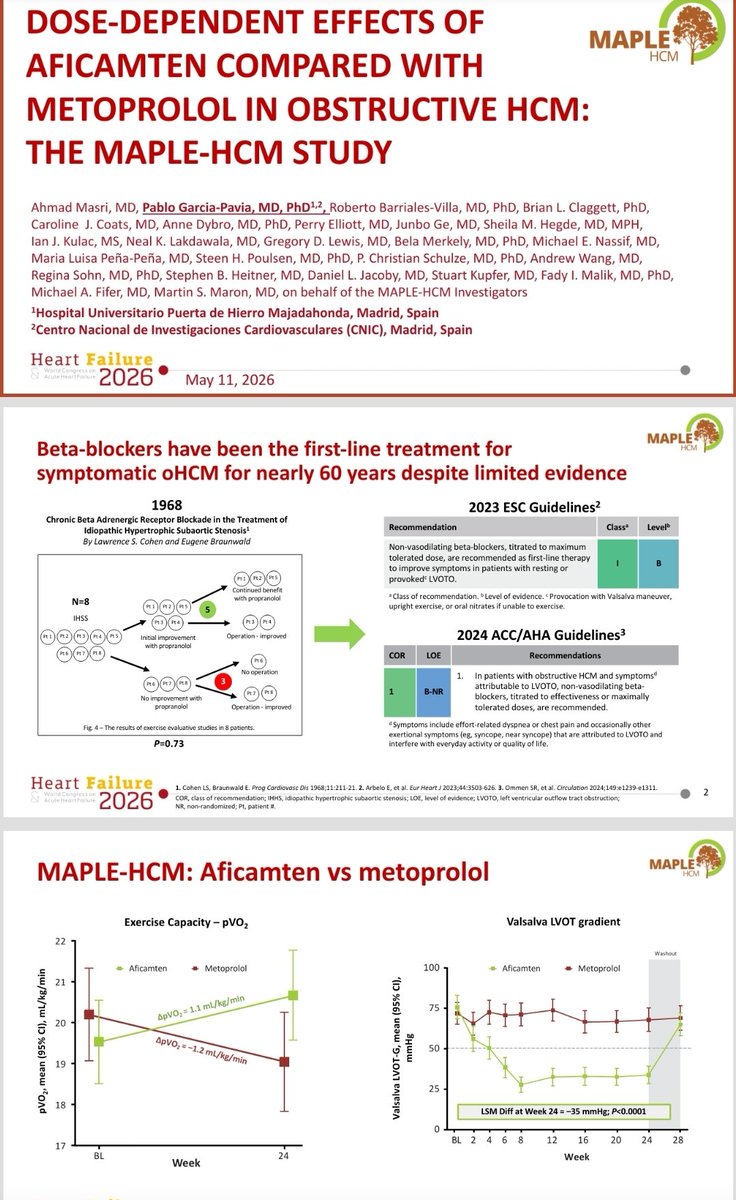
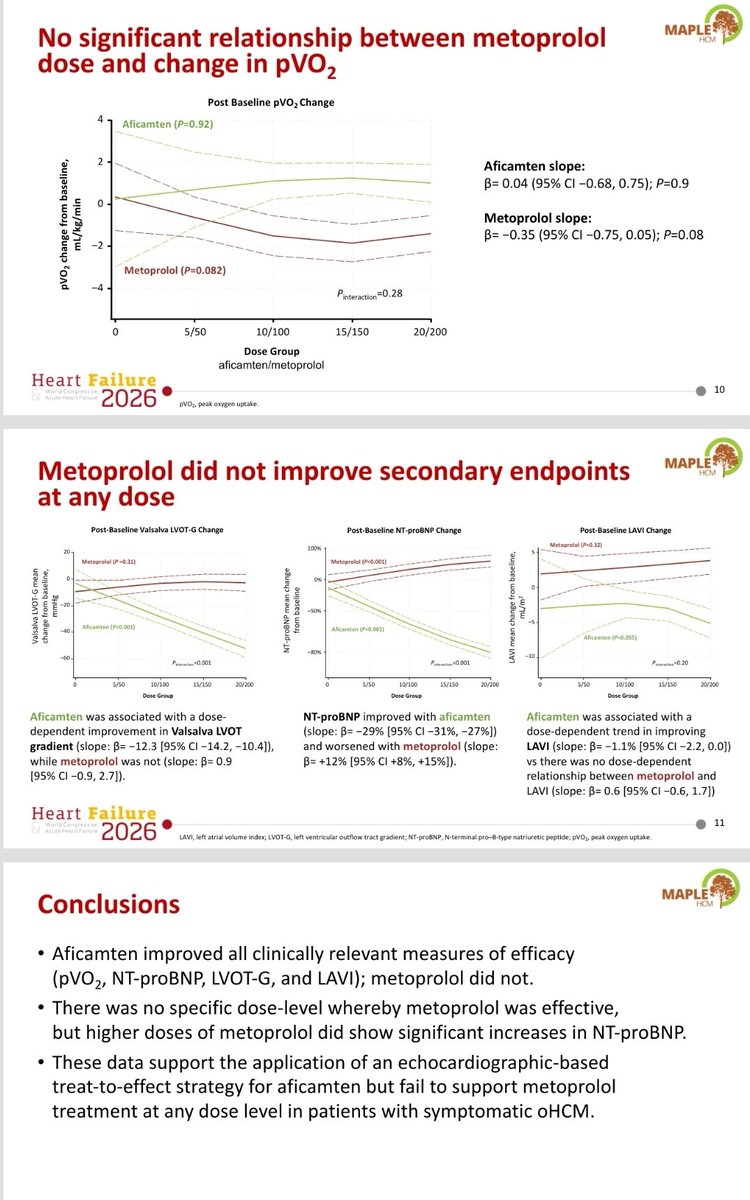
MAPLE-HCM showed that metoprolol as a BB is harmful. In this complementary analysis presented by @dr_pavia#Heartfailure2026#HFA2026 we showed that the lack of benefit was not a dose dependent finding. More in the slides
#CardioTwitter
🚨 Return-to-Play in Desmosomal Arrhythmogenic Cardiomyopathy 🫀🏃♂️
A new study explores one of the most difficult questions we face in clinical practice:
👉 Can patients with arrhythmogenic cardiomyopathy safely continue sports?
In this cohort of genotype-positive athletes:
🔹 25% experienced cardiac events after diagnosis
🔹 Event rates were higher after return-to-play (RTP)
🔹 But importantly… only ~50% of events occurred during exercise
🔹 The rest happened at rest or in unclear contexts
➡️ This challenges the traditional idea that exercise is always the main trigger
➡️ And reinforces the complexity of this disease
Even more interesting:
✨ Some athletes were able to return to sport with careful evaluation and shared decision-making
✨ Phenotype-negative patients showed a much lower short-term risk
📊 Overall, this study highlights the need for:
✔️ Personalized risk stratification
✔️ Close follow-up
✔️ Honest, shared decisions with patients
📄 Based on:
https://t.co/G3BNq910pj
💭 And here comes the real question…
Will there ever be hope for safe physical activity in these patients?
Honestly… I have a gut feeling that the answer is yes.
Not for everyone, not without risks… but with better understanding, genetics, imaging, and tailored care —
✨ we may be moving from restriction to precision medicine
And maybe… one day…
👉 from fear to possibility
#Cardiology #ArrhythmogenicCardiomyopathy #SportsCardiology #Genetics #PrecisionMedicine #CMR #CardioTwitter #MedTwitter #HeartRhythm #SuddenCardiacDeath #Research #SharedDecisionMak
Day 3… And last (but not least)… more insights on the way.
Small incision, big impact: efficient, reproducible early outcomes in the largest single-center sutureless AVR series.
Grateful to #AATS2026 for the opportunity to share over a decade of experience with sutureless Vvs.
Presenting now and newly published in #JTCVS Open: Mitigating Conduction Disturbances in Sutureless Aortic Valve Surgery: A Standardized Anti-oversizing Strategy in a Large Single-Centre Program. @barbeito_g, Castillo, et. al. Read more: https://t.co/JCKPqEL04N
🚸 New AHA Statement: Let kids with cardiomyopathy MOVE! ❤️🔥
For years, children with cardiomyopathies were often told to avoid physical activity due to fear of sudden cardiac death ⚠️
👉 But new evidence is changing the paradigm:
✅ Physical activity is essential for cardiovascular, emotional & social health
✅ Risk during exercise may be lower than previously thought in selected patients
✅ Exercise can even support functional improvement & reverse remodeling
✅ Sedentary lifestyle = higher risk of obesity, hypertension & poor QoL
💡 The key message:
➡️ Individualised risk stratification + shared decision-making = safe participation for most patients
⚖️ Not “restrict vs allow” — but tailored prescriptions based on phenotype, genotype & patient goals
👨👩👧👦 Let’s move from fear to empowerment
📄 Read the full statement here: DOI: 10.1161/CIR.0000000000001431
#Cardiology #PediatricCardiology #Cardiomyopathy #AHA #SportsCardiology #ExerciseIsMedicine #SharedDecisionMaking #CMR #Genetics #HeartHealth 💙
🏃♂️🫀 Exercise Prescriptions Should Be Risk-Stratified — Not Generic
Current guidelines recommend ≥150 min/week of moderate-to-vigorous physical activity (MVPA) for everyone.
But is that optimal for a 45-year-old low-risk individual and a 70-year-old very high-risk patient?
This large UK Biobank cohort (72,884 participants, median 13.2-year follow-up) provides a more nuanced answer .
🔬 What’s innovative?
• Objective 7-day wrist accelerometer data
• ESC-aligned SCORE2 risk stratification
• Isotemporal substitution modeling (reallocating sedentary time)
• Identification of optimal vigorous activity thresholds by risk group
📊 Key findings
Each +150 min/week MVPA →
• 20% lower CVD risk in very high-risk individuals
• 16% reduction in high- and low-to-moderate-risk groups
Higher-risk individuals benefit the most from increasing activity.
BUT intensity matters.
When replacing 300 min/week sedentary time:
🔹 Low-to-moderate risk → Any mix of moderate (MPA) and vigorous (VPA) works. More VPA = more benefit.
🔹 High risk → VPA should be ≤60 min/week (~20% of MVPA).
🔹 Very high risk → Optimal VPA ≈ 42 min/week (~14% of MVPA). Beyond that, benefits decline.
In high-risk groups, excessive VPA may attenuate benefit—likely due to hemodynamic stress, endothelial dysfunction, and oxidative burden.
🎯 Take-Home Messages
1️⃣ Physical activity remains powerfully protective across all risk strata.
2️⃣ Higher-risk patients gain the largest relative benefit.
3️⃣ Vigorous exercise has a ceiling effect in high-risk individuals.
4️⃣ Exercise prescriptions should integrate formal risk stratification (e.g., SCORE2).
Precision prevention now extends to lifestyle medicine.
One size does not fit all.
🏃♂️❤️ Should ECG screening be mandatory for all competitive athletes? The ACC says no.
Sudden cardiac arrest (SCA) is the leading medical cause of death during competitive sports. Screening aims to detect silent conditions — and adding a 12-lead ECG to history & physical can increase detection sensitivity to >90% for certain diseases.
So why oppose mandatory ECG laws?
The American College of Cardiology argues that legislative mandates would likely cause more harm than benefit .
⚖️ The core concerns:
1️⃣ Workforce reality
Accurate athlete ECG interpretation requires expertise. The U.S. does not have enough trained sports cardiologists to handle universal screening volumes. Poor interpretation → false positives, false negatives, unnecessary testing, missed diagnoses.
2️⃣ Equity risk
False-positive rates (2–15%) disproportionately affect Black athletes and those from underserved communities. Mandates could widen disparities, increase financial strain, and delay care.
3️⃣ Resource diversion
Mass ECG programs are expensive. Funds may shift away from what actually saves lives:
🚨 Emergency Action Plans (EAPs)
Immediate CPR + AED access is the only intervention proven to reduce mortality in young athletes.
4️⃣ Screening limits
Not all lethal conditions are detectable by ECG. A normal ECG does not eliminate future risk.
📌 ACC position:
ECG screening may be reasonable in structured programs with:
✔ Expert interpretation
✔ Equitable downstream resources
✔ Clear implementation planning
But laws mandating universal ECG screening are not evidence-based policy.
Prevention isn’t just about detecting risk.
It’s about implementing what truly saves lives.
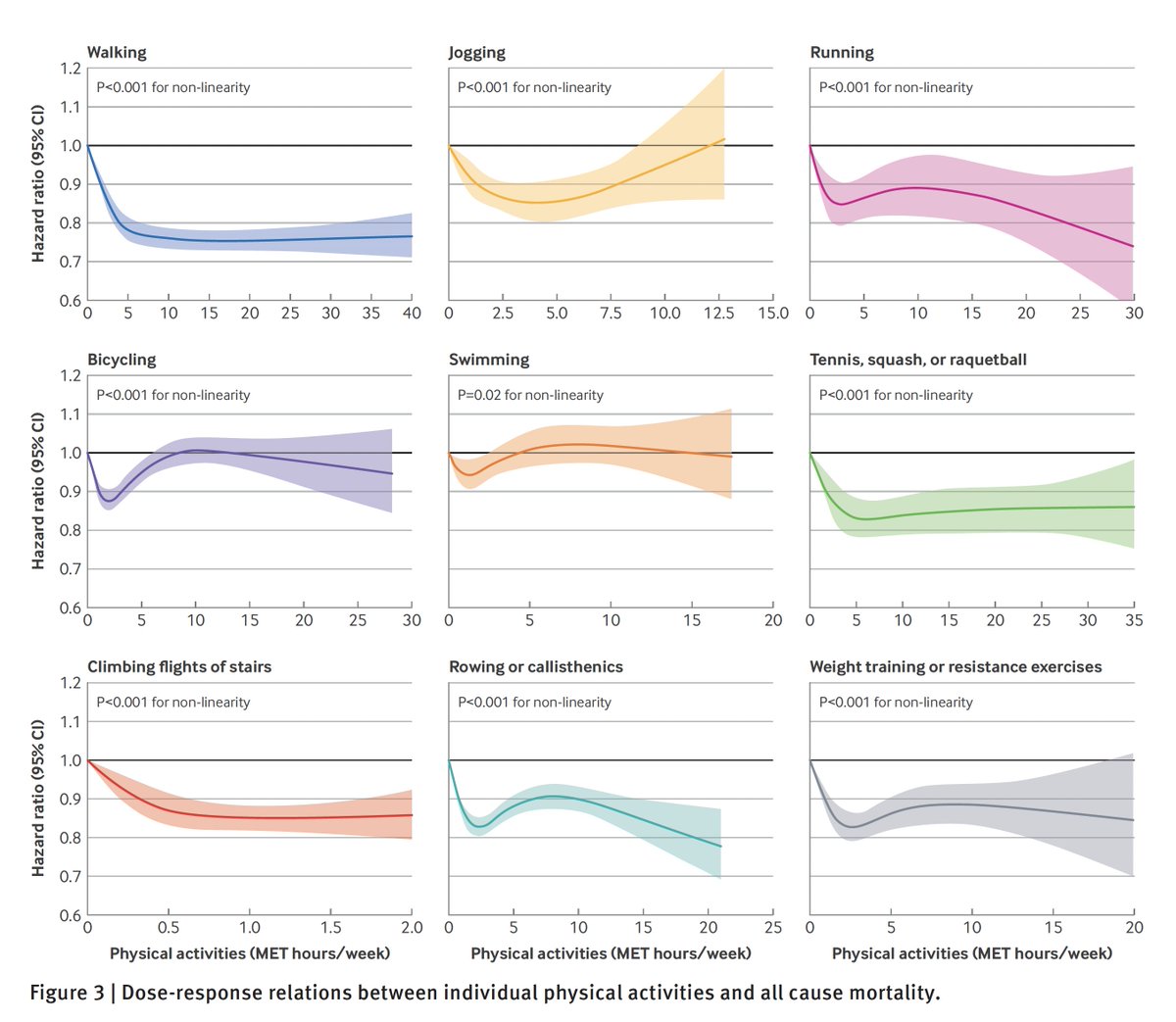
Physical activity and the reduction of all-cause mortality, from 2 very large prospective cohorts
1. The relationship is non-linear, suggesting a threshold effect for many types of exercise as seen below
🧵 Lo que un ultramaratón le hace realmente a tu cuerpo (y por qué la distancia sí importa)
💥 Nuevo estudio en ultrarunners (100 km, 160 km y 230 km).
Resultados: tu cuerpo entra en modo supervivencia metabólica, da igual la distancia. Pero cuanto más largo… peor👇
🫀🫶🏻¿CUÁL ES EL MEJOR TIPO DE EJERCICIO FÍSICO PARA LA LONGEVIDAD?
💪🏻Sólo entrenamiento de fuerza =
⇩ ⇩Reducción del 9-22% de la mortalidad.
🏃Sólo entrenamiento cardiovascular=
⇩ ⇩Reducción del 24-34% de la mortalidad.
🤝Entrenamiento de fuerza + cardiovascular= ⇩ ⇩Reducción del 41-47% de la mortalidad.
Our work stablishing the HCM-phenotype associated with p.Asn271Ile variant in TNNT2, a founder variant in A Coruña, is finally out in @JACCJournals https://t.co/a4Du2teTNK @rbarvil@jpocardio@LRGuerr
La “respuesta de la esgrima” es un reflejo involuntario debido a un impacto craneal de gran intensidad. Se puede ver en deportes de contacto/pelea y sugiere daño cerebral secundario al traumatismo.
Consiste en la extensión de un miembro + flexión del contralateral ⬇️⬇️⬇️
Watch Trevor Lawrence immediately after this horrific hit. His right arm suddenly flexes as his left arm simultaneously extends. This is known as the “fencing posture”—an involuntary reflex that occurs after impact in blunt head trauma. It signifies a traumatic brain injury with loss of consciousness and represents a severe concussion. Prayers up for Trevor.
Medidas a tomar en una parada:
✅ Reconocer y pedir ayuda
✅ RCP PRECOZ (lo más importante)
✅ Desfibrilación precoz (si oportuno)
❌ EVITAR QUE LA PERSONA SE TRAGUE LA LENGUA
Hay que acabar con este mito, en caso de respirar —> POSICIÓN DE SEGURIDAD
El futbolista Edoardo Bove, sedado y en cuidados intensivos tras desplomarse en el Fiorentina-Inter. La causa del colapso pudo ser un golpe en el torso que sufrió minutos antes de que entrase en parada cardiorrespiratoria @vozdeportes https://t.co/gEwD5ytz7M
Después de unos días escuchando hablar de la importancia de la zona 2 en #ErgoDonostia2024 tocaba ponerlo en práctica.
Mejorar la recuperación, el rendimiento deportivo, pero también (y muy importante) la capacidad funcional de los pacientes.
El pan nuestro de cada día en rehabilitación cardíaca. Paciente con DM1, IAM inferior reciente, FEVi normal y enfermedad de 3 vasos. Le tratan la culpable (CD) y una DA severa. Se deja sin tratar una bisectriz severa con buen lecho (desconozco el motivo, mañana lo revisaremos en sesión con Hemodinámica) El paciente está libre de angina (como lo estuvo el día del IAM: DM1) En la #CPET pre #RehabilitaciónCardíaca hace esto que veis. Un Bellardineli de libro...Además, a 122 lpm, antes de VT2, en su zona sensible de entrenamiento. La prueba, clínica y ECG NEGATIVA. Con una ergo normal, "nos la comemos", y le estaremos entrenando en zona de inducción de isquemia - inducción de disfunción de VI. Además, con FEVi normal, a lo mejor hasta le planteamos un programa domiciliario....no supervisado. De nuevo, la importancia de LA #CPET en #RehabilitaciónCardíaca, muy superior a la ergometría convencional para todo: detección de isquemia, valoración CF, mecanismos deterioro funcional y diseño de entrenamiento. Si queréis saber más....nos vemos en #ErgoDonostia2024 !!! 6-7 noviembre 2024