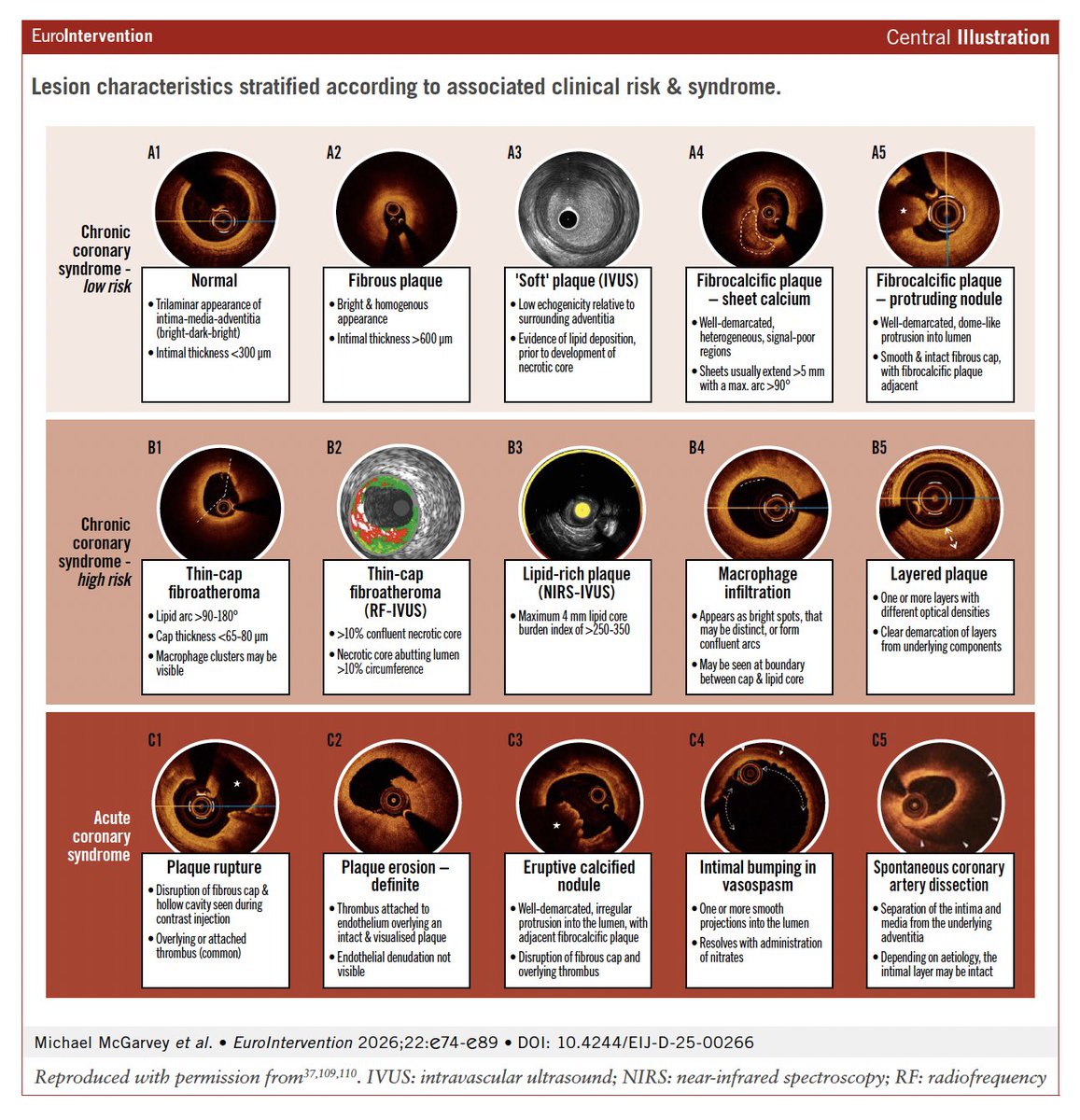
In this new State-of-the-art paper, the authors review the evidence and guideline support for intracoronary imaging in contemporary clinical practice, and outline a modern, imaging-driven approach to PCI planning.
https://t.co/YUCGlkT9Et
Cardiogenic shock is associated with high early mortality. Prompt revascularization in infarct-related cardiogenic shock improves outcomes, and mechanical circulatory support may reduce mortality in specific groups.
Read the Review Article “Cardiogenic Shock” by Holger Thiele, MD (@thiele_holger), and Christian Hassager, MD, from Heart Center Leipzig at Leipzig University, Leipzig Heart Science, Rigshospitalet, and the University of Copenhagen (@koebenhavns_uni): https://t.co/V9IfEFDaYw
📚Ya está disponible la actualización 2025 de la Guía ESC 2019 sobre el manejo de las dislipemias.
🎯 Actualiza los objetivos terapéuticos
💊 Refuerza y optimiza las estrategias de tratamiento
➡️ Mejora el abordaje integral del riesgo cardiovascular
📄 Puedes descargarla aquí: https://t.co/neb4ParS16
@VDelgadoGarcia
🔥🫀 Inflammation is no longer a hypothesis—it’s a therapeutic target
The 2025 ACC Scientific Statement on Inflammation and Cardiovascular Disease marks a turning point: inflammation is now recognized as a causal, measurable, and actionable driver of cardiovascular risk, not just a bystander .
🧠 Key paradigm shift
Even in statin-treated patients with optimal LDL-C, residual inflammatory risk—best captured by high-sensitivity C-reactive protein (hsCRP)—strongly predicts recurrent events and cardiovascular death. In fact, post-statin hsCRP is often more prognostic than LDL-C itself.
📏 Measure what you want to treat
The statement makes a bold recommendation:
👉 Near-universal hsCRP screening in both primary and secondary prevention.
hsCRP <1 mg/L → low risk
1–3 mg/L → intermediate risk
3 mg/L → high inflammatory risk
Persistently elevated hsCRP (>2 mg/L) identifies patients who remain vulnerable despite guideline-directed therapy.
💊 Anti-inflammatory therapies: what works (and what doesn’t)
❌ Broad immunosuppression failed (e.g. methotrexate in CIRT).
✅ Targeted inflammation inhibition works:
Canakinumab (CANTOS) proved the inflammation hypothesis—reducing events without lowering LDL-C.
Low-dose colchicine (0.5 mg/day) reduced recurrent CV events by ~25% and is now FDA-approved for secondary prevention.
🚧 New frontiers: IL-6 inhibition (ziltivekimab, clazakizumab) in CKD, HFpEF, ACS—results expected soon.
🧘♂️ Lifestyle is anti-inflammatory medicine
Mediterranean/DASH diets 🥗, omega-3 intake 🐟, exercise 🏃♀️, weight control, and smoking cessation are explicitly framed as anti-inflammatory interventions, not just “healthy habits.”
🖼️ Imaging: promising, not ready
Advanced imaging of vascular inflammation (e.g. perivascular fat attenuation index) is exciting—but not yet for routine clinical use.
🔮 Bottom line
Atherosclerosis is an inflammatory disease with lipid involvement.
The time has come to treat cholesterol and inflammation—with biomarkers, lifestyle, and targeted therapies—moving cardiovascular prevention into a new era 🚀
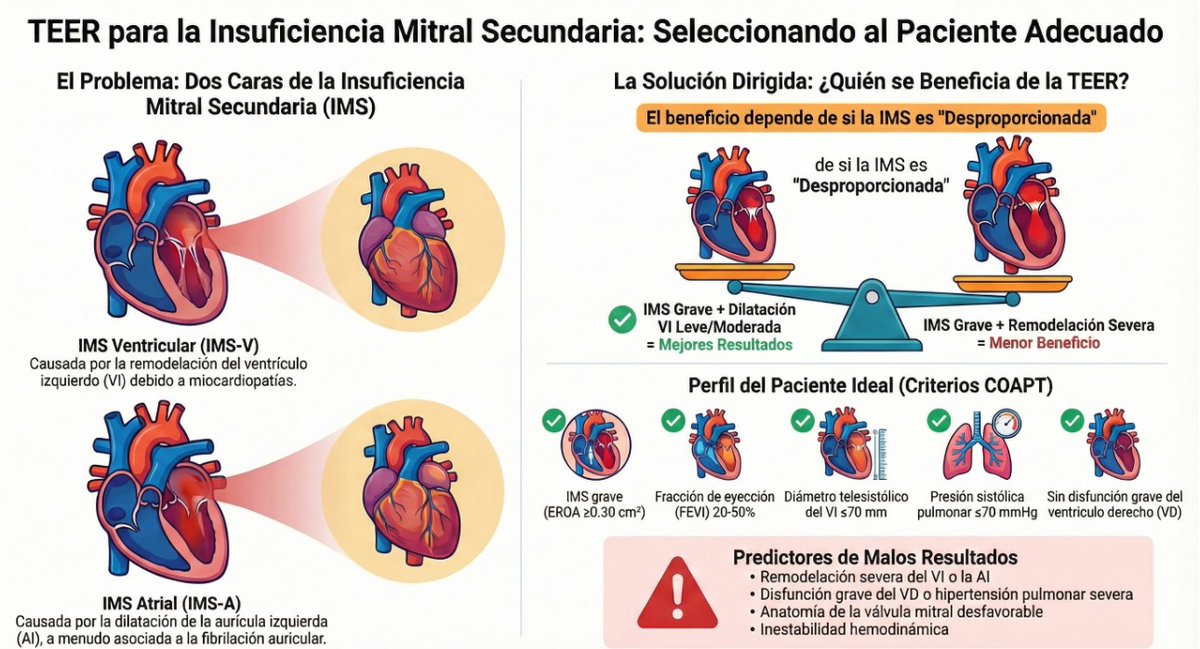
🆕 Reparación mitral percutánea borde a borde en la insuficiencia mitral secundaria: a quién, cuándo y por qué.
📕 EuroIntervention
🔓 Resumen del artículo en https://t.co/pIFbVyAd1T
1. Unpaywall — unpaywall . org
Extensión para Chrome y Firefox. Identifica versiones gratuitas y legales de artículos científicos en sitios de revistas. Accede al texto completo directamente desde la página del artículo si existe una versión en acceso abierto.
2. Open Access Button (OAB)
Plataforma que permite buscar artículos por DOI o URL. Si el documento está disponible en algún repositorio, lo muestra. Además, si no está disponible, te da la opción de solicitarlo directamente al autor.
openaccessbutton. org
3. PaperPanda
Extensión para navegador (Chrome) que funciona de forma similar a Unpaywall. Detecta DOIs automáticamente en páginas académicas y busca versiones gratuitas. Ideal para estudiantes e investigadores.
paperpanda . app
4. DOAJ (Directory of Open Access Journals)
Base de datos que indexa más de 20,000 revistas científicas de acceso abierto revisadas por pares. Puedes buscar por tema, título de revista, idioma, etc.
5. OA (.) mg
Buscador de artículos científicos con más de 250 millones de documentos. Permite acceder a versiones en acceso abierto y enlaces a repositorios. Su diseño es simple e intuitivo, como un “Google académico mejorado”.
7. CORE — core(.)ac(.)uk
Uno de los mayores repositorios de artículos científicos del mundo. Más de 298 millones de documentos indexados de universidades, revistas y repositorios institucionales. Ideal para revisiones sistemáticas y tesis.
Non-ST-segment elevation acute coronary syndrome: understanding the full spectrum to guide management. Read this State-of-the-Art review in #EHJ 👉 https://t.co/Z4IodPvslr
@RoccoMontone@ehj_ed#acutecoronarysyndrome
In older patients with frailty who were receiving antihypertensive drugs and had a systolic blood pressure below 130 mm Hg, reducing antihypertensive drugs did not lead to lower all-cause mortality over 4 years than usual care. Full RETREAT-FRAIL trial results and Research Summary: https://t.co/xRdZMaEAYd
Guía básica para leer una revisión sistemática + metaanálisis y aplicar los resultados a los pacientes.
Una guía obligada para los profesionales de la salud.
https://t.co/uGgEd3p9BF
Aplicaciones clínicas de la ecocardiografía de deformación miocárdica: Declaración de consenso clínico ASE/EACVI-ESC
👓 https://t.co/QdwujmgqDc ◀️
Primera publicación de la nueva sección "García Fernandez te pone al día"...
¡No te lo pierdas!
Beta-blocker use after myocardial infarction reduces the risk of death in patients with a reduced ejection fraction, but its benefit is less clear in patients without a reduced ejection fraction. Research findings from the REBOOT trial are summarized in a new Quick Take video. https://t.co/05LMiS4iRP
🚀 Calcium Score & CCTA: Key Highlights from the 2025 AHA Scientific Statement (DOI: 10.1161/CIR.0000000000001394)
Non-obstructive CAD in Chest Pain Patients
🧊 1. CAC = Atherosclerotic Burden, Not Just a Number
CAC is one of the strongest predictors of future ASCVD risk—better than biomarkers or stenosis alone.
📉 CAC = 0 → high NPV for obstructive CAD (but not zero risk: ~10% still have non-calcified plaque, especially if young or high-risk).
🔥 CAC ≥1000 = extreme risk → annual CV mortality similar to 2ndry prevention populations.
📊 CAC → intensity of preventive therapy: from lifestyle (CAC 0) → to statins (CAC ≥100) → to high-intensity LLT + aspirin (CAC ≥300).
🧮 2. CAC for Risk Upgrading & Therapy Decisions
CAC ≥100 or ≥75th percentile supports starting statins even in borderline/intermediate-risk patients.
- hidden high-risk phenotypes (eg, DM or preDM patients with CAC ≥100).
🌈 CAC from non-gated PET/SPECT CT is increasingly used and correlates well with dedicated CAC scans.
🫀 3. CCTA: The New Backbone of Chest Pain Evaluation
The 2021 Chest Pain Guidelines expanded CCTA → leading to a surge in detecting nonobstructive CAD (NOCA).
CCTA is essential because:
- plaque beyond the lumen (including noncalcified plaque).
- vessels down to ~2 mm (even smaller with photon-counting CT).
- high-risk plaque features (LAP, positive remodeling, spotty calcification).
👁️ CCTA reveals that up to 50% of symptomatic patients have NOCA.
🧨 4. High-Risk Plaque on CCTA = High Future Event Risk
High-risk markers include:
📦 High total plaque volume
🟣 Low-attenuation plaque (>4%)
➕ ≥2 high-risk features (per CAD-RADS 2.0)
🔥 Pericoronary adipose tissue (PCAT) inflammation
These features predict MI better than stenosis, shifting the paradigm from stenosis-centric to plaque-centric care.
📈 5. CCTA-Based Risk Staging (CAD-RADS 2.0 + Plaque Volume)
Stage 0 → no plaque
Stage 1–2 → increasing plaque burden
Stage 3 → high-risk NOCA
🎯 Treatment intensity escalates with plaque volume, not stenosis alone.
🔄 6. CAC + CCTA = The Most Powerful Combination
CAC quantifies calcified burden → great for long-term risk and therapy escalation.
CCTA quantifies total plaque (calcified + noncalcified) → great for short-term event risk.
💡 7. Why This Matters
Most ACS events originate from nonobstructive lesions.
📢 The statement pushes clinicians to:
Detect early plaque (especially noncalcified).
Classify risk by plaque burden + inflammation.
Intensify therapy before stenosis develops.
#PCCT #Atherosclerosis #PhotonCountingCT #CCT #yesCCT
❤️🔥 AHA 2025 – Nonobstructive Coronary Artery Disease (NOCA): Time to Act!
Slipczuk et al., Circulation 2025 🇺🇸
Non obstructive CAD is the modern frontier of atherosclerosis prevention, management, treatment. And Cardiac CT is the epicenter of this paradigm shift.
🎯 What’s new:
Not all chest pain comes from blocked arteries! 🩻
👉 Up to 50% of symptomatic patients have nonobstructive CAD (NOCA) — plaques <50% stenosis but still dangerous 🚨
🧠 Key message:
➡️ NOCA ≠ benign.
Patients with even mild plaque face up to 4× higher MI risk than those with no CAD ⚠️
➡️ Microvascular dysfunction (CMD) affects 30–50% of these patients 💔
🩻 Modern imaging revolution:
CCTA + CAC = new gold standard for detection & risk staging 🪩
AI & plaque quantification (total volume, % low-attenuation plaque, segment score) → better precision 🔬
Photon-Counting CT & AI-QCT identify high-risk noncalcified plaques unseen before 👁️
🔥 High-risk red flags:
🚨 Plaque burden >15%
🚨 Low-attenuation plaque >4%
🚨 Segment involvement >7
🚨 Perivascular inflammation (FAI↑)
🚨 Left main NOCA involvement
💊 Medical management essentials:
Aggressive lipid lowering: statin → ezetimibe → PCSK9i → <55 mg/dL
Anti-inflammatory therapy: colchicine, statins, diet 🌶️
Icosapent ethyl & GLP1-RA = plaque stabilizers
Lifestyle first: AHA Life’s Essential 8 🧘♀️
💬 Why it matters:
👉 ACS often arises from nonobstructive lesions!
👉 Treating NOCA early = preventing tomorrow’s infarctions 💪
👉 Time to bridge the gap between “no stenosis” and “no risk.”
💡 Take-home:
🩻 CCTA & CAC must become routine for chest pain & screening.
🌈 NOCA is a continuum of risk — not a reassurance.
💪 Treat the plaque, not just the stenosis.
📣 #AHA2025 #NOCA #INOCA #ANOCA #CAD #CCTA #PhotonCountingCT #AIQCT #CardiacImaging #PrecisionCardiology #HeartHealth #YesCCT #Cardiology