Top Tweets for #MarkoAASGuide

MAAS-11.2
#MarkoAASGuide
#CycleFromStartToFinish #TRTPrep #PEDLongevity
Testosterone: Part 2 - from glands → lab synthesis → medicine cabinet
Before we had injectable esters, bro forums, and “TRT clinics” next to the vape shop… testosterone was a legit scientific conquest.
And the story is actually wild.
1) Humans knew “testes do something” long before they knew testosterone existed
For basically all of recorded history, people observed that removing testes changed behavior, strength, secondary sexual traits, fertility, etc. That knowledge got used in… let’s call it “ethically questionable ways,” including castration for social control and other grim reasons.
Modern science eventually tried to turn that crude observation into medicine. Early “organotherapy” was basically: “What if we… used testes… as therapy?”
Spoiler: mostly placebo-level nonsense.
The real breakthrough required isolation and chemistry.
2) 1935: isolation + naming (the “we finally caught the hormone” moment)
In May 1935, a group at Organon published work describing the “isolation of crystalline male hormone from testes” and named it testosterone — built from “testicle” + “sterol” + “ketone.”
That’s a real “put it in a jar and prove it exists” milestone.
3) 1935: first lab synthesis (the “we can now make it” moment)
Also in 1935, testosterone’s structure was clarified and then the molecule was chemically synthesized from cholesterol — reported by Butenandt and Hanisch, shortly followed by another synthesis report from Ruzicka and Wettstein.
This matters because it’s the difference between:
“We found a rare thing in biology,” and
“We can manufacture a reliable supply for medicine.”
4) 1939: Nobel Prize energy enters the chat
The Nobel Prize in Chemistry in 1939 was split between Adolf Butenandt (“for his work on sex hormones”) and Leopold Ruzicka (for his work on polymethylenes and higher terpenes).
And yeah — this is why I’m befuddled when people think “steroids” are some brand-new dark art cooked up in a gym bathroom. The science is old, elite, and foundational.
5) Why testosterone became a medical tool (and not just a chemistry flex)
Once testosterone existed as a reliable pharmaceutical, medicine had a hammer… and suddenly a lot of conditions looked like nails.
Clinically, testosterone has been used for:
*Hypogonadism and related conditions (i.e., true low testosterone states)
*Delayed puberty in certain contexts
*Historically/regionally: some breast cancer cases and other indications depending on era and guidelines
*And broader “anabolic” therapeutic contexts have included things like wasting syndromes, severe burns, certain injuries, anemia, etc.
6) The delivery problem: why early testosterone needed formulation innovation
Here’s the key pharmacology headache: oral testosterone gets heavily inactivated by the liver, which pushed medicine toward parenteral administration (injections) or modifying the molecule and formulation to make it clinically useful.
That one fact is basically the mother of a whole pharma family tree:
*injectable forms that last longer
*transdermals
*modified oral approaches
*and a long list of testosterone-derived AAS that tried to separate “anabolic” from “androgenic” (never perfectly achieved)
Uncle Marko takeaway
Testosterone’s medical story is not “gym lore.” It’s a 1930s scientific breakthrough (isolation + synthesis), followed by decades of real clinical utility — and then later the molecule got dragged into sports controversy and cultural panic.
Next post: the part everyone reads first anyway —testosterone as a PED in sports and recreational use, and why anti-doping science had to get clever because… you literally make testosterone in your own body.
MAAS-11.1
#MarkoAASGuide
#CycleFromStartToFinish #TRTPrep #PEDLongevity
Testosterone: The OG, naturally occurring AAS (the “base plate”) – PART 1
Ok… you wanted it, so here we go. I warned you the Testosterone posts take multiple parts — because this molecule is basically the foundation of the whole AAS universe. It's the GOAT.
Also: I’m NOT a scientist or a medical professional. I’m the guy trying to translate biology into something your AAS Goblin brain can actually use, with risk reduction being the whole intent.
Now… let’s talk about the fundamental naturally occurring anabolic-androgenic steroid in the human body: TESTOSTERONE.
1) Testosterone isn’t “a male hormone.” It’s a human hormone.
Yes, testosterone is the headline hormone for male physiology — but it exists in both males and females, and it matters in both.
Here’s the part that melts people’s brains: in females, testosterone is the most abundant circulating active sex steroid across the lifespan. And it can be 5–50x more abundant than estradiol depending on life stage.
So, if someone says “women don’t have testosterone,” they’re telling you they learned endocrinology from a comment section.
“But chicks ain’t got no nads!” you say: Women DO produce testosterone, primarily from two sources:
The ovaries (which produce a significant portion, often around 25–50% of circulating testosterone, depending on the source and measurement method).
The adrenal glands (which contribute directly in small amounts but also produce precursors like DHEA and androstenedione that are converted to testosterone in peripheral tissues).
2) What is testosterone, chemically?
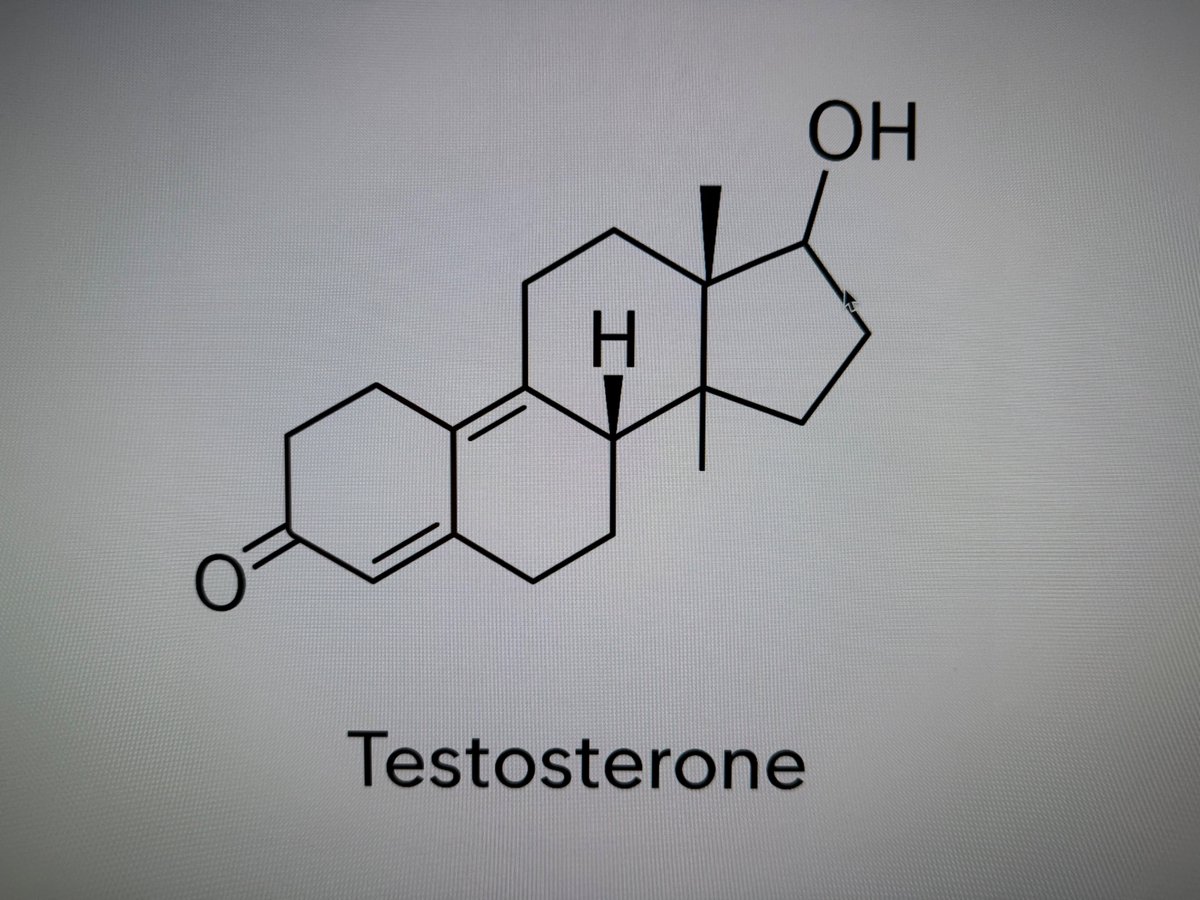
Testosterone is a C19 steroid (androgen) built on the classic steroid backbone — those famous four carbon rings.
In chemistry terms, androgens are built on an androstane skeleton and testosterone is the primary natural androgen (with the typical Δ4-3-keto and 17β-hydroxyl features).
If you want the “label on the bottle” version: testosterone’s chemical formula is C₁₉H₂₈O₂, and you’ll see it referred to as 17β-hydroxy-4-androsten-3-one.
3) Testosterone is the base structure for basically every AAS you’ve heard of.
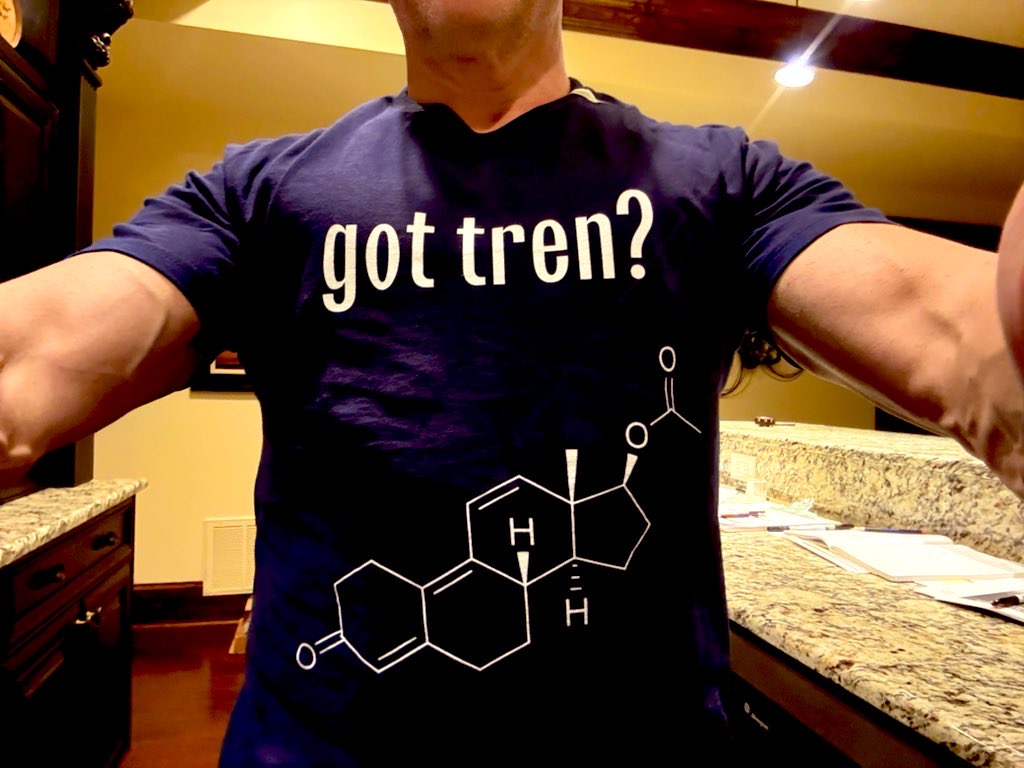
This is the “epiphany” moment: look at testosterone… then look at tren, dbol, primo, mast… and realize they’re all the same steroid Lego set, just with different pieces clipped on.
EVERY AAS is a derivative of the human testosterone molecule.
That doesn’t mean “they’re all the same.” It means the core skeleton is the same, and the “feel” (and risk profile) changes because chemists tweak how the molecule behaves: receptor binding, aromatization, reduction to DHT-like effects, metabolism speed, etc.
4) Testosterone is both a hormone AND a “parent molecule”
In males, testosterone is produced by Leydig cells in the testes. It binds the androgen receptor (AR) like a proper hormone… but it also acts like a parent compound that can be converted into other powerful hormones in tissues.
Two famous conversions:
Testosterone → DHT (via 5α-reductase): a “pure AR” androgen vibe
Testosterone → Estradiol (E2) (via aromatase): not “the enemy,” but a real physiological player
Translation: testosterone isn’t just “the king.” It’s also the fork in the road to other major biological effects.
5) Why we call it an AAS (even when it’s natural)
“AAS” is short for Anabolic-Androgenic Steroid.
Anabolic = supports muscle protein building (and recovery, and tissue adaptation)
Androgenic = supports “male-pattern” traits (voice, hair, libido, etc.)
Testosterone is highly anabolic and androgenic in the real world.
But don’t get it twisted: testosterone isn’t a magic spell that overrides bio-chemistry. If your training is trash and your diet is Doritos + Vapes, your “anabolism” is going to build… nothing.
Uncle Marko takeaway:
Testosterone is the most important naturally occurring AAS in the human body, present in both sexes, and it’s the molecular base plate that the entire synthetic AAS world is built on.
Next post we go into: How humans first isolated it, synthesized it, and why a Nobel Prize got dropped into the chat.
MAAS-10
#MarkoAASGuide
#CycleFromStartToFinish #TRTPrep #PEDLongevity
You don’t run a cycle: You build one. You measure one. You survive one.
Everyone wants to talk Tren, Halo, or the “secret Russian blend.” Ask @KING_DOC_ or @Ironhands57...lol
But your first real discovery is this:
👉 how much testosterone your body can handle without blowing your lipids, your sleep, or your life apart, and get good results in the gym.
1️⃣ Pre-Cycle — The Setup
If you skip this, you’re not cycling… you’re gambling.
Full labs (CMP, CBC, Lipids, Hormones, Iron, Thyroid — see MAAS-4)
Baseline DEXA, BP, HRV, and weight
Sleep fixed, diet dialed, training plan written
Support stack purchased before first pin (TUDCA, NAC, fish oil, citrus bergamot, telmisartan, nebivolol, etc.)
Cycle tracking sheet printed and ready
The setup is the most underrated phase. You either start controlled or start chaos.
Be ready to break up your weekly dose into 2 or 3 microdoses. So 300mgs per week can easily become 3 100mg shots. Get used to it. It’s just a better approach, but it increases the chances of PIP and abscesses because you’ll be 2 or 3 shots into contaminated gear before you notice pain and swelling (is your LAB setup optimized?)
2️⃣ The First Cycle — Test-Only Discovery (Weeks 1–12)
Your goal isn’t to become Mr. Olympia — it’s to learn your personal tolerance ceiling.
Start with testosterone enanthate or cypionate.
That’s it.
No Deca. No Tren. No Dbol. No “super blend.”
Start modest — 250 mg/week, ramp slowly (from 125mgs in 50–100 mg steps) if labs and sides stay clean.
You’ll discover:
How fast you aromatize (E2 swings)
How your BP, HDL, and sleep react
How your mood and libido shift
How much acne or bloat or hair loss
How much oil your delts or glutes can take
Run an AI only if high E2 symptoms or bloods require it — not preemptively.
STAY PURE TEST - add no other PED.
The first cycle isn’t about size.
It’s about signal: learning your body’s feedback loop.
3️⃣ Blasting & Cruising — The Long Game
Once you’ve mapped your tolerance, you’ll face the next philosophical question:
Do you come off… or cruise?
Cruising means holding at a TRT dose (150–200 mg/week) year-round, staying hormonally stable and using short “blasts” (higher-dose phases) for growth.
Blasting means strategic surges — 12–20 weeks of elevated Test and/or a companion compound.
Think of it as performance season followed by maintenance season.
The secret isn’t in the blast. It’s in the discipline of the cruise.
Cruising is where your heart, blood, and brain recover so you can keep doing this for decades — not just one summer.
4️⃣ The Build Phase (After You Know Your Ceiling)
Now you can design a proper blast:
Test stays at your sweet spot (for some guys – that’s 300mgs, for others it’s 750mgs – YOU do YOU and don’t chase what some other genetic freak can tolerate)
Add one additional compound with purpose (Primo, Mast, or Deca — pick your lane - and I will do a writeup on all of these and more in upcoming MAAS posts)
Progressive overload training, 0 RIR sets, cardio intact
Bloods every 6–8 weeks
Track sides ruthlessly
Data replaces ego here.
5️⃣ Cruise / Reset (6–8 Weeks)
Come back down to TRT.
Stay on your health stack.
Let your labs normalize before you chase another blast.
Hematocrit, lipids, and E2 will thank you.
6️⃣ Exit & Reflection
Compare pre- vs post-cycle labs, DEXA, and notes.
Ask:
What dose felt best?
What sides appeared and when?
Was the trade-off worth it?
If you can’t answer those — you weren’t tracking enough. Go back and read all my MAAS post to learn how to track.
Marko’s Commandments
First cycle = Test-only. Everything else is noise until you know your baseline response.
Add one variable at a time. You can’t debug chaos.
Bloods every 6–8 weeks.
Sleep & BP > pumps & PRs.
Over time, Cruise longer than you Blast. Longevity > novelty.
Poll:
What was your biggest surprise on your first Test-only run?
1️⃣ How much better I felt overall
2️⃣ How fast sides showed up
3️⃣ How much my bloods changed
4️⃣ How little I actually needed



MAAS-9
#MarkoAASGuide
#LabSetup #CyclePrep #TRTReady
Before the first pin ever hits skin, you need your lab dialed in.
No, not a Breaking Bad trailer or whatever lab my friend @PGC1a_RB is cooking Pho in....
I’m talking about the home chemist’s drawer — the toolkit that keeps your cycle sterile, accurate, and trackable.
If you’re going to inject hormones you bought on the internet, at least look like you’ve got your shit together - as my buddy @Ironhands57 does.
1️⃣ Injection Hardware
Syringes:
1 mL or 3 mL Luer-Lock only (no slip-tips, no Amazon mystery packs)
Designate each for single use; you are not a street junkie - never reuse, ever.
Buy 100 at a time and be ready to reorder – they go faster than you think.
Needles:
Drawing: 18-20 g, 1 inch
Injecting: 25-27 g, 1–1.5 inch (glutes = 1-1.5", delts/quads = 1") – I use a 1” for everything IM. Sometimes use a ½” for delt shots of peptides or HGH (when out of SLINs)
Rotate sites religiously — glute → quad → delt → ventroglute. (watch YouTube videos in IM injection sites)
I find I can push oil through a 27g easily from a 1mL syringe, but I need a 23g/25g to push oil from a 3mL syringe without my thumb cramping up.
Again – buy 100 or more at a time – you’ll find an empty box soon enough.
NEVER inject with the needle you draw with – aways use a new injection needle (unless you’re using a fixed needle SLIN (not ideal))
Alcohol Swabs & Cotton
If you run out, your cycle is over until you restock. Period. NEVER REUSE ANYTHING.
2️⃣ The Clean Zone
70% isopropyl wipes or spray
Nitrile gloves (oil is bacteria food)
Paper towels > cloth rags
Lighted magnifier if you’re mixing peptides or filtering oil
Think of this like food prep — would you eat off that surface? Then don’t pin from it.
3️⃣ The “Chemist” Tools
Filters: 0.22 μm sterile syringe filters for re-filtering UGL oils.
Crimp tops / sterile vials: transfer & store your own mixes safely.
Bacteriostatic water: for peptides or HCG reconstitution.
Insulin syringes “SLINs” (29–31 g): for subQ or peptide shots.
Mixing Beaker / Hotplate: optional, for advanced users brewing carrier oil blends (if you don’t know, don’t).
🧫 SIDEBAR: Re-Sterilizing Used Vials — Marko’s “Don’t-Die” Method
You’re out of empties.
You’ve got filtered oil ready.
And that old vial is winking at you.
Short answer — yes, you can reuse it… if you do it right.
1️⃣ Strip it down
Toss old stopper + crimp.
Wash glass with hot water + soap and soak 20 minutes.
Rinse with distilled H₂O → final rinse 99 % isopropyl.
2️⃣ Bake the glass
180 °C (356 °F) × 60–90 min.
Cool in the closed oven = no dust seasoning.
3️⃣ Prep new closures
New sterile rubber + caps preferred.
If reusing (not recommended): soak 20 min in 70 % iso, then boil 30 min.
4️⃣ Assemble clean
Gloves on, wipe bench, transfer baked vial, insert stopper, crimp, wipe again.
5️⃣ Fill through a 0.22 µm filter
Hydrophobic (PTFE/PES) for oil, hydrophilic for water.
Filter directly into the vial, cap, label, store cool and dark.
Reality check
✅ Filters out bacteria and spores.
❌ Does not remove endotoxins or viruses – you may still react.
❌ If it still looks cloudy or smells off — toss it.
Sterility > Strength.
Every infection you prevent is worth more than another 3000 mgs of gear.
And remember this – your gear is most likely contaminated by YOU. It's you’re poor handling practices that are likely to contaminate that hard to get Primo, so be obsessive about cleanliness.
🧫 End SIDEBAR
4️⃣ The Tracking Arsenal:
Digital kitchen scale (0.01 g precision for oral powders)
Mini-notebook or spreadsheet: every pin, compound, and lot # logged
Label maker or tape & Sharpie: date, concentration, expiration
Weekly printout sheet (see MAAS-7 tracking setup)
If it’s not written down, it didn’t happen — and when your bloodwork spikes, you’ll have no clue why.
5️⃣ Storage & Disposal:
Temperature: Keep oils 68-75 °F. Avoid freezing or direct sun.
Light: Amber vials for a reason. UV kills potency.
Sharps container: $5 at CVS. Don’t be the idiot tossing pins in the trash.
Mini-fridge: For peptides, HCG, insulin. Label EVERYTHING.
Mini-safe: Got kids? The gear goes in a safe box with a combination lock, or your 12 year-old is going to quickly appear to be abnormally hairy and jacked.
6️⃣ Emergency & Safety Kit:
Antibacterial ointment + band-aids
10 mL sterile saline (for flushing accidental abscess area)
Thermometer & BP cuff
Antibiotic on standby (doctor-prescribed only — don’t self-dose blindly)
If you’re going to play chemist, you better play nurse too.
7️⃣ The “Luxury” Upgrades:
Vial warmer (faster draws, smoother IM pins)
NeedleGuide auto injector for that fast and accurate jab
Vortex mixer for peptide blends
Vial Crimper hand crimping tool
Mini-ultrasonic cleaner (for glassware)
Dedicated toolbox or tackle box for everything above
Autoclave - but you can use a pressure cooker too
Organization is underrated masculinity.
Marko’s Rules of the Lab:
Sterility beats strength — every single time.
Never reuse anything that pierced skin.
Label like a psychopath.
Treat your body like the test subject it is — with respect.
If it smells off, it is off. Toss it.
Poll:
What’s the dirtiest thing you’ve seen someone do on cycle?
1️⃣ Reuse a needle
2️⃣ Skip swabbing
3️⃣ Store vials in a gym bag
4️⃣ “Dry pinned” straight from a bottle cap




MAAS-8
#MarkoAASGuide #TRTPrep #PEDLongevity
CYCLES — TRT, HRT, BLASTING, CRUISING, & WHEN TO BAIL 🚨
Most people know how to start a cycle.
Almost nobody knows how to end one without wrecking their health.
Let’s fix that 👇
But first – I don’t want to get into the “cycle” definition controversy. My definition of a cycle is when you’re going from natty or TRT, to some dosing of AAS that’s greater than the top end of TRT (like >200mgs/wk) to achieve a physiological objective, and then back to TRT or natty for a period of time.
There are four main ways to live the enhanced life — and only one of them is permanent.
1️⃣ TRT — Testosterone Replacement Therapy
Goal: bring hormones back to normal range.
100–200 mg/wk. Supervised. Sustainable.
You’re not chasing size — you’re chasing stability.
But half the guys calling it “TRT” are pinning 400 mg and lying to themselves.
2️⃣ HRT — Hormone Optimization
The “wellness” cousin of TRT.
Maybe GH, DHEA, peptides, micro-dosed anabolics.
Marketed as anti-aging, but you’re basically running a forever-mini-blast.
Treat it like medicine: labs, BP, liver.
3️⃣ Blast & Cruise — The Lifestyle
The honest long game.
You stay on year-round — you just change altitude.
Blast: 12–16 wks higher dose (Test + one anabolic – you are NOT COMPETING so keep it simple, silly)
Cruise: 20–24 wks at TRT dose (150–200 mg/wk)
If your “cruise” is 500 mg, that’s not cruising — that’s denial.
The secret isn’t the blast. It’s the discipline of the cruise.
Cruise longer than you blast, or you’ll be cruising straight into a cardiac MRI.
4️⃣ Cycle + PCT — The On/Off Classic
8–16 wks on a blast, 4–6 wks PCT.
Clomid + Nolva (+ HCG if you’re smart).
Works for younger users with intact HPG axis.
Older guys? You’ll probably end up on TRT anyway.
Bloods at 4 & 8 wks post-PCT to prove recovery.
Bailing on a Cycle — When & How:
Things go wrong. Awareness > ego.
Pull the plug if:
* BP > 150/95 for a week
* You develop multiple injection site reactions/abscesses – your gear is dirty or you're reacting to harsh ingredient!
* Resting HR ↑ 15 bpm
* Chest pain, dark urine, insomnia, panic
Blood work is not right (not a complete list):
* ALT/AST > 3× baseline
* Hematocrit > 54 and you can’t donate
* LDL is through the roof, HDL is crashed
* Kidney function is suffering – eGFR dropping,
* Cystatin-C above range
How:
1️⃣ Drop orals first
2️⃣ Reduce to TRT dose 4–6 wks (new vial if multi-PIP driven)
3️⃣ Load support stack (NAC, TUDCA, Citrus Bergamot)
4️⃣ Hydrate + sleep
5️⃣ Retest labs 3–4 wks later
Quitting early doesn’t make you soft — it keeps you alive to lift again.
6️⃣ PCT — Restart Mode
(Example: Test E cycle)
Wks 1-2: Wait for esters to clear
Wks 3-6: Clomid 50 mg ED + Nolva 20 mg ED
Wk 7+: Labs → Test, LH, FSH, E2
If still tanked → stop pretending. Go see a doctor (like @CoffeeBlackMD) or a great consultant (like @BowTiedHRT) who knows and understands this process, consider TRT and focus on longevity.
Marko’s Cycle Rules
Don’t start what you can’t finish.
Always have your cruise or PCT ready before the first pin.
Never chase sides — mitigate them.
Bloods > Bros.
Health > Hype.
UNDERSTAND: YOUR BALLS MAY PERMANENTLY SHUT DOWN - DO NOT START THIS IF THAT'S AN ISSUE FOR YOU. Uncle Marko is 62, has all the kids he'll ever have, and a vasectomy - I don't give a shit of my HPTA is fractured.
In the end - you'll do what you do. Some guys just white-knuckle through sides hoping they'll settle down (and some actually do get better). But these posts are about risk mitigation for older lifters who may not have much health reserve left. It's one thing when you're 30. It's a whole different ballgame at 60.
Poll:
Which camp are you in right now?
1️⃣ TRT for life
2️⃣ HRT optimization
3️⃣ Blast & Cruise
4️⃣ Still pretending I’ll PCT and “recover naturally”



MAAS-7
#MarkoAASGuide #TRTPrep #PEDLongevity
How I Track a Cycle (Responsibly):
If you don’t track your cycle details on a daily basis, here’s what’s going to happen:
You’ll lose track of when you started.
You’ll forget when compounds were added or dropped.
You won’t know which week your bloodwork lined up with.
You’ll almost always pin more than you think.
You won’t be able to pinpoint the cause of side effects.
Was very happy to see that @nateyamasaki, @RaelHelman , @liftfromspiral, @doubleJ200 , @notsleepy , @chrisbgolfer , @LloydChiro , @cjtrapp , @ranchertexan99 , @reallyoptimized , @SevLaxRules , and @TxSecurityGal , to name a few, are all avid data trackers, all using different but equally effective methods. Please sound off in the replies and provide your approach so people can learn. Using AI or a ready made app is brilliant!
DAILY:
I keep a 7-day sheet listing every compound on hand — AAS, peptides, aminos, orals, oils, everything.
I print one for each week.
If I add a compound, I re-print the pack and toss the old one.
Each sheet lists the calendar date and cycle day (Oct 6 = Cycle Day 117).
Every time I pin or swallow something, I write down the exact mL or tabs used that day — right off the syringe.
Once per week, I total those numbers on a separate weekly sheet.
This keeps me honest. No “I think that was 0.7 mL.” I measure. I write. I verify.
You’ll miss days, get sick, hit bad sites, or lose track.
This system keeps chaos from taking over.
WEEKLY:
I build a weekly table with compounds down the side and each week as a column header.
I total up the mLs and the sheet auto-converts to mgs per week.
I always keep Testosterone separated — it’s my anchor compound and I want its trend visible.
On this same sheet I log bloodwork dates so I can line up any anomalies to what compounds were active, added, or pulled that week.
METRICS:
Every week I record:
Morning weight (same Withings scale, same time)
Waist size
Resting HR & BP (BP creep is real)
Sleep quality (WHOOP, Garmin, or 1–10 rating)
Training performance (top sets or total volume)
Injection site reactions / mood notes
Those six datapoints + your AAS log = 80% of what’s really happening inside you.
RED FLAGS:
If I see BP > 145/90, resting HR > 80, hematocrit > 53%, or ALT/AST > 2× baseline, I mark it in red.
That’s my cue to pull labs early, donate blood, adjust dose, or pause a compound.
Patterns never fix themselves — they escalate.
TOOLS I USE:
Excel / Google Sheets for automatic mg/week math
Apple Numbers on mobile for logging on the go
WHOOP or Garmin for HRV, sleep, RHR trends
Withings BP cuff for daily readings
DEXA every 90 days for composition tracking
Your cycle isn’t a game — it’s a controlled experiment on your endocrine system.
Everyone reacts differently, and odds are you’re not under medical supervision.
If something goes sideways, these records can literally save you — and show your doc you weren’t just freelancing with hormones.
Attached below:
👉 My actual 7-day daily tracker (pins, orals, peptides, aminos etc.)
👉 My weekly cycle summary (auto-calculates mg/week and tracks bloodwork + compound changes)
These are the exact spreadsheets I’ve used for every cycle.
Use them, copy them, tweak them — just track.
Because memory lies, but data never gaslights you.
Bottom Line:
If you don’t track it, you’re not cycling — you’re gambling.
Every extra pin without data is just roulette with hormones.
Write it down, stay honest, and you’ll know whether it’s the gear, the grind, or your genetics doing the work.
Poll 👇
What’s your weakest discipline when running a cycle?
1️⃣ Forgetting to log pins
2️⃣ Skipping bloodwork
3️⃣ Changing doses mid-week
4️⃣ Losing track of injection sites


MAAS-6
#MarkoAASGuide #TRTPrep #PEDLongevity
The Lifestyle — aka: The part that makes you boring at parties but alive in your 60s.
Ask my buddy @Ironhands57 – he’s in full contest prep and he’s a disciplined 8th degree Cali-meet-monk.
Gear works. But gear + sloppy lifestyle = 🚑 faster than you can say “bro science.” If you’re running AAS, your life outside the pin must be dialed in:
Alcohol / Smoking / Partying:
• Booze + orals = liver waving a white flag
• Nicotine wrecks vascular health (your #1 weak link)
• Party drugs + AAS = ER roulette (BP spikes, serotonin storm, arrhythmias)
N=1: I quite alcohol in my late 40s. Best decision I ever made. I wonder where’d I’d be today if I’d never started that stupid habit in my teens
Sleep:
• Recovery = growth. Period.
• 7–9 hrs is non-negotiable
• If you snore like a chainsaw, CPAP/BiPAP isn’t optional — it’s survival
N=1: I’m on BiPAP nightly. Without it, my sleep architecture is trash and my recovery tanks.
Diet:
• High-quality protein, healthy fats, micronutrients
• Fiber for heart & gut health
• Junk in = junk labs, plaque, insulin resistance
N=1: I’m strict — celiac, so no gluten. Daily magnesium, omega-3s, curcumin (you saw my stack in MAAS 5). I eat clean, and I track labs every 4 weeks to make sure food + gear aren’t wrecking me.
Travel:
• Breaks routines, crushes sleep
• Plan meals, meds, and gym time in advance
• Hydrate like your kidneys depend on it (because they do)
N=1: Business travel kills rhythm. I bring pins/gear, supplements, and a gym-plan — otherwise recovery nosedives.
Discipline & Routines:
• Consistency > motivation
• Same time for training, meals, and sleep → your body thrives on rhythm
N=1: I live on routine. Without it, AAS + work stress + family = chaos.
Monitoring:
• Labs every 6–8 weeks = non-negotiable
• Bloods, BP, scans — otherwise you’re flying blind
• MAAS-4 was all about baselining; MAAS-6 is about discipline to keep testing
N=1: I pull labs every 4 weeks. It’s the only reason I’ve caught issues before they turned catastrophic.
Cardio:
• “Cardio kills gains” = clown take
• Your heart is the bottleneck, not your quads
• 3–5x/week, Zone 2 base. Add HIIT sparingly
N=1: 4-5 days a week, 30 mins Zone 2 on the bike. Heart health first — muscle means nothing if the pump fails.
Gym Time:
• Train hard, but train smart
• Match volume + intensity to your recovery (and gear)
• Tendons don’t grow as fast as muscles — ego lifting = injury
N=1: After training 2–4 RIR, I’ve shifted to training to failure on a hypertrophy program. Copious gear helps, but tendons and joints still lag. Physio Therapists do wonders for joints. Respect the weak links.
Bottom line:
AAS isn’t just about syringes — it’s about restructuring your life around recovery, discipline, and health. No supplement stack will save you from a reckless lifestyle.
Uncle Marko says: You don’t “party” on cycle. You live like a boring monk with big arms so you’re still flexing when the grandkids show up.
What’s your most monk-like discipline?
1. Meal prep on trips
2. 7-9hrs of sleep
3. ZERO alcohol/drugs
4. Zone 2 cardio




MAAS-5
#MarkoAASGuide #TRTPrep #Biohacking
Mitigation strategies — aka: How not to die while still flexing in the mirror.
We did fire-and-brimstone risks in MAAS-3.
We baselined in MAAS-4.
Now comes mitigation: supplements, OTC, and prescription meds that might keep your organs from rage-quitting while you’re on cycle (not Post Cycle).
⚠️ Reminder: Every person’s goals, genetics, labs, and cycles are different. This isn’t a prescription. It’s a menu. Pick what fits your data.
Supplements (easy adds):
• Omega-3s
• Vitamin D + K2
• Magnesium + Taurine
• Curcumin
• NAC
• CoQ10
• Garlic
• Fiber & probiotics
OTC tools:
• Electrolytes (Na / K / Mg)
• Blood pressure support (Carditone, hawthorn, etc.)
• Baby aspirin (case-by-case: clot vs bleed balance)
• Antihistamines / decongestants (if BP allows, for the Tren sleep zombies)
Prescription (doctor-supervised only):
• Telmisartan / ACEi (blood pressure & cardiac protection)
• Statins / ezetimibe (lipids if labs demand)
• Metformin (glucose control, longevity cred)
• Beta-blockers (arrhythmia insurance - Nebivolol)
• CPAP / BiPAP (sleep apnea warriors)
** talk to a doc (like @CoffeeBlackMD) or an expert consultant (like @BowTiedHRT) for individual tuning.
Mitigation ≠ Permission. It’s not a green light to abuse—it’s the parachute after you’ve already jumped.
My N=1 On-Cycle Stack (Age 61, July 2025)
This is my shield. Yours may (and should) look different depending on your labs, goals, and cycles. I have unique medical needs - a surgical kidney injury (from stones), celiac disease (which limits my nutrients), systemic inflation, and I'm older than dirt - my stack works for me. Your stack will necessarily be different.
Also - your supplement stack should be much different if you're just on TRT compared to 2.5g of gear with Halo and Tren sprinkled in for good measure.
Morning (fasted, pre-workout):
• Protein + creatine (50 g)
• Citri-Cal Slow Release (1200 mg)
• CoQH-CF Ubiquinol (500–600 mg)
• Amino-1MQ / NMN blend
• Vitamin C (500 mg)
• 9-ME-BC (2 caps)
• Taurine (1–2 g)
• Lumbrokinase (2 caps)
• Nattokinase (4 caps)
• L-Carnitine tartrate (3 g)
• TMG (5 g)
• Carditone (1 tab)
• Aged garlic (3 tabs)
• Copper (1 tab)
• ATP360 (3 caps)
• Flaxseed oil (1 tbsp)
• Libidon A-16 (2 caps)
• Pielotax A-9 (2 caps)
• Endoluten A-8 (2 caps)
• Alpha Lipoic Acid (2 caps)
Morning (post-workout):
• Whey protein isolate (50 g)
• Magnesium (1 g)
• Potassium (99 mg)
• Pink Himalayan salt (2 g)
• Glutathione IV push (weekly)
Morning (post-breakfast):
• Multivitamin (high quality)
• Vitamin E (400 IU)
• Zinc (30 mg)
• Iron (per labs)
• Vitamin C (1 g)
• Lactoferrin (250 mg)
• Copper (again)
• Fish oil (2–3 g)
• Curcumin (500 mg)
• Probiotic (1 cap)
Night (Tren sleep support):
• Magnesium glycinate (500 mg)
• Theanine (200 mg)
• Glycine (3 g)
• Apigenin (50 mg)
• Ashwagandha (600 mg)
• Melatonin (low dose, PRN)
• Gabapentin (300 mg)
• CPAP / BiPAP (nightly)
Mitigation ≠ Permission. This is my N=1 stack at age 61. Yours will look totally different.
The goal is simple: stay alive long enough to still be flexing when the grandkids show up.
What’s your non-negotiable side-effect shield?
Drop it below.
— Uncle Marko




MAAS-4
#MarkoAASGuide
Baselining: Getting your house in order!
#TRTPrep #PEDLongevity
Picture this: You're a 55+ AAS Goblin, pinning daily barrels of monkey juice, posting pics of those massive 15's... then BAM—bloods are in the RED. Weeks of freak-out ahead.
How do you know you’re not dealing with a pre-existing condition? Do you know your baseline lipids? Did you know your pre-cycle iron study results?
If you don’t get baselines on your health and body to use as comparisons – you will freak the f*%k out and blame everyone around you (except the man in the mirror) for letting you do AAS.
Uncle Marko lesson learned: Don’t start blind. Baseline everything you can afford on this list and keep records BEFORE your first pin. Trust me – you’ll thank yourself because you’ll know a pre-existing condition versus any of the AAS-induced health threats painfully listed in MASS-3.
Here’s a comprehensive list of tests and images for you to get while you’re on no more than modest TRT, or better yet, none at all. If you’re on more than 150–175 mg of test per week and it’s been 2 months, the skewing of numbers may have started. But if you could go back in time, you would get these control baselines:
Blood Panel:
Comprehensive Metabolic Panel - Kidney/liver function baseline to catch AAS strain early
Complete Blood Count
Iron Study
Cystatin C: gold standard for kidney function
Pancreas (Lipase and Amylase)
Liver Panel (enzymes including GGT) - Catch ‘orals’ damage early
Lipids (cholesterol, triglycerides, Lp(a), ApoB)
Immunoglobulins (IgG, IgA, IgM)
Thyroid (TSH, T4, T3)
A1C and fasting glucose
Reproductive hormones (FSH, SHBG, LH, Testosterone and Estradiol by LC/MS/MS)
Electrolytes
Heavy metals (only if you’ve had credible exposure)
Optional one-time baselines for future reference:
hs-CRP: inflammation and cardiovascular risk
Homocysteine: vascular and methylation marker
Fasting insulin: clarifies glucose/A1C
Prolactin: relevant when manipulating dopamine/AAS
IGF-1: marker of GH activity
DHEA-S & Pregnenolone: broader steroidogenesis view
Vitamin D, B12, Folate: common deficiencies with systemic effects
You can ask your PCP to order these (expect some pushback), or spend $300–$500 with online providers like Quest. There are services that bundle tests + interpretation for more money. Honestly – after a while you’ll know what things mean. I use ChatGPT to feed in a spreadsheet of my labs for interpretations and suggestions. Track everything in one spreadsheet.
Blood Pressure:
Buy a BP cuff (~$30) and measure properly – arm supported at heart level, seated quietly for 5 minutes, no crossed legs. Take morning and evening readings for a week to establish your baseline. Then, if three weeks into Test your BP is 145/97, you’ll know it’s the cycle kicking in and you need to mitigate.
CAC score:
The Coronary Artery Calcium (CAC) score is a CT of your heart arteries that gives an Agatston score plus an age/sex percentile. Hopefully your baseline is low (mine is 4 – very low risk, but a sign that soft plaque is present). AAS will disrupt lipids and may accelerate calcification. Get the baseline once (about $200) and consider repeating every 3–5 years if it will change your management – not yearly.
DEXA Scan:
DEXA (dual-energy X-ray absorptiometry) is low radiation, repeatable, and tracks fat, lean mass, and bone density with good precision. It’s far more reliable than the mirror test (“biceps vein at 18%” and “abs at 10%” are anecdotes, not universal rules). MRI can offer more precision, but DEXA is the affordable gold standard for body-comp tracking. Marko does a DEXA every 90-180 days.
Cardiac Imaging:
If you want LV size, aortic diameter, and ejection fraction, start with an echocardiogram. It’s radiation-free and widely available. Cardiac MRI offers even more detail for tissue and volumes. Coronary CT angiography with contrast is reserved for specific indications – not something to repeat annually.
Full-Body MRI Scan:
Prenuvo and similar companies offer full or partial body MRI scans. MRI is excellent for soft tissues (tumors, lesions, abnormalities), though it does not detect calcifications well (CT does). Full-body MRI as routine screening is controversial, but if you’re 50+, high-risk, or just want peace of mind, doing it once per decade is reasonable if you can afford it ($2000-$3000). Check if your HSA/FSA covers it – plans vary.
Cancer Markers:
Don’t waste money on broad annual tumor marker panels – they aren’t validated for screening and generate false positives. Stick to targeted markers based on risk (e.g., PSA for prostate cancer after discussion with your doctor). Remember, some cancers are androgen-driven – prostate is the classic example. And yes, castration was once used as a treatment for prostate cancer!
Did I miss anything @CoffeeBlackMD ? How about you @Dr_Red_Gamer ?
Bottom line:
Yes, it costs money. But the goal is biohacking for a longer, healthier life – not cutting it short because you didn’t know you had heart disease or cancer before you poured fuel on the fire with AAS. Baseline now, so when numbers change you’ll know whether it’s you or the gear.
Stop guessing. Test, measure, and then decide if that next pin is worth it.
What's your baseline win story for the N=1 section?



MAAS-3
#MarkoAASGuide
Dangers, Consequences, Side Effects (a.k..a: “Sides”):
This is going to be the least fun post I’m going to do in this series. But it’s THE MOST IMPORTANT one. The vast majority of you are unaware of the full list of consequences of doing AAS, so I’m going to squeeze this lemon in your eyes right now and hopefully wake you up a bit.
If you’re on TRT – Testosterone Replacement Therapy at between 100-200mgs per week – you’re on AAS. Period. End of discussion. You’re not loading up on gear for a pro card, but you are on THE fundamental base Anabolic Androgenic Steroid. And even at that dose a medical professional should be monitoring you because there are consequences and risks to even low dose TRT.
Here is an incomplete list of possible side effects in pinning anything from TRT all the way to crazed roid raged gorilla doses. READ IT and KNOW THE RISKS:
Cardiovascular:
Dyslipidemia: ↓HDL, ↑LDL, ↑total cholesterol
Atherosclerosis and plaque formation → coronary artery disease
Left ventricular hypertrophy (LVH) and cardiomyopathy
Aortic root dilation → ↑ risk of dissection with heavy lifting
Myocardial fibrosis and impaired contractility
Hypertension and fluid retention–driven strain
↑ Risk of arrhythmias (atrial fibrillation, ventricular tachycardia)
↑ Risk of sudden cardiac death
Polycythemia (↑RBC, Hct, Hb) → ↑ viscosity, clotting risk
↑ Homocysteine levels → thrombotic events
Endothelial dysfunction → loss of vascular elasticity
Hematologic:
Hypercoagulability → DVT, PE, stroke, MI
Paradoxical bleeding risk if platelets become dysfunctional
Iron dysregulation (↑RBC turnover, ↑ ferritin demands)
Immune / Inflammatory:
Both immunosuppressive (infection risk) and immunostimulatory (autoimmune flares) effects
↑ Systemic inflammation markers (CRP, IL-6, TNF-α)
Hepatic:
17-α-alkylated orals → hepatotoxicity, cholestasis, hepatic peliosis
Elevated liver enzymes (AST, ALT, GGT, ALP)
Jaundice, fibrosis, cirrhosis, rarely hepatocellular carcinoma
Renal / Electrolyte:
Sodium/water retention → edema, ↑BP
Direct nephrotoxicity (esp. high doses, orals, trenbolone, stanozolol)
↑ Risk of kidney stones and focal segmental glomerulosclerosis (FSGS)
Proteinuria and CKD progression
Musculoskeletal:
Acne, oily skin, sebaceous hyperplasia
Accelerated androgenic alopecia (male pattern baldness)
Premature epiphyseal closure in adolescents → stunted height
Tendon rupture (strength lag vs. hypertrophy + reduced elasticity)
Water retention → joint pain, edema
Gynecomastia (from aromatization)
Muscle cramps (electrolyte imbalance)
Male Reproductive:
Infertility (via HPG axis suppression)
Testicular atrophy (“shrinkage”)
Erectile dysfunction, reduced spermatogenesis
Gynecomastia (from estradiol or prolactin imbalance)
↑ Prostate volume → BPH symptoms (urinary obstruction)
↑ Risk of prostate cancer progression (debated, but mechanistically plausible)
Priapism (rare but dangerous)
Female Reproductive:
Virilization (clitoromegaly, hirsutism, voice deepening – permanent)
Menstrual cycle irregularities / amenorrhea
Breast atrophy
Infertility, teratogenic effects in pregnancy
Neurological / Psychological:
Aggression / irritability (“roid rage”)
Depression, anxiety, mood swings
Hypomania / mania-like states
Dependence / withdrawal syndromes
Insomnia
Cognitive effects (memory impairment, executive dysfunction with long-term use)
Neurotoxicity (oxidative stress, possible ↑ risk neurodegenerative disease)
Metabolic / Endocrine:
Insulin resistance, metabolic syndrome
Altered thyroid hormone metabolism (rare but reported)
Gynecomastia from aromatization (E2 excess)
Adrenal suppression if stacked with corticosteroids or prohormones
Pulmonary / Sleep:
Worsening of obstructive sleep apnea
↑ Risk of pulmonary embolism (via clotting changes)
Other / Rare:
Allergic reactions to excipients (sesame oil, benzyl alcohol, etc.)
Peliosis hepatis (blood-filled cysts in liver)
Rare reports: brain tumors, breast cancer (from estrogen conversion), kidney cancer
Severe acne → risk of bacterial superinfection
Nosebleeds (due to BP and vessel fragility)
Key takeaway:
Even at TRT, most of the risks are mild but still measurable (RBC ↑, HDL ↓, prostate/BP issues). At higher “blast” levels, the risks compound synergistically (cardiac remodeling + hypercoagulability + hypertension = catastrophic events in susceptible individuals).
Bottom Line, kids:
Listen to Uncle Marko....You’re playing with FIRE. And don’t engage in dismissive thinking ”But every medicine my doc gives me has sides and risk too!” You’re under medical supervision for that prescription. You can call them and see what to do next.
But if you’re secretly on 2g/wk of Test and Tren and A-Bombs, who you gonna call? And that’s not to mention the 6IU of HGH and the 37 different amino acid blends and peptide stacks, that clearly state on the label “NOT FOR FUCKING HUMAN USE”, that you inject every 3 hours.
Are you going to fess up to your doc that you’re basically juicing like a maniac and expect they need to do anything other than say ‘stop juicing like a maniac’? The minute you do reveal your protocols to a ‘normal’ doc, your life insurance policy will be cancelled, and you will never get a policy again.
It’s a rare doc, like @CoffeeBlackMD , or my own private pay physician, who wants the truth so they can address the most likely cause of the health symptoms you have. There are countermeasures and methods that you can employ to mitigate some/most of these issues (and we’ll discuss this in a future post). But having a solid medical expert in your court, someone you will likely have to pay cash for service, is worth every dime.
No point in getting that perfect body when an aortic dissection is waiting for you in the next 99 ass-to-grass squats.
Did you know there were this many possible health consequences to AAS?
Next post will be for the knuckle heads like me who pin gear and want to know what Marko does to mitigate these sides....

MAAS-2
#MarkoAASGuide
What are Anabolic Androgenic Steroids:
There are 4 pathways to getting jacked:
1. Mechanical Tension – from a properly designed, executed, and consistent resistance training program
2. Steroids – which are already present in your body (mainly in the form of testosterone, which is the most abundant steroid hormone found in both males and females)
3. HGH – which is already present in your body
4. PI3K – Which activates protein kinase B, the critical hub for muscle growth signaling.
I’d love to add food and protein, because it’s certainly involved, but without the 4 pathways above, you’d just get fat like I used to be.
Steroids, have a subcategory called Anabolic which means they promote muscle growth. Another category is Androgenic, which means they promote ‘male’ characteristics like a body hair growth, and a deep sounding voice. I am not going to speak about SARMs in these threads because SARMS are NOT AAS.
Testosterone is HIGHLY anabolic and androgenic. Estradiol is not strongly anabolic, but it supports an anabolic environment, and it is not androgenic.
AAS (anabolic–androgenic steroids) grow muscle through 3 main mechanisms:
· ↑ Protein Synthesis (Anabolic effect):
AAS bind to androgen receptors (AR) in muscle, activating pathways like PI3K–AKT–mTOR, which increase ribosome activity and drive new muscle protein formation.
· ↓ Protein Breakdown (Anti-catabolic effect):
They suppress catabolic regulators (like FoxO transcription factors, atrogin-1, MuRF1), reducing muscle protein degradation.
· ↑ Satellite Cell Activity (Muscle Remodeling):
AAS stimulate satellite cells (muscle stem cells) to proliferate and fuse with existing fibers, donating nuclei → enabling larger muscle fibers (hypertrophy) and better recovery.
Here is when I had an early epiphany from researching this entire topic:
Look at the first photo of the testosterone molecule: 4 carbon rings, with some atoms attached (so what?).
Now look at the Trenbolone (The vaunted “Dragon” of steroids) molecule: 4 carbon rings, same general structure. Couple of tweaks.
EVERY AAS is a derivative of the human testosterone molecule, a bio-identical synthetic version of which was lab produced for the first time in 1935, with a Nobel Prize in Chemistry awarded to a German and a Swiss scientist in 1939. The first lab produced AAS - synthetic bio-identical testosterone, was in 1935!
This fact dispelled my pre-conception that ‘steroids’ were some new unique dark creations, the structures of which were secretly concocted in someone’s toilet by a jock with a high school chemistry background. The truth is that AAS had a 50-year period of discovery and synthesis from big pharma, by tweaking the testosterone base molecule, and used by medical professionals for a variety of health reasons and diseases. But later in the 80's, vilified by politicians and media because of unfair “sports” advantages. Oddly enough, I believe Turinabol, invented by the GDR in 1962, was the only AAS ever developed solely for performance enhancements in sports.
This is when I went from TRT pellets inserted in my glutes, to testosterone injections and soon after adding in and trying different combinations of nandrolone, primobolan, masteron, trenbolone, anavar, halo, anadrol, dianabol, turinabol, etc….
I just wasn’t afraid of it anymore. It’s playing with fire for sure, but it’s not nuclear waste either.
Did you know that every AAS is just a testosterone molecule with a few unique tweaks?


MAAS-1
#MarkoAASGuide
A FOREWARD to these next 30-40 AAS related posts:
· These posts will take a long time to create and publish. Be patient with me. I have kids and a full-time job.
· There will be a hashtag #MarkoAASGuide that you can use to search on all of them.
· Each Post will be uniquely numbered with MAAS-# so you can go right to a specific topic. If there are sub posts, they will be numbered as MAAS-#.#. The Testosterone posts will take 3-4 posts. So MAAS-#.1, MAAS-#.2,…
· I will pin this in my profile.
· There’s a chance that I will publish something incorrect – it is not my intention to do so, and I will update and republish based on a credible follower providing a professional citation that refutes what I’m saying…but…
· Bro Science, and N=Marko is real too and it sometimes defies the research.
· I’m NOT a source and I am NOT shilling for sources. Where I’ve used a brand I know works, and I mention it, do your own research. I will ignore DMs requesting access to sources.
*** DISCLAIMER: I am NOT a scientist or medical professional. I’m doing this to bring some information to the community that you can use to do your own research. AND I’m all about risk reduction. If you go against the consensus of medical professionals, you’ll likely be on your own, and so maybe some risk reduction protocols can help you prevent a big consequence. This is just summarizing information that takes time to learn for education and entertainment purposes only. DO NOT PIN OR POP GEAR - your junk will fall off and your heart will explode. This disclaimer applies to all of the MAAS series.
And so it begins... Are you ready?
Last Seen Hashtags on Sotwe
Most Popular Users

Elon Musk 
@elonmusk
240.2M followers

Barack Obama
@barackobama
119.3M followers

Donald J. Trump
@realdonaldtrump
111.6M followers

Cristiano Ronaldo
@cristiano
109.3M followers

Narendra Modi
@narendramodi
106.9M followers

Rihanna
@rihanna
97.4M followers

NASA
@nasa
92.1M followers

Justin Bieber
@justinbieber
90.6M followers

KATY PERRY
@katyperry
87M followers

Taylor Swift
@taylorswift13
80.8M followers

Lady Gaga
@ladygaga
72.4M followers

Kim Kardashian
@kimkardashian
69.5M followers

Virat Kohli
@imvkohli
68.9M followers

YouTube
@youtube
68.6M followers

Bill Gates
@billgates
63.5M followers

The Ellen Show
@theellenshow
62.5M followers

CNN
@cnn
61.9M followers

Neymar Jr
@neymarjr
61.5M followers

X
@x
60.9M followers

Selena Gomez
@selenagomez
60.1M followers