#acc26 Six reasons why CHAMPION AF should not change oral anticoagulation for AF
I will have a formal post up on @theheartorg but here is a short summary
1) Stroke and Ischemic Stroke went the wrong way.
All S -> 33 vs 50 [HR 1.46 95% CI, 0.94-2.27)]
IS -> 27 vs 45; [HR = 1.61; 95% CI, 1.00-2.59)]
Look at those upper-bounds.
2) NI would not have been met for efficacy had they used a margin with both rate ratio and risk difference, which is standard practice.
The margin of 4.8% is based on event rates at 12%, which is 1.4 in relative terms (40% higher). But when event rates come in lower, as they did: 4.8% vs 5.7%, the 4.8% margin is too lenient.
The 0.9% higher rate of the primary endpoint has a 95% CI of (-0.8-2.6%), so 2.6% is less than the margin of 4.8%. Now do it with relative risk.
It's in table 2. The relative risk is 1.20. The 95% confidence intervals were 0.87-1.66. Note that 1.66> 1.40 so LAAC is not noninferior based on rate ratio margins
3) The primary safety endpoint is flawed because it excludes periprocedural bleeding and uses nonmajor bleeds, such as gum bleeds and bruising. It's open label trial so who which group will complain of more nonmajor bleeding?
4) When counting all events, Watchman barely reduced major bleeds. Also in the main results table is that major bleeds were 83 vs 87 (5.5% vs 5.8%; HR 0.92 95% CI 0.68-1.24)
5) Net Clinical Benefit was also flawed because they used nonprocedural bleeding and nonmajor bleeds.
A normal patient would simply say, there were 17 more strokes and only 4 less bleeds. Hardly a good trade.
6) Bayes: trials don't give answers, they update priors. For Watchman, you have PREVAIL failing against warfarin, CLOSURE AF clearly failing against best med Rx (mostly DOACs) so priors are pessimistic. To go from pessimistic priors to enthusiastic posteriors you'd need hugely positive data. CHAMPION is not that.
Don't believe the stories that CLOSURE failed due to them using other LAAC devices. In the AMULET IDE trial, Watchman and Amulet were similar. Also, if you believe that German operators are worse than US authors, you need to travel more.
Conclusion: Oral anticoagulation for AF is one of the most evidence-based practices in all of medicine. To upend that would take much stronger data.
Don't be bamboozled by this trial, which was designed to be positive before the first patient was enrolled.
#ACC2026
Did you hear? Our electrophysiology team at the Sandra Atlas Bass Heart Hospital at North Shore University Hospital was the first in the world to implant the smallest diameter defibrillation lead to help treat potentially life-threatening abnormal heart rhythms. 🌎🫀👏
🔗: https://t.co/uaSdHaI38g
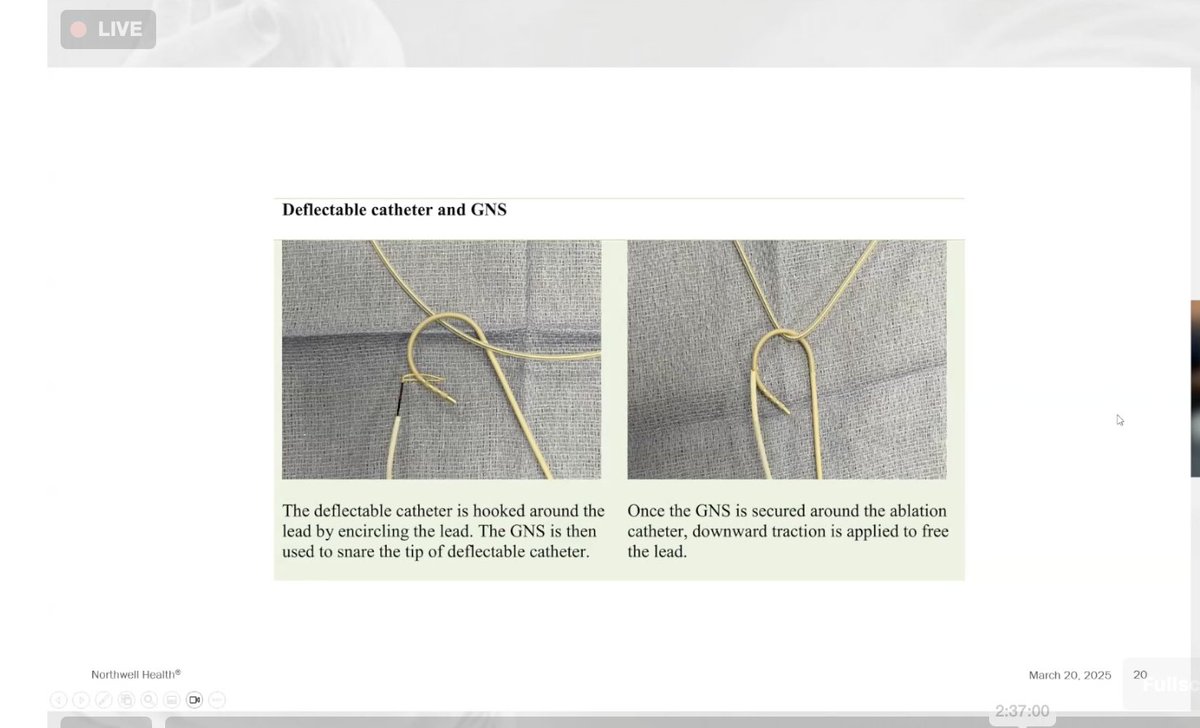
First commercial implant of an OmniaSecure lead in the world by Dr Larry Epstein @NorthwellHealth! Pt with CHB with PPM CM and VT. Upgraded to BiV ICD but unable to program around phrenic stim. LV lead and ICD removed and OmniaSecure lead placed. Beautiful result! @Medtronic
@News12LI
Two people trying to break into cars at valley stream around 1:48am this morning. You can see the second person in the top corner of the video on the next block.
AF is a poor marker in ACS. In our latest paper, AF was present in 25% of ACS patients, 50% of which is newly diagnosed, and increased risk of bleeding, in-hospital and post discharge mortality. @NorthwellHealth#epeeps#AFIB#cardiology#MI#ACS
https://t.co/lOnpkkOAnC
In-hospital Outcomes and Post Discharge Mortality in Patients with Acute Coronary Syndrome and Atrial Fibrillation
@keepinrhythm, @kcole_12, @hisbundle
https://t.co/Q6nJvxlO0o
@GeoRebekah Correct. But it is historically used to designate North/South geographically. So one could make the argument it’s geographically considered south.