Top Tweets for #AnesthesiaTips

🌟 Mastering Spinal Dosing: From Babies to the Elderly! 🌟
#SpinalAnesthesia #SafeSpinals
#RegionalAnesthesia #SpinalBlock
#NeuraxialAnesthesia #AnesthesiaMatters #PediatricAnesthesia #GeriatricAnesthesia #AnesthesiaTips #FellowshipLearning #TipOfTheDay #MyRATips
Tip of the Day:
A simple guide to make spinal anesthesia less confusing and more confident!
A. 🧠 How Do We Decide the Spinal Dose?
🔹The dose of spinal anesthetic isn’t “one-size-fits-all.”
🔹Customize it based on the patient’s profile, surgery site, and local anesthetic characteristics.
B.📌 Tips for Beginners
✅ Ask 2 things:
💡“What level of block do I need?”
💡“Can this patient tolerate high spinal spread?”
✅Start with the standard dose:
💡Adjust up or down based on: Height, Age, Comorbidities (like kyphosis, obesity, severe AS, scoliosis)
✅ When unsure – Use spinal opioid adjuvants to reduce LA dose but maintain analgesia.
✅ Keep a quick "SPINAL DOSING QUICK REFERENCE CARD " in your pocket.
✅ When in doubt - start conservatively, observe, and document spread.
C. 🔑 Key Factors That Influence Spinal Dose
1. 🧍♂️ Height
🔸Short (<150 cm): Slightly lower dose
🔸Tall (>180 cm): May need full dose
🔸Rationale: Taller people have a longer spinal column, so drug may spread less unless compensated.
2. ⚖️ Weight & BMI
👉Obese patients have reduced CSF volume → increased spread → use less
👉Very thin: May also need lower dose
3. 🎂 Age
🧩Elderly have less CSF + increased nerve sensitivity → use 10–20% less
🧩Young adults: standard dose
🧩Infants/children: strictly weight-based
4. 🩺 Surgery Site
📌Perineal: S2–S4 → ~1.2–1.5 mL
📌Lower limb ortho: T10–T12 → ~2.0–2.5 mL
📌LSCS/Gyn: T6–T8 → ~1.6–2.0 mL
📌Lower abdominal: T4–T6 → ~2.5–3.0 mL
5.🤰 Pregnancy
💡Less CSF, increased vascularity → reduce dose
6.📏 Baricity & Position
📍Hyperbaric: spreads with gravity (adjust table tilt)
📍Hypobaric/Isobaric: less predictable; position critical
D.👶 Pediatric (esp. <8 years):
☑️CSF volume is higher per kg than adults → requires more mL/segment
☑️General rule: 0.05–0.07 mL/kg/spinal segment (for hyperbaric bupivacaine) Or overall dose: 0.4–0.5 mg/kg
☑️Example, a 10-kg child needing T10 block (around 6–8 segments): ~0.7 mL total of 0.5% bupivacaine.
E. 👨⚕️ Adults:
➡️Not commonly taught as mL/segment because dosing is not linear.
➡️ 0.1–0.15 mL/segment can give some approximation, only in average-sized adults
➡️Example, for a T4 level (approx. 14 segments from S5): 2.0–2.5 mL of 0.5% hyperbaric bupivacaine.
➡️Remember LA spread is governed by gravity, baricity, CSF volume, and patient factors, not just volume.
F. 👵 Elderly:
👉Decreased CSF volume, increased sensitivity to LA, less compliance.
👉Need less volume/segment → 0.08–0.1 mL/segment
👉Example, in an 80-year-old, 1.2–1.4 mL may be enough for a T8 level
G.✅ Safe Geriatric Dosing (Bupivacaine 0.5% Heavy)
🦴 Hip Surgery (T10–T12 level)
🔸Dose: 1.2–1.5 mL
🔸Use adjuvants (e.g., fentanyl 15–20 mcg) to enhance effect with reduced LA volume.
🦵 Knee/Lower Limb Ortho (T10–T12 level)
🔹Dose: 1.0–1.4 mL
🔹Reduce to as low as 0.8–1.0 mL if frail or kyphotic.
📌 Tips for Geriatric Safety:
🎯Use smaller gauge needle (25G/27G pencil-point)
🎯Keep head slightly elevated to avoid high spinal
🎯Monitor for bradycardia, hypotension more closely
🎯Consider preloading + gentle vasopressor titration
🎯Maintain MAP = Age of the Patient
H.🚀🏠Take-Home Messages🎯
💉 Spinal dose is never fixed — always tailor to the patient.
👶 Pediatrics: Use 0.08–0.1 mL/kg of 0.5% bupivacaine.
🧍 Adults need 1.5–3.0 mL based on surgery level.
🧓 Elderly? Go low — 1.0 to 1.4 mL is often enough.
👩🦰 Pregnant or obese? Reduce dose by 10–20%.
🛌 Baricity and position guide your block spread.
💊 Opioid adjuvants = lower LA, longer relief.
📏 No fixed mL/segment - think clinically, not mathematically.
🧠 Ask: What level do I need? Can the patient tolerate it?
🚨 Watch for high spinal signs - and act fast.
"When it comes to spinal dosing — think smart, dose small, and aim precise!"

🔍💉 Sharpen the View: Mastering Needle Visibility in Ultrasound-Guided Blocks ✨🧠
#UltrasoundGuidedBlocks #NeedleVisibility #RegionalAnesthesia #UltrasoundTechniques #EchogenicNeedle #NeedleTracking #POCUS #UltrasoundEducation #AnesthesiaTips #MedTwitter #MedicalInfographics #BlockTechniques
#TipOfTheDay #MyRATips
Tip of the Day:
⚖️ FRCS vs PHART Framework
🔷 FRCS – Image Optimization for Diagnostics (POCUS & Scanning): Designed to maximize visualization of internal structures, ideal for initial assessment and diagnosis.
🔄Fanning: Pivoting the probe in an arc to visualize the full extent of a structure (e.g., a vessel or nerve).
🔁Rotation: Clockwise or counterclockwise turn of the probe to align anatomical landmarks with the beam.
👞Rocking (Heel-Toe Maneuver): Tilting one end of the probe to center the beam over curved surfaces like vessels.
📦Compression: Gentle downward pressure to collapse veins, remove air, and enhance contact.
➡️Sliding: Shifting the probe linearly across the skin to trace a nerve or vessel.
🧹Sweeping: Wide arc movement to explore deeper or adjacent areas.
🧠Uses: Pre-block scanning to identify structures, confirm sonoanatomy, and assess for anatomical variants.
Click this link to know it better:
https://t.co/BDOLLqHpR5
🔶 PHART – Needle Optimization for Intervention (RA & Procedures): Designed to align the needle with the ultrasound beam and improve needle tip visibility during insertion.
💪Pressure: Applying/modulating pressure to flatten tissue planes or highlight fascial layers.
👠Heeling: Lifting one end of the probe to steer the ultrasound beam and align it with the needle shaft.
🧭Alignment: Realigning the probe's center to follow the trajectory of the advancing needle.
🔄Rotation: Minor probe twists to correct obliquity or gain a clearer needle view.
🎚 Tilt: Subtle angling to enhance reflection from the needle, especially when it's not ideally echogenic.
🧠Uses: During needle insertion for peripheral nerve blocks, particularly useful in steep or oblique approaches.
🧪 TECHNIQUES to Enhance Needle Visibility
1. Needle Approach Optimization 📌
✅In-Plane Approach: Needle is aligned parallel to the probe; full shaft and tip are visible.
🚫Out-of-Plane Approach: Only a cross-section of the needle is visible; tip identification is more challenging.
⚙️Oblique Approach: A hybrid technique to improve visualization when conventional methods fail.
2. Optimize Needle Angle 📐
✅Shallow Angle (30–45°): Ideal for reflecting sound back to the probe. Better echogenicity.
⚠️Steep Angle (>60°): Ultrasound waves reflect away from the probe; needle becomes nearly invisible.
3. Hydrodissection 💧
🔷Injecting small volumes of saline/LA between tissue layers creates a visible separation and guides needle advancement.
🔷Particularly useful in fascial plane blocks (e.g., TAP, QL, ESP).
4. Tissue Movement Cues 👀
🔷Even when the needle is not directly seen, watch for tissue movement caused by needle tip advancement.
🔷Subtle lifting or shifting of layers indicates needle location and spread.
🛠️ GADGETS & Advanced TECHNOLOGIES
1. Echogenic Needles ✨
🔶Feature dimples, coatings, or laser etching that enhance ultrasound wave reflection.
🔶Essential when working at steep angles or deep planes.
2. Needle Guides 📏
🔶Clip-on accessories that maintain a fixed angle between the probe and the needle.
🔶Particularly useful for novices or in deep block placements (e.g., lumbar plexus, paravertebral).
3. Beam Steering (Electronic Focusing) 🔄
🔶Alters the ultrasound beam angle without moving the probe, enhancing needle-beam alignment.
🔶Excellent for in-plane blocks at steep angles.
4. Compound Imaging (Spatial Compounding) 🧊
🔶Uses multiple angles to generate a composite image, reducing speckle and improving clarity.
🔶Enhances visualization in noisy or artifact-prone zones.
5. Needle Tracking Systems 📡
🔶GPS-like technology using sensors in the needle or probe.
🔶Provides real-time on-screen guidance.
🔶Examples: eZono eZGuide, Philips Needle Navigation, BK Medical Smart Needle.
✅ PRACTICAL TIPS:
🕵️♂️Pre-scan first: Locate nerve, muscle, and vessels; plan the needle path before puncturing.
🔄Combine PHART & FRCS: Use FRCS for target clarity and PHART for perfecting needle visibility.
🪞Move the needle slightly: Subtle jiggling or tapping can help track needle location when visibility is poor.
⚙️Adjust depth, gain, and focus on your machine to match needle location.
✍️Use echogenic needles for deeper, angled, or fascial blocks.
🔄Don't hesitate to re-angle or re-insert if the needle is off-plane.
💡Practice on phantoms or simulators to master probe maneuvers and beam alignment.



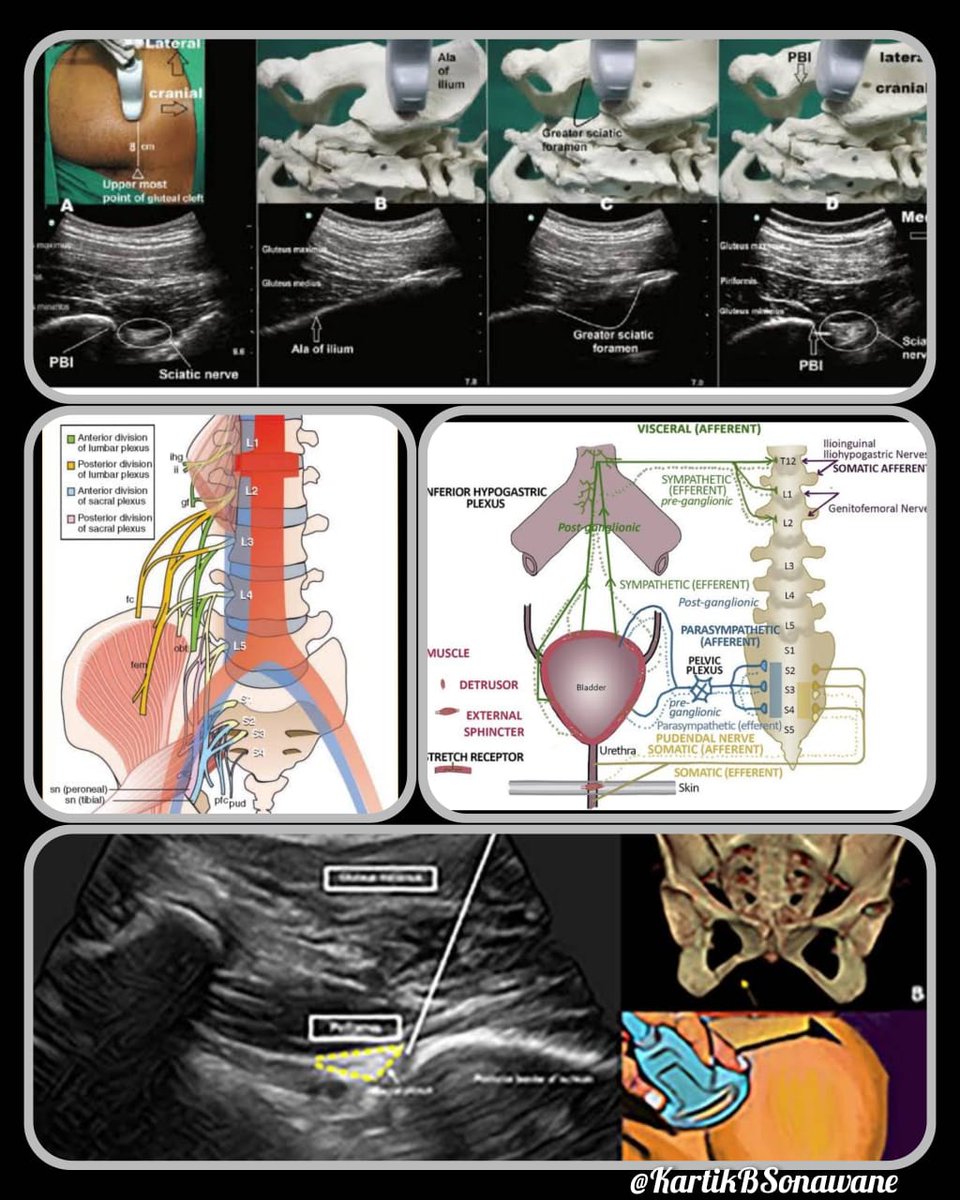
"Bladder on Hold: The Hidden Risk of Sacral Plexus Blocks"
#RegionalAnesthesia #SacralPlexusBlock #UrinaryRetention #AnesthesiaTips #NerveBlocks
#TipoftheDay
#MyRATips
Tip of the Day:
Yes—urinary retention can occur, with Sacral Plexus Block
Let's see How?
🧠 Nerve Roots Involved:
S2–S4 from the sacral plexus control bladder contraction.
⚡ Mechanism:
Blocking S2–S4 disrupts parasympathetic output, leading to:
• ↓ Detrusor contraction
• ↑ Risk of bladder atony and retention
➡️ Unilateral Block:
Lower risk—but not always risk-free.
Even a unilateral block can cross over via:
• Large LA volume
• Deep pelvic fascial spread
• Patient positioning (supine/lateral)
⚠️ Unintended Bilateral Spread:
• High LA volumes (>20 mL)
• Combined lumbar-sacral blocks
• Bilateral approaches
• Continuous techniques
• Pre-existing bladder dysfunction
♻️ Bilateral Block:
Greater chance of bladder dysfunction.
Now the risk amplifies:
• Both pelvic splanchnic supplies are inhibited
• Voiding becomes challenging or impossible
• Especially concerning in elderly or patients with LUTS
🔺 Risk Amplifiers:
High LA volume, lumbar-sciatic combo, pre-existing bladder issues.
🩺 Clinical Tip:
• Monitor post-op voiding in all sacral blocks
• Consider bladder scanning if retention suspected
• Warn patients about temporary urinary difficulties—especially with dense or bilateral effects
Bottom line:
Even "motor-sparing" regional blocks can cause autonomic side effects.
Understanding anatomy + spread = smarter, safer anesthesia.
💥 “When Serotonin Strikes: Know the Syndrome Before It Spreads!”
A deadly yet preventable drug interaction—don’t miss it!
#SerotoninSyndrome #RegionalAnesthesia #AnesthesiaTips #DrugInteractions #ICU #PharmaSafety #TipOfTheDay #MedTwitter #MyRATips
Tip of the Day:
🔬 What is Serotonin Syndrome?
A toxic storm of excessive serotonin 🔄 in the CNS—can escalate rapidly if missed.
🧠 Mechanism:
⬆️ Serotonin → overstimulation of 5-HT1A & 5-HT2A receptors → neuro, autonomic, & cognitive chaos
⚠️ High-Risk Drug Combos:
🚫 Linezolid + Tramadol
🚫 SSRI/SNRI + MAOI
🚫 Fentanyl or Methadone + Antidepressants
🚫 Lithium + SNRI
🚫 Dextromethorphan + SSRIs
🚨 Symptoms to Catch Early:
🌀 Agitation, confusion
🔥 Hyperthermia, hypertension, tachycardia
🤯 Tremor, clonus, hyperreflexia (esp. in lower limbs)
😓 Sweating, restlessness
🕐 Rapid onset (within hours), fast progression
👁️ Lower limb clonus = a red flag!
🧴 Management Pearls:
🛑 Stop all serotonergic drugs
💤 Sedate with benzodiazepines
🧊 Cooling for hyperthermia
💊 Cyproheptadine = serotonin antidote
🏥 ICU care if severe
💉 Regional Anesthesia (RA) Advantage 🚀
✅ Opioid-sparing: Reduces risk in serotonergic patients
✅ Avoids systemic sedatives
⚠️ But beware:
Intra-op use of Linezolid + Tramadol is risky—even in RA cases
Post-op agitation or tremor ≠ shivering → think serotonin!
Use non-serotonergic multimodal analgesia: Paracetamol, NSAIDs, ketamine (low dose)
🔍 Bottom Line:
🧠 Think serotonin syndrome in confused, twitchy, sweaty post-op patients
💊 Always review med history before giving linezolid or tramadol
💉 Use RA wisely—it could be life-saving


"Don’t Be Fooled: Why ESP Block Isn’t a Spine Surgery Soloist"
#ESPBlock #AnesthesiaTips #SpineSurgery #RegionalAnesthesia #PainManagement #PatientSafety #MinimallyInvasive
#MyRATips
Tip of the day
The Erector Spinae Plane (ESP) Block may look like a magic trick—but here's why it's not your one-stop solution for spine surgeries:
🎯 Targets dorsal rami only consistently – covers skin & deep muscles
🚫 Misses anterior rami – which supply superficial/intermediate muscles & thoracolumbar fascia
⚠️ Medial branch spread? – too unpredictable to trust
🔥 Fascial pain generators – often go untouched
🔒 Airway security in prone – GA is a must for patient safety, isn't it?
So, when does ESPB shine?
✅ Great for minimally invasive procedures (e.g., vertebroplasty, endoscopic discectomy)
❌ Not enough for open or major spine surgeries
Use ESPB smartly—but don’t fly solo when the stakes are high!




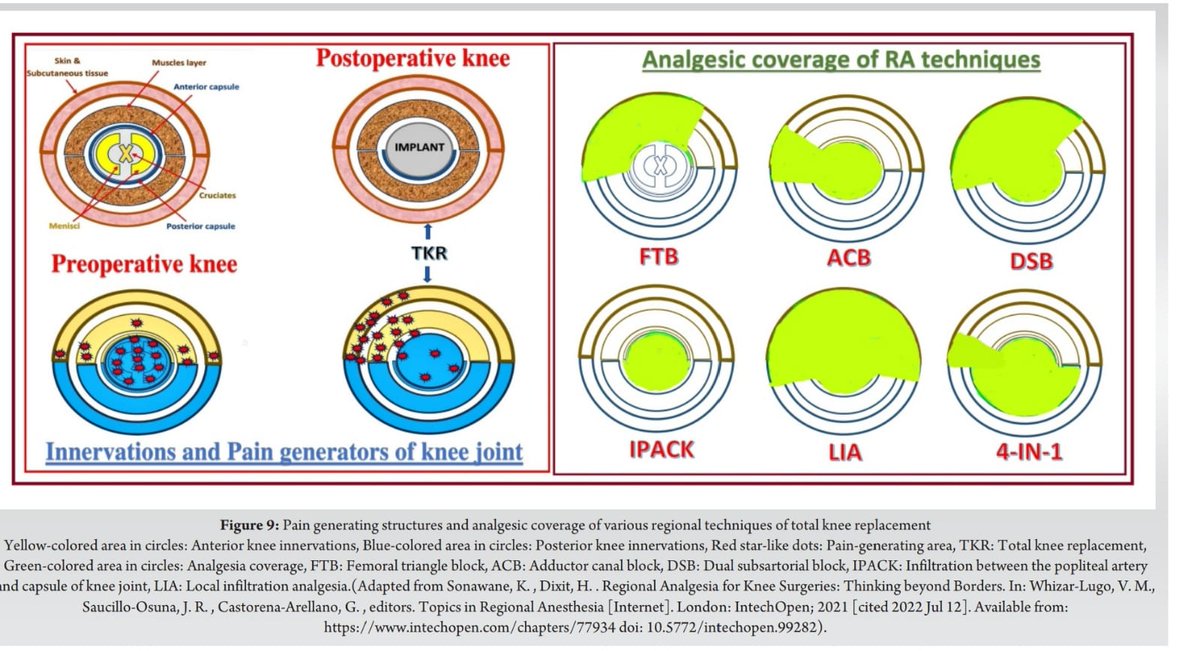
"Shifting the Pain Paradigm in TKA"
#TKAInsights #PainPathways #RegionalAnesthesia #PostoperativePain #KneeSurgery #GenicularBlock #ExtraArticularPain #PeriarticularTargets #SmartAnalgesia #OrthoAnesthesia #AnesthesiaTips #PainManagement #PrehabToRehab
Tip of the Day:
Before TKA,
The Pain source is primarily intra-articular—originating from structures inside the knee joint such as cartilage degeneration, inflamed synovium, and subchondral bone changes.
This makes targeting intra-articular and capsular innervations, especially the genicular nerves, a logical approach for preoperative pain management and delaying surgery.
However,
After TKA,
the native joint is removed and replaced with prosthetic components. Now, the pain no longer comes from inside the joint. Instead, it becomes an iatrogenic, extra-articular issue—arising from surgical trauma to soft tissues, the joint capsule, periosteum, quadriceps tendon, and skin. These are structures that lie outside the replaced joint.
Bottom line:
Patients don't feel pain in the joint post-TKA—it’s the pain around it that matters!
Tailor your analgesia accordingly.
Watch this video to understand it better,
https://t.co/p2Wnpv4W3H
Tip of the Day
"Where It Starts, It Spreads: Chest Wall Blocks Decoded"
#RegionalAnesthesia
#ChestWallBlocks
#UltrasoundGuidedBlocks
#AnatomyMatters
#BlockSpread
#PecsBlock
#SAPBlock
#PainManagement
#AnesthesiaTips
Always know the origin and insertion of the muscle where local anesthetic (LA) is deposited during chest wall blocks.
The anatomical extent of that muscle largely determines the dermatomal coverage of the block.
For example:
Pectoralis Major extends only to the 6th rib, typically providing coverage from T2 to T6.
Serratus Anterior originates as far as the 9th rib, allowing the SAP block to cover T3 to T9.
Understanding muscle anatomy is key to predicting block spread and optimizing analgesia.
By Dr. Kartik Sonawane


🚨 New Video Alert! 🚨
🎤Just released a new video on YouTube Channel “Block Onn!”
✍️ sharing some key insights from #ESRA2024 Regional Anaesthesia Workshops 🙌
🎥 Watch it here:
👉 https://t.co/TuJg223bf8
#RegionalAnaesthesia #UltrasoundGuided #AnesthesiaTips #MedEd #PainManagement #NerveBlocks #AnesthesiaEducation #AnesthesiaCare #HealthcareProfessionals #BlockOnn #MedicalYouTube
@MadanNarayanan @EMARIANOMD @SerkanTulgarMD @Ropivacaine @drnavyaravi @NavBahal @ashwani_doc @DG_KDASGUPTA @docmorne @beckimarshRA @rosie_hogg @chandra_ri64999 @tsmurali @DrRakeshGarg8 @RAPMOnline @AoraIndia @aosra_pm @claralexlobo @Steve_Coppens @KalagaraHari @loinabhi




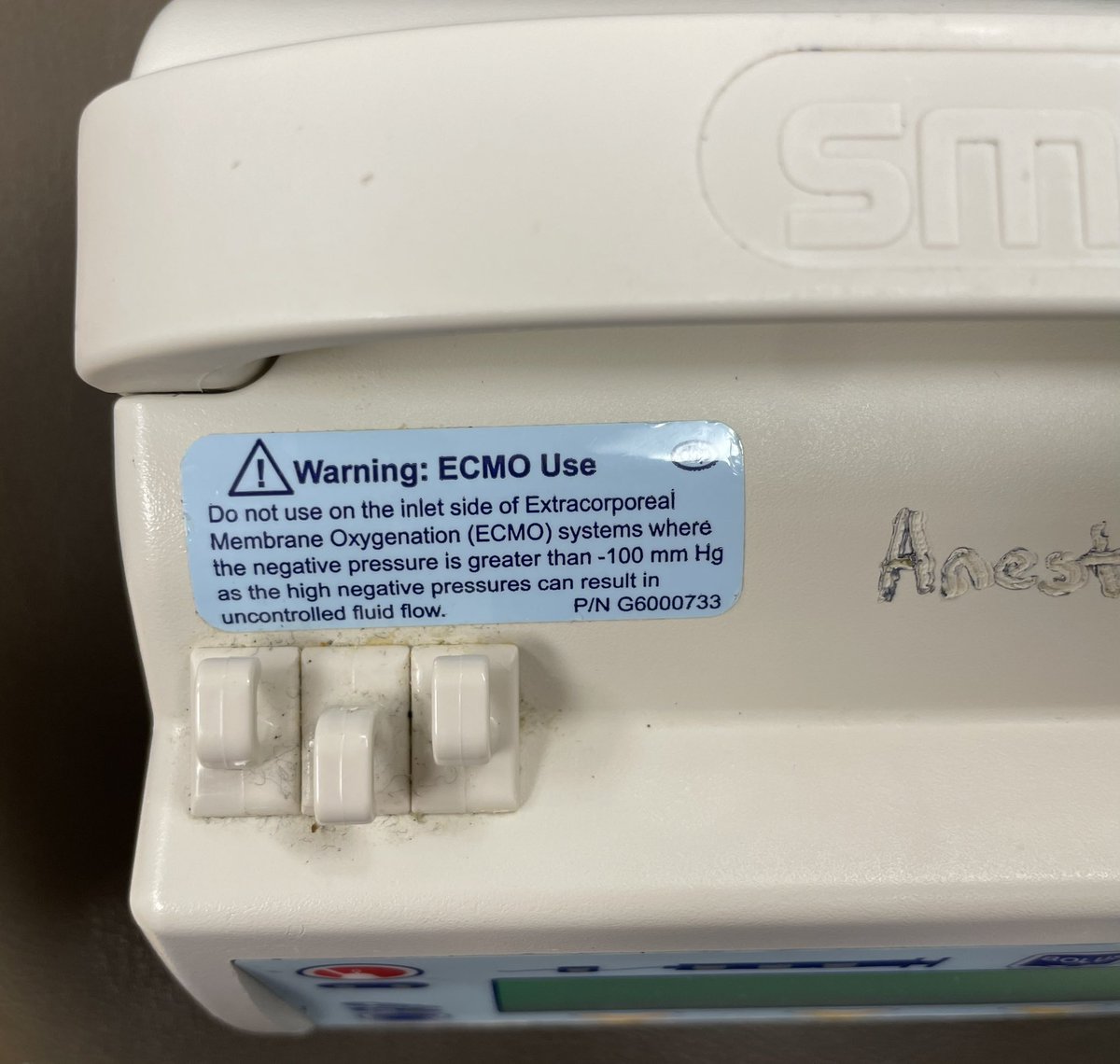
Do not use syrine-pumps on the inlet (drainage) side of Extracorporeal Membrane Oxygenation (#ECMO) systems where the negative pressure is greater than -100 mm Hg as high negative pressures can result in uncontrolled fluid flow. #anesthesiatips #criticalcare

#AnesthesiaTips: side effect of #GeneralAnesthesia is nausea/vomiting aka #PONV (post-op nausea vomiting).
Greatest risk:
🔹young females
🔹non-smokers
🔹procedures: Gyn, ENT, Urology
🔹motion sick
Help:
🔹#TIVA (total IV anesthesia), avoid gas
🔹#NerveBlock
🔹#ScopePatchZofran

Trends for you
Most Popular Users

Elon Musk 
@elonmusk
240.7M followers

Barack Obama
@barackobama
119.2M followers

Donald J. Trump
@realdonaldtrump
111.7M followers

Cristiano Ronaldo
@cristiano
110.8M followers

Narendra Modi
@narendramodi
107M followers

Rihanna
@rihanna
97.7M followers

NASA
@nasa
92.2M followers

Justin Bieber
@justinbieber
90.9M followers

KATY PERRY
@katyperry
87.8M followers

Taylor Swift
@taylorswift13
81.6M followers

Lady Gaga
@ladygaga
73.1M followers

Virat Kohli
@imvkohli
70M followers

Kim Kardashian
@kimkardashian
69.8M followers

YouTube
@youtube
68.7M followers

Bill Gates
@billgates
63.9M followers

Neymar Jr
@neymarjr
62.8M followers

The Ellen Show
@theellenshow
62.4M followers

CNN
@cnn
61.9M followers

Selena Gomez
@selenagomez
60.8M followers

X
@x
60.8M followers