Gastroenterólogo, con interés en enfermedad inflamatoria, cápsula endoscópica y enteroscopía. Editor Principal de la Revista de Gastroenterología del Perú
Vonoprazan-Tetracycline dual therapy achieved non-inferior H. pylori eradication vs. bismuth quadruple therapy, with markedly fewer adverse events. Click the link to read the full article:
🔗 https://t.co/dL0GhscMqY
Interception Vs Primary Prevention in #IBD
Consider: scalability , practicality , bang for the buck , cost , global impact
Please debate this : we thought long and hard before this 👇 paper
JAKs may have ⬇️risk of serious infections that previously thought compared to TNFs. Could it be related to more rapid 🔥 control or JAKs safer in IBD population as we suspected after ORAL trial?
¿Es posible tener síntomas de diarrea después de una cirugía de vesícula biliar?
La respuesta es sí: se llama diarrea por malabsorción de ácidos biliares (MAB) y es más frecuente de lo que pensamos.
💜✨ Día Mundial de la EII ✨💜
No te acostumbres a vivir mal.
Dolor, diarrea, sangrado o cansancio constante NO son normales. 🚨
La Enfermedad Inflamatoria Intestinal puede afectar el día a día, pero con diagnóstico y tratamiento adecuados, se puede volver a vivir con libertad.
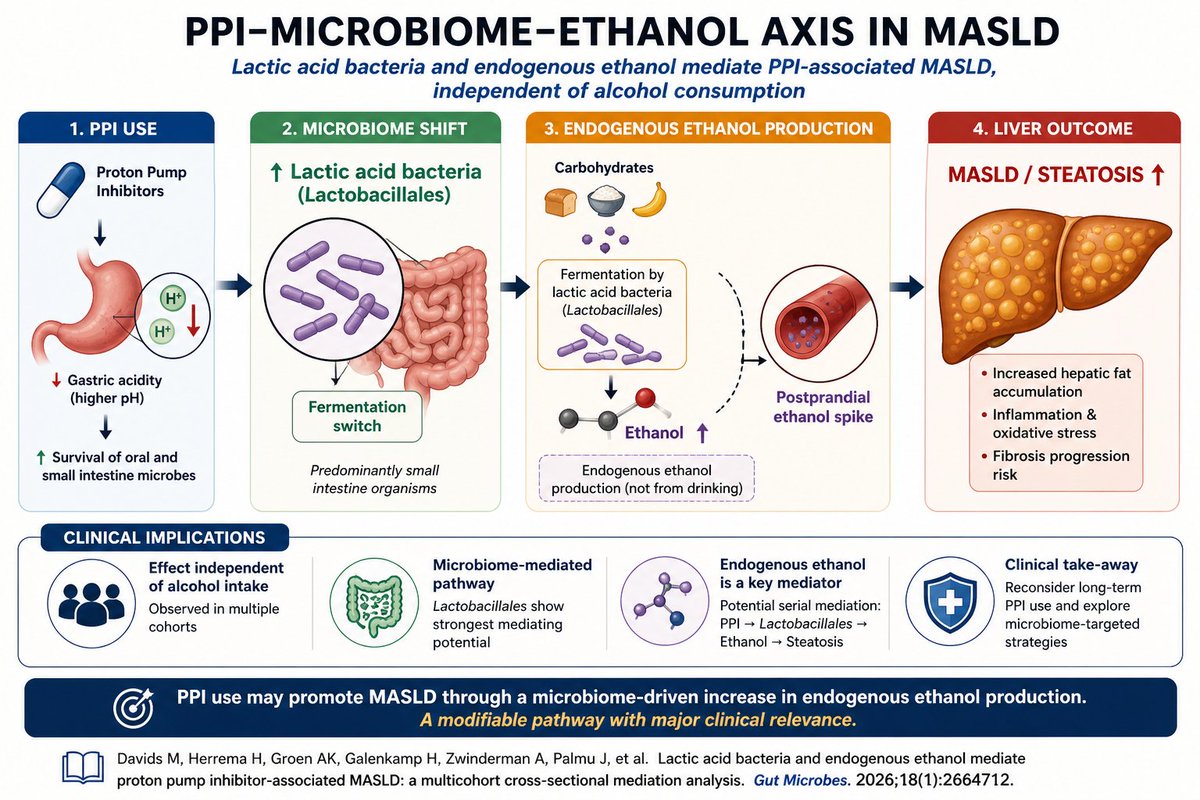
Fascinating study with real clinical implications:
PPIs → altered microbiome → ↑ endogenous ethanol → MASLD
Time to rethink long-term PPI use in patients with MASLD?
📢 ¡Artículo de acceso gratuito en nuestra revista 'Gastroenterología y Hepatología'!
📕Nuevo "Documento de consenso sobre el diagnóstico, manejo y tratamiento de la infección crónica por el virus de la #hepatitisB y por el virus de la #hepatitisD en España".
🔎Coordinado por @SaSi_Lens. Accede aquí: ➡️ https://t.co/C7ttGjdsIa
“Semaglutide shifts MASH therapy from glycemic control to multi-organ disease modification—but fibrosis still demands time and combination strategy.”
Semaglutide in MASH with F2–F3 Fibrosis (ESSENCE Trial Perspective)
🔬
MASH with F2–F3 fibrosis represents a critical therapeutic window, where timely intervention can prevent progression to cirrhosis, HCC, and liver-related mortality.
💉 Semaglutide: Disease-Modifying Potential
Once-weekly semaglutide 2.4 mg demonstrates true disease-modifying signals, not just metabolic improvement.
🧠 Histological Efficacy (Key Takeaway)
Semaglutide significantly increases:
Resolution of steatohepatitis without worsening fibrosis (~2/3 vs ~1/3 placebo)
≥1-stage fibrosis improvement (~1/3 vs ~1/5 placebo)
👉 Number needed to treat (NNT):
~3–4 for MASH resolution
~6–8 for fibrosis improvement
⚖️ Weight Loss: The Central Driver
Semaglutide induces ~10–11% weight loss vs ~2% with placebo, a threshold strongly linked to:
MASH resolution
Fibrosis regression
👉 ≥10% weight loss remains a biological pivot point in MASLD management.
❤️ Cardiometabolic Amplification
Semaglutide delivers multi-organ protection, including:
HbA1c reduction
Blood pressure lowering
Improved lipid profile
Reduced inflammatory markers (hs-CRP)
👉 Important: Cardiovascular disease remains the leading cause of mortality in MASLD.
🧪 Non-Invasive Markers Align with Histology
Consistent improvements seen in:
ELF score
VCTE (FibroScan stiffness)
PRO-C3
FAST score
ALT/AST
👉 This supports a future biopsy-sparing strategy in MASH monitoring.
⚙️ Mechanistic Insight (Very Important)
Semaglutide works via dual pathways:
Weight-dependent effects (dominant)
Reduced caloric intake
Improved insulin sensitivity
Reduced adipose inflammation
Weight-independent (partial)
Anti-inflammatory pathways
Gut–liver axis modulation
👉 However:
GLP-1 receptors are not expressed in hepatocytes, suggesting indirect hepatic benefits.
⚠️ Fibrosis: The Hard Endpoint
Fibrosis improvement is:
Slower and less weight-dependent
Likely requires longer duration and targeted antifibrotic pathways
👉 Cirrhosis (F4) shows limited reversibility with semaglutide alone.
🛡️ Safety Profile
GI side effects (nausea, vomiting) are common but transient
No major hepatotoxicity signal
Similar serious adverse events vs placebo
👉 Caution:
Gallbladder disease
Rare pancreatitis
🔄 Therapeutic Positioning
Semaglutide is best suited for:
Obese / T2DM phenotype MASH (commonest in India)
High cardiometabolic risk patients
🔬 Future Strategy: Combination Therapy
Semaglutide (systemic metabolic drug) + Resmetirom (liver-directed THR-β agonist) offers:
Upstream metabolic unloading + direct hepatic antifibrotic action
👉 Likely future paradigm:
Multi-target therapy for MASLD
❗ Clinical Gaps
Long-term outcomes (cirrhosis, HCC, mortality) not yet confirmed
Limited data in:
Lean MASH
Diverse ethnic populations
Need for omics-based patient stratification
🔴 CME INDIA key point
“Semaglutide shifts MASH therapy from glycemic control to multi-organ disease modification—but fibrosis still demands time and combination strategy.”
📚 Key Reference
Pirola CJ, Sookoian S. Semaglutide in MASH with F2–F3 fibrosis: ESSENCE phase 3 perspective. Metab Target Organ Damage. 2026.
https://t.co/KG024CiBtF
Should GLP-1s be held before endoscopy? The OCULUS trial provides prospective data. 🛑
Continuing GLP-1 ⬆️ risk of clinically significant residual gastric volume (25.0% vs 3.1%). Key finding: a clear liquid diet 24h prior mitigated this risk.
🔗 https://t.co/f2fnOphXAS
☔ #BavenoVIII teasers on the EASL #TalkLiverToMe podcast
I ask @MattiasMandorf1 & Cristina Ripoll about...
🟦cACLD & the big picture
🟦Non-invasive tests
🟦First decompensation
🟦Quick-fire updates on variceal bleeding
🎧Spotify, Apple & EASL Campus:
https://t.co/mMCkjTDoqR