For evaluating the course of treated Parkinsons disease there is nothing better than the medical interview comparing it with the written previous consultations ( takes 30 minutes) .
The examination is a momentary snapshot.Scales are for trials, wearables a waste of time.
Fact✅ The training places were necessary in the Ten Year plan agreed 12months ago
Fact ✅You have increased medical school places & they will need training
Fact ✅UK has fewer doctors per head of population than peer nations
Fact✅… DHSC lies to the public
FACTS vs FICTION 👇🏻
The cholesterol wars are over.
LDL won.
New guidelines. Four landmark trials. An oral PCSK9 inhibitor that matches injectables. And data proving we should be treating patients we currently aren't.
Here's everything clinicians need to know. 🧵
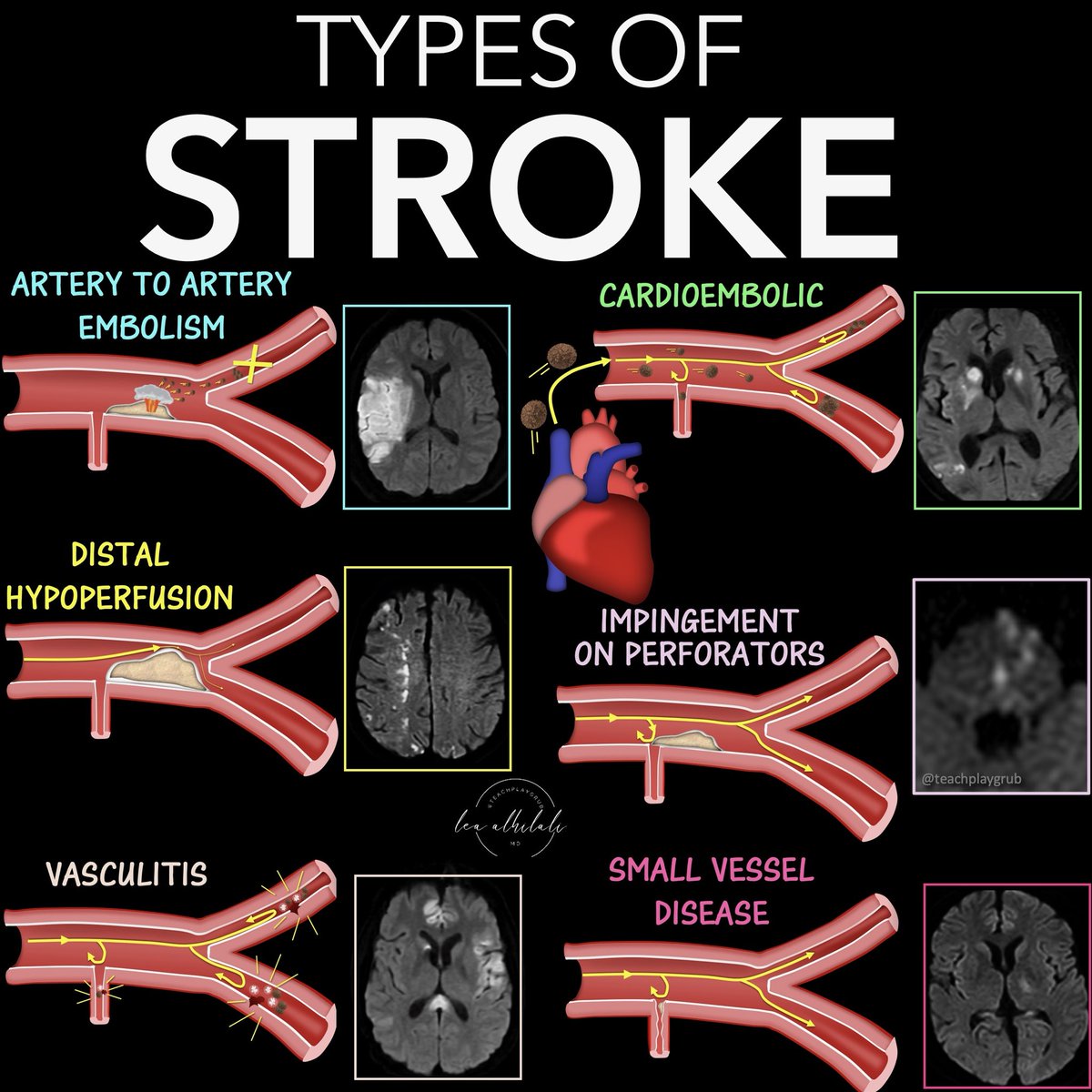
Anyone can see the bright spot on diffusion—what sets you apart is if you can tell them why it’s there!
Can you tell a stroke’s etiology from its appearance on MRI?
Main stroke types:
Artery to artery embolism
—Vulnerable plaque ruptures & causes clot formation
—Occludes the artery & distal blood flow
—Makes a wedge shape
Distal hypoperfusion:
—At the border zones
—Remember borderzones almost look like a fancy letter H for Hypoperfusion = two vertical lines (ant, internal watershed) that have curls at each end (ant & post external watersheds)
Vasculitis
—Inflammation ofvessel wall
—Idiopathic, autoimmune, or infectious
—Remember: Vascu-LIGHT-us = tons of little regions LIGHT up on DWI
—Remember Vascu-LITE-us = usually in LITE vessels or small vessel territories
Impingement on perforators:
—Large vessel plaque covers opening of small perforator in its wall
—Perforators affect the Ps = pons, putamen (lenticulostriate)
Small vessel dz
—Many different pathologies that cause occlusion of small, unnamed vessels
—Remember: Small & subcortical both start w/—tend to be subcortical
Cardioembolic
—Emboli from heart stasis or vegetations
—Remember: Emboli & everywhere both start w/E = emboli go everywhere
So now you know how different etiologies have different distributions on MRI.
Remember, catching a stroke on DWI isn’t the end of your job—it’s the beginning!
Can you get the diagnosis when it comes to carotid stenosis?
Having some confusion about the strokes you see w/ICA occlusion?
Why are there so many different patterns of infarcts w/ICA occlusion/stenosis?
There are 5 main infarct patterns—and they reflect the different types of disruption to flow you get w/carotid disease: artery to artery emboli, embolic shower, & hypoperfusion
Here’s what you see:
1. Territorial infarction w/cortical or subcortical involvement
--From artery-to-artery or distal embolism.
--More than one occlusion indicates more proximal arterial dz
2. Subcortical infarction
--When ICA, MCA, & ACA perforating deep arteries are occluded
--Can be from MCA occlusion w/good collaterals or emboli directly to deep perforating arteries
3. Combined territorial & smaller cortical and/or subcortical infarcts
--From partial embolism fragmentation or emboli shower of various sizes
4. Multiple small infarcts in the distal territories of the MCA & ACA
--If in more than one arterial territory, it’s suggestive of cardio-embolism
--If single arterial territory, it’s from a parent artery steno-occlusive lesion
5. Watershed infarctions.
Two types:
--External border-zone (located between the cortical territories of ACA, MCA, & PCA)
--Internal borderzone (between the deep & superficial networks of MCA & ACA)
--Traditionally thought from low-flow, but emboli are often a cause
--Hemodynamic mechanism may be more important in internal borderzone infarcts & embolism in external borderzone infarcts
Now you can draw the right conclusions with ICA occlusions!
Feeling stuck in the middle when it comes to middle cerebral artery infarcts?
It may be only one vessel, but you can get many different infarct patterns & symptoms depending on where it’s occluded!
Here’s what you NEED to know:
FIVE MAIN INFARCT PATTERNS
1. Occlusion of the MCA stem or proximal M1 segment before the lenticulostriate origin
--Involves deep & superficial territories
--Weakness is usually severe. Face, arm, & leg are similarly affected
--Remember: Whole MCA occlusion = Whole hemiparesis
2. Lenticulostriate artery (LSA) Infarcts
--Involves deep territory
--Hemiparesis, hemisensory, occasional aphasia & visual hallucinations
--Remember: LSA stands for Limp (weakness), Sensory deficits, & occasional Aphasia
3. Distal M1 segment occlusion after the LSA origin
--Involves whole superficial MCA territory
--Sometimes weakness in face & arm > leg (brachiofacial hemiparesis)
--Remember: Distal MCA occlusion can somewhat spare the DISTAL most extremity (leg)
4. Superior Division occlusion
--Uncommon bc superior trunk is so short
--Involves frontal & anterior parietal lobe, including pre- & post-central gyri
--Prominent faciobrachial hemiparesis w/matching hemisensory
--Rarely visual field defect
--Remember: Superior is more = more pronounced motor deficits than inferior division
5. Inferior Division occlusion
--Involves temporal gyri & superior/inferior parietal lobule
--Facial brachial weakness is more mild than w/superior division
--Common visual field defect (homonymous hemianopia or upper quadrantopia)
--Remember: Inferior is less, so motor deficits are less pronounced
--Remember: Inferior starts w/the letter “I” = “eye” so visual field deficits
Hopefully now your reports won’t middling when it comes to middle cerebral artery infarcts!
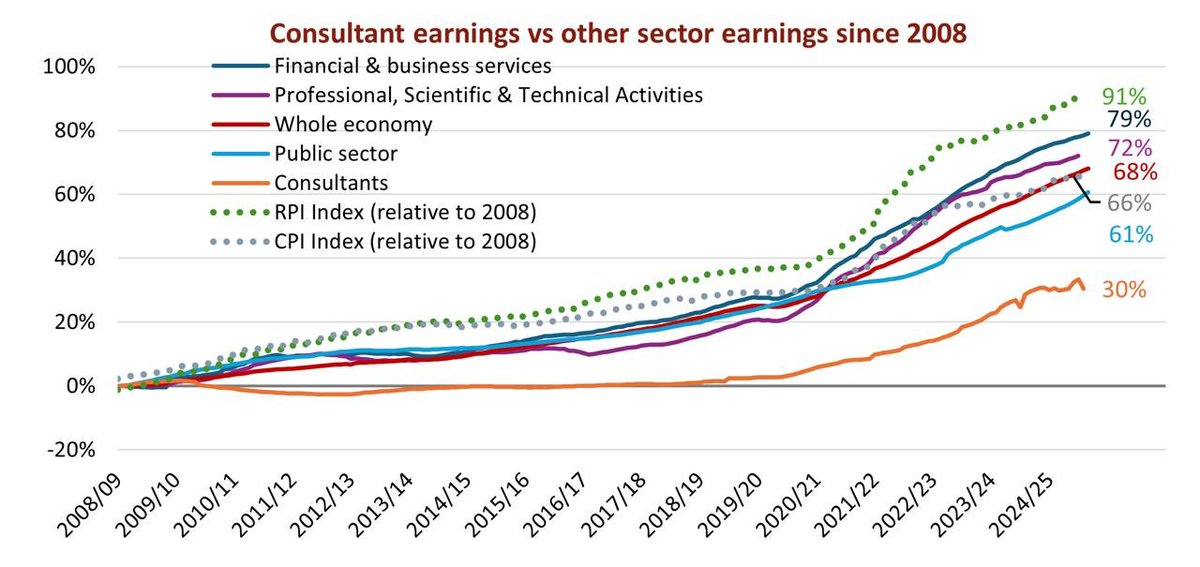
I've been trying with the BMA research team to produce one graph to rule them all. Real terms pay with inflation indexed on the same graph. Look at the CPI dotted line, our pay, the average public sector worker, worker & our comparators. It's not pretty! ONS & NHS digital
I've been a doctor since 1991. I've seen enough of my colleagues kill themselves because of the stress of this work to have zero f**ks left to give in dealing with people who abuse and malign us.
I qualified in London, worked as a medical SHO until 1995, eventually completed GP training in 1999, worked as a GP, initially locum then partner, until 2012. Then moved to Australia and became a rural generalist. I now work predominantly in the emergency, ward and HDU of a busy remote hospital, dealing with patients with the highest morbidity on the planet.
I have seen medical practice evolve. There are no 80 hour weekends for internal medicine residents anymore, but the intensity of the work has increased, the complexity has increased, the expectations have increased, the blame dumping onto juniors has increased, the general mindless bullshit has increased and the pay and conditions have got exponentially worse.
Resident doctor in a busy hospital remains one of the physically and emotionally toughest jobs in the world. People who think it's a 'job like any other job' have no f***ing idea.
Pay the residents what they are worth - which is a lot more than the BMA is asking for - and improve their conditions out of all recognition or watch them leave the profession or leave the country.
Then all you whiners will be whining your pathetic little hearts out about how there is no-one competent left to look after you. And you will deserve it.
It's your choice.
Unless someone unequivocally in last few hours/mins of life, it is very unwise for doctors ever to answer the question (under some pressure to do so) "how long?"
Be clear that person nearing end of life but avoid imprecisely guestimating n(days)
No end of trouble can result
I absolutely get the frustration many pts feel about having to repeat their 'story'.
What initiatives like this ignore is that The Story is THE cornerstone of any clinical encounter.
Before I see any pt I have formed a preliminary opinion based on the EPR
1/
Why don’t ya all in @NHSE_WTE just admit you introduced PAs to replace doctors / plug gaps and then messed up your calculations as you forgot to coordinate with @gmcuk re PLAB exams & numbers?
And now bar shutting out IMGs- you have no other way left to accommodate local graduates
Be honest
And close the door on your way out
Somehow a lot of folks have got together
And managed to create a narrative that being a doctor of medicine is elitist and one must avoid such titles
Nah.
You worked hard, you did the hard yards, you are trained beyond what others are
Feel proud to be a Doctor
Remember this- it’s a title of such value & respect that many others spend so much time trying to draw false equivalency
Imitation is the sincerest form of flattery
Be proud of that title
#sundayvibes
It's time to address the many complaints that resident doctors have about their working conditions. Access to a desk and PC to undertake administrative work, a kitchen with adequate facilities, lockers for storing personal items etc. should be standard in all NHS hospitals.
Let me predict where this is heading:
1. @wesstreeting will shut down external applications ergo IMGs applying for training posts. And the exams too.
2. There likely will be a ‘pass’ for those IMGs already in system. Maybe.
3. Non-training posts will prioritise local grads - local grads will then find out how mostly appalling these non training posts are re training & support.
An absolute sorry state- not to mention sacrifice of IMGs- most here due to rules and PLAB exam being open- with no planning being done by those who should have.
We are here due to the ineptitude and callousness of @NHSE_WTE
And the lack of any spine or foresight from organisations purporting to be “IMG- defenders” while busy being pally with central bodies for their own business
You - collectively- (allegedly) leaders across Colleges, National health bodies should hang your heads in shame- more so as you play mental gymnastics around Unqualified people trying to cos play as doctors
And hope there is a special dose of Karma reserved for you - somewhere.
And yeah- I said what I said.
For shame on you all.
It really is hard for anybody not in medicine and paying close attention, to fully understand how badly this generation of UK trainees is being treated and how profound the effects will be
Voting opens in the @RCPhysicians elections on Monday 17th March
If elected I will lead with integrity and purpose to restore the College as the #VoiceOfPhysicians - using our experience and expertise to lead on policy
This is more important than ever with the abolition of @NHSEngland and challenges that doctors' face
You can see my election statement and video here https://t.co/p98r4ETJgv
#VoteAsifQasim
#TimeForChange
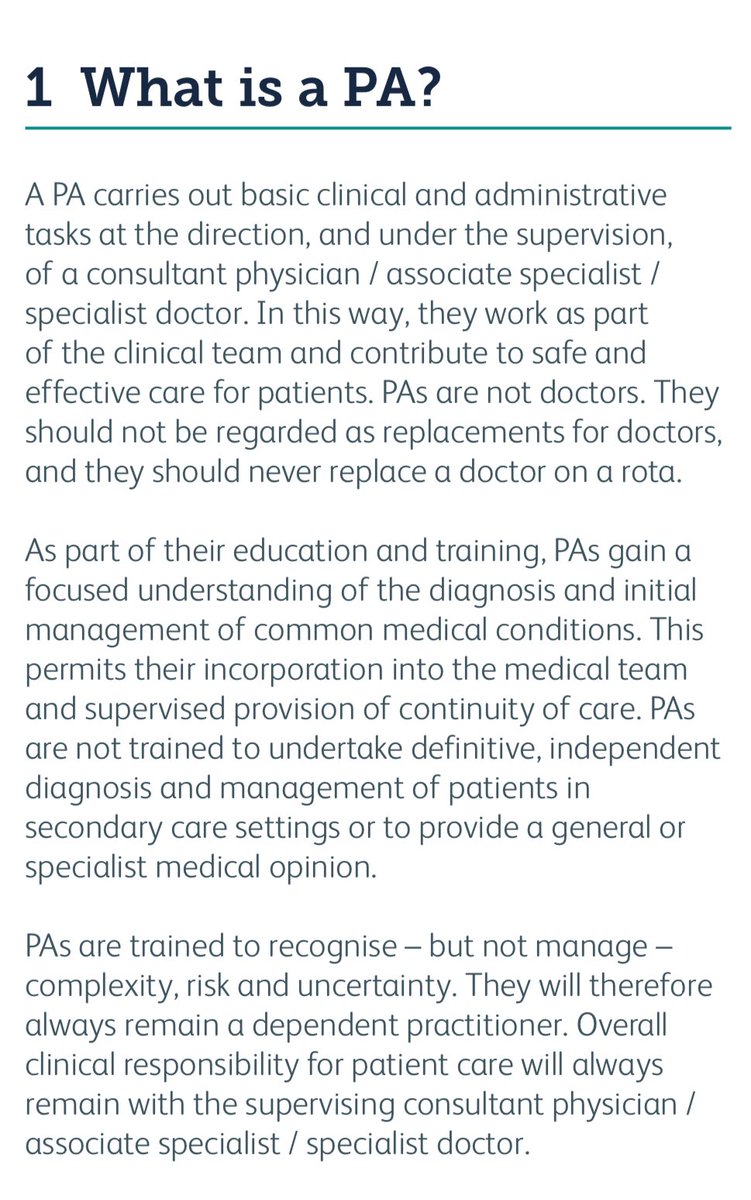
This is a much more honest and accurate description of PAs, their education, & how they can be safely part of a medical team.
Not the “generalist specialist medical model” nonsense from @NHSEmployers that obfuscated how undertrained PAs are for the roles they were deployed into.